 |
Case Series
Myositis and osteomyelitis due to radiotherapy-related fistulae in locally advanced cervical cancer
1 Resident of Medical Oncology Department, Hospital Virgen de la Salud, Toledo, Spain
2 Resident of Internal Medicine Department, Hospital Virgen de la Salud, Toledo, Spain
3 Nephrologist of Nephrology Department, Hospital Virgen de la Salud, Toledo, Spain
4 Oncologist of Medical Oncology Department, Hospital Virgen de la Salud, Toledo, Spain
5 Oncologist Head of Department of Medical Oncology Department, Hospital Virgen de la Salud, Toledo, Spain
Address correspondence to:
Miguel Borregón Rivilla
Calle Fuenterrabía, nº4, piso 6º centro izquierda, Madrid 28014,
Spain
Message to Corresponding Author
Article ID: 100051Z08MR2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Borregón Rivilla M, Serrano Romero de Ávila V, Acevedo Ribó M, Cárdenas JD, Chacón López-Muñiz JI, Esteban Esteban C. Myositis and osteomyelitis due to radiotherapy-related fistulae in locally advanced cervical cancer. J Case Rep Images Obstet Gynecol 2019;5:100051Z08MR2019.ABSTRACT
Enteric and urinary fistulae secondary to chemoradiation for carcinoma of the uterine cervix are devastating uncommon conditions with a significant impact in quality of life. They can also originate multiple disturbances and complications, mainly recurrent infections. We present two women with locally advanced cervical cancer treated with radiation who presented myositis and osteomyelitis secondary to pelvic infections due to radiation-induced fistulae. Recognizing and managing these complications need a high level of suspicion. Treatment is based on a multimodal approach which includes antimicrobial therapy, nutritional support, and surgical intervention. Revision of the literature is presented.
Keywords: Cervical cancer survivors, Myositis, Osteomyelitis, Pelvic sepsis, Radiation-induced fistulae, Secondary amyloidosis
Introduction
Some of the major causes of morbidity and mortality in locally advanced cervical cancer survivors are derived directly or indirectly from late toxic effects of their treatments. Radiotherapy-related enteric-urinaryvaginal fistulae are not common, but they strongly affect quality of life and can lead to severe medical conditions, such as recurrent infections. We present two women with locally advanced cervical cancer who developed myositis and osteomyelitis from pelvic infections secondary to radiotherapy-related fistulae.
CASE SERIES
Case 1
A 74-year-old woman with past medical history of hypertension, hypercholesterolemia, and obesity was diagnosed in 1996 of locally advanced stage III squamous cervical cancer with myometrium and lower third vaginal involvement. She received external beam radiotherapy 50 Gy to the pelvis with partial response, followed by radical hysterectomy, and internal brachytherapy with Caesium-137 (30 Gy).
In 2014, 18 years after these treatments, and with no evidence of malignant relapse, the patient complained of vaginal flow leakage and pelvic pain. She was diagnosed by pelvic examination and image studies of vaginal introit necrosis and vesicovaginal fistula. Then, she started suffering recurrent urinary tract infections and finally needed hospital admission due to a severe pelvic infection.
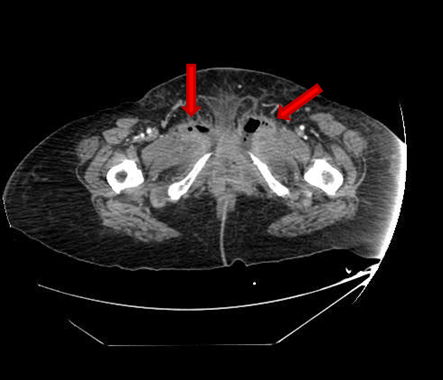
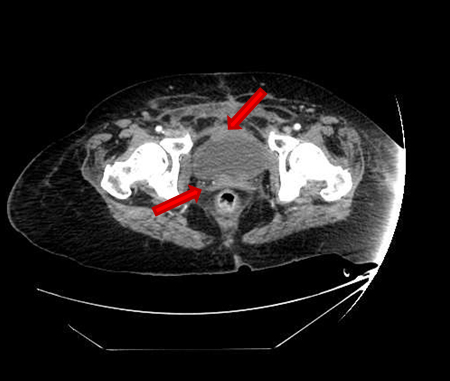
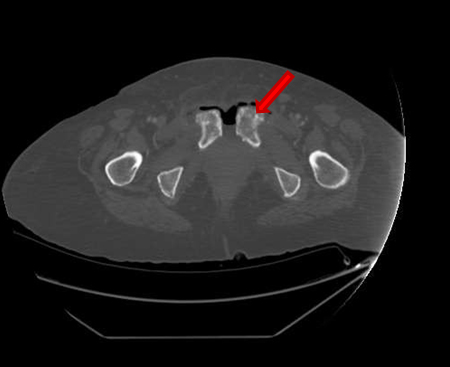
She presented on Emergency room suffering from fever, pelvic pain, and functional impairment of her right lower limb. Physical examination revealed bad smell vaginal flow and loss of strength on her right lower limb. Contrast computerized tomography and magnetic resonance images showed pelvic muscles impairment (Figure 1), inflamed bladder (Figure 2), and pelvic abscess lying from right psoas muscle to pubis bone, which presented radiologic signs of osteomyelitis (Figure 3) and (Figure 4).
Blood tests revealed moderate lymphocytosis, moderate elevation of C reactive protein, and mild normochromic and normocytic anemia. Urine, vaginal flow, and pelvic flow cultures demonstrated polymicrobial infection by Enterococcus faecalis and Bacteroides fragilis. Long antimicrobial therapy with Meropenem and Amoxicillin and bilateral nephrostomy were necessary to achieve infectious control.
Few months later, the patient developed secondary amyloidosis related to her chronic inflammatory status, with associated nephrotic syndrome unresponsive to conservative treatment, so renal replacement treatment with hemodialysis became necessary. The patient finally died four years later, because of progressive impairment of her performance status after several hospital admissions due to recurrent urinary tract and pelvic infections, the last one complicated with septic shock by Pseudomonas aeruginosa.
Case 2
A 33-year-old woman, active smoker, with chronic hepatitis B infection was diagnosed in 2016 of locally advanced stage IVA squamous cervical cancer because of bladder wall invasion and secondary obstructive uropathy, requiring bilateral nephrostomy diversion. A laparoscopic retroperitoneal and pelvic lymphadenectomy was performed. Twenty para-aortic and pelvic lymph nodes were resected and studied, with no infiltration on histology examination. Then, she received concurrent chemoradiotherapy: external beam radiotherapy with conformed intensity modulated radiotherapy (IMRT) to a total dose of 45 Gy to the pelvis and a boost to a total dose of 53 Gy to the primary tumor, concomitant with six weekly doses of Cisplatin 40 mg/m2 and posterior intrauterine high dose rate brachytherapy (6 Gy). Acute toxicity was mild and consisted in grade 1–2 hematologic and gastrointestinal toxicity.
Six months after finishing the multimodal treatment, persistent cervical malignant tumor was suggested by gynecologic examination, transvaginal ultrasound, magnetic resonance image, and positron emission tomography, so she underwent radical hysterectomy. The biopsy specimen showed microscopical focus of microinvasive and in situ carcinoma with free margins.
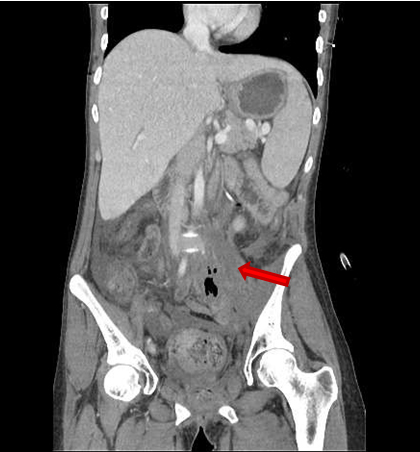
One month after surgery, late toxicity came up, with three consecutive radiation related fistulae (Figure 5), (Figure 6) and (Figure 7). Vesicovaginal and rectovaginal fistulae caused recurrent urinary tract and vaginal infections and abdominal pain, and required intravenous antibiotic therapy, nutritional replacement, and diversion colostomy. A further third fistula connecting the small intestine with the cloaca formed by the bladder, rectum, and vagina complex required an ulterior terminal diversion ileostomy. There was no evidence of relapse on image test or biopsy specimens.
Ten months later, she presented on Emergency room suffering from fever and left inguinal pain due to abdominal sepsis. Physical examination did not reveal any significant alteration. Blood tests demonstrated moderate lymphocytosis and moderate elevation of C reactive protein. Contrast computerized tomography showed a mass located in left psoas muscle, which was described as possible recurrent malignant mass versus infectious abscess (Figure 8). Biopsy by computer scan image was attempted, with not conclusive pathologic or microbiology results, so she received empirical antibiotic therapy. She also required intensive medical and nutritional support because of chronic diarrhea and electrolyte abnormalities.
During her hospitalization time, she presented sudden and massive vaginal bleeding that caused hemorrhagic shock requiring Intensive Care Unit admission, strong hemodynamic support, blood transfusions, and uterine right artery embolization. Once recovered, she developed severe pain and inflammation on her left thigh. Femoral magnetic resonance image revealed significant signal alteration of femoral diaphysis, with cortical disruption and muscle edema, suggesting femoral osteomyelitis originated from adjacent infected soft tissues (Figure 9) and (Figure 10).
Then, the patient went under surgery for soft tissues washing, drainage, and bone biopsy. Microbiologic cultures revealed Enterococcus raffinosus and Bacteroides thetaiotaomicron infection, so four weeks pathogen-directed antibiotic therapy with Linezolid and Metronidazole was prescribed for symptoms relief. Multifactorial progressive and severe renal impairment was developed and it was not reversible despite conservative measures. Bone biopsy was positive for squamous carcinoma metastasis.
She was finally discharged from hospital long admission. She has a good performance status despite her metastatic bone relapse, but she can not receive a new chemotherapy line due to her severe renal impairment, so she is being followed by Palliative Care Unit.






Discussion
External bean radiotherapy with concomitant Cisplatin chemotherapy plus intracavitary brachytherapy is standard of care for locally advanced cervical cancer, achieving local control rates of 60–70% and 67–80% five-year overall survival [1],[2],[3]. There is no standard treatment for residual cervical carcinoma after chemoradiation. Adjuvant hysterectomy or pelvic exenteration seems to improve local control and overall survival, at the expense of increasing late morbidity [4],[5].
Late toxicity of pelvic chemoradiation for cervical cancer remains to be fully quantified. Several systematic reviews and meta-analyses which have evaluated chemoradiotherapy cervical cancer trials conclude uniformly that there is insufficient data available to assess long-term morbidity of this therapeutic approach [2],[6],[7],[8]. Several authors reported an incidence of significant late toxicity after chemoradiation of cancer of the uterine cervix around 16–18%, basically, bowel and urinary complications [9],[10].
Enteric, urinary, and vaginal fistulae in patients irradiated for cancer of the uterine cervix are a feared complication. They are not common, especially when modern radiotherapy techniques are employed, but the real incidence can be under reported. Most of them occur between sigmoid colon or rectum and vagina, or bladder and vagina, and they can appear few months or years after finishing chemoradiation [11].
Factors identified as possible contributors of radiotherapy-related late toxicity include multimodal treatment, Cobalt radiotherapy, higher total dose of radiation and dose per fraction, larger radiation field (which implies advanced disease stage), medical comorbidities (particularly cardiovascular disease), smoking, low body mass index, persistent or relapsed disease, antiangiogenic therapy with Bevacizumab, and abdominal surgery (which may lead to a reduction in the blood supply to pelvic organs and/or bowel adhesions) [8], [12],[13],[14],[15]. Conformational intensity modulated radiotherapy (IMRT) delivers standard dose to the uterus while decreasing the dose to the critical organs (rectum, small bowel, and bladder) and has become widely accepted in developed countries as therapy of choice associated to high dose rate brachytherapy. However, many concerns remain about its real impact on survival and homogeneity between centers [16].
Symptoms of pelvic fistulae include vaginal passage of flatus and leakage of stool from the rectum to bladder and vagina, and recurrent urinary tract and pelvic infections. They also can originate significant emotional, social, and sexual disturbances as well as impairment of healthrelated quality of life and threatening consequences. Ruling out persistent or recurrent disease when it happens is advisable in order to select the best therapeutic approach for the patient.
We present two patients who complained of typical fistulae symptoms, such as flow leakage and pelvic pain, and developed recurrent urinary tract and pelvic infections. The relevance of these two cases is that these infections led to more severe complications with myositis and osteomyelitis and profound renal function impairment. One of the patients remained in complete remission, whereas the other one had concomitant bone metastasis. They supposed serious medical conditions that led to a significant impairment in their quality of life, requiring long hospital admission and invasive procedures. Ruling out the presence of active primary tumor was also a challenge.
Myositis and osteomyelitis are uncommon infections in this setting, but they have been previously described in prostate cancer survivors after surgery or radiotherapy. Inflammatory markers and pelvic magnetic resonance image contributed to the diagnosis. Nutritional support, specific antibiotic therapy, and surgical procedures were used in most cases, requiring cystectomy or urinary/fecal diversion, with or without surgical debridement [17].
Optimal management of radiation-induced fistulae is an unmet need and must be tailored to the individual patient. Restorative surgery in selected cases can relieve pelvic symptoms, but in many circumstances this procedure is difficult. Pelvic organs can be matted together with no natural planes, making resection hazardous and many patients require debridement because of tissue necrosis and presence of septic collections. Non-muscle flaps-based repairs have a high recurrence rate and most patients end up requiring permanent urinary or fecal diversion procedures to palliate symptoms and prevent recurrent infections. In selected cases, vascularized muscle advanced techniques can be used in well experimented centers.
Long-term complications of fistula repair include persistent urinary incontinence, fistula recurrence, anastomotic leak, pelvic or abdominal abscess, and intestinal obstruction. Multiple factors contribute to these poor results, including insufficient viable tissue for interposition, lack of adequate vascularity, and impaired healing. Surgical outcome is also related to the general condition of the patient and presence of malignant disease. Permanent enteric or urinary diversion can be followed by spontaneous closure of the fistula in a small percentage of patients previously irradiated, and prevents progression of symptoms, such as pelvic pain, diarrhea, and rectal ulceration [18],[19],[20],[21],[22],[23].
The two patients we present suffered from devastating late radiation toxicity that led to a significant impairment in their health-related quality of life, as well as a negative impact on their probability of survival. Myositis and osteomyelitis due to contiguous spread of abdominal infections secondary to radiation-induced fistula complication can be difficult to recognize if it is not suspected. Patients with intermittent urinary tract infections, abdominal pain, lower limb swelling, malaise, and impaired performance status can suffer underlying pubic or femoral osteomyelitis from contiguous unresolved infection. Surgical approach may be necessary to obtain microbial cultures and debridement.
Surveillance of patients with cervical cancer treated with chemoradiation intends to identify patients with isolated relapse amenable to curative salvage therapy as well as recognizing and managing long-term toxicity, in order to provide patients adequate medical and psychological support.
Although severe consequences are rare, some reports suggest that 20–50% of patients with cancer of the uterine cervix may experience long-term adverse events derived from their treatments that interfere to a greater or lesser extent with their daily life. Many times, patients suggest that their specialist clinicians undervalue their symptoms and do not offer adequate measures to alleviate them or prevent worsening [24]. Late severe radiationinduced toxicity can be threatening and devastating. Unfortunately, optimal management of these serious complications is far from being satisfactory.
Conclusion
Enteric, urinary, and vaginal fistulae in patients irradiated for cancer of the uterine cervix are not common but feared complication that can be threatening. The relevance of the two cases we present is that their fistulae led to severe infections such as myositis and osteomyelitis and profound renal function impairment, with devastating impact on their life quality and probability of survival.
REFERENCES
1.
Thomas GM. Improved treatment for cervical cancer—concurrent chemotherapy and radiotherapy. N Engl J Med 1999;340(15):1198–200. [CrossRef]
[Pubmed]

2.
Green J, Kirwan J, Tierney J, et al. Concomitant chemotherapy and radiation therapy for cancer of the uterine cervix. Cochrane Database Syst Rev 2005;(3):CD002225. [CrossRef]
[Pubmed]
3.
Eifel PJ, Winter K, Morris M, et al. Pelvic irradiation with concurrent chemotherapy versus pelvic and para-aortic irradiation for high-risk cervical cancer: An update of radiation therapy oncology group trial (RTOG) 90-01. J Clin Oncol 2004;22(5):872–80. [CrossRef]
[Pubmed]
4.
Hass P, Eggemann H, Costa SD, Ignatov A. Adjuvant hysterectomy after radiochemotherapy for locally advanced cervical cancer. Strahlenther Onkol 2017;193(12):1048–55. [CrossRef]
[Pubmed]
5.
Ota T, Takeshima N, Tabata T, Hasumi K, Takizawa K. Adjuvant hysterectomy for treatment of residual disease in patients with cervical cancer treated with radiation therapy. Br J Cancer 2008;99(8):1216–20. [CrossRef]
[Pubmed]
6.
Chemoradiotherapy for Cervical Cancer Meta-analysis Collaboration (CCCMAC). Reducing uncertainties about the effects of chemoradiotherapy for cervical cancer: Individual patient data meta-analysis. Cochrane Database Syst Rev 2010;(1):CD008285. [CrossRef]
[Pubmed]
7.
Kirwan JM, Symonds P, Green JA, Tierney J, Collingwood M, Williams CJ. A systematic review of acute and late toxicity of concomitant chemoradiation for cervical cancer. Radiother Oncol 2003;68(3):217–26. [CrossRef]
[Pubmed]
8.
Güth U, Hadwin RJ, Schötzau A, McCormack M. Clinical outcomes and patterns of severe late toxicity in the era of chemo-radiation for cervical cancer. Arch Gynecol Obstet 2012;285(6):1703–11. [CrossRef]
[Pubmed]
9.
Tan LT, Zahra M. Long-term survival and late toxicity after chemoradiotherapy for cervical cancer – the Addenbrooke's experience. Clin Oncol (R Coll Radiol) 2008;20(5):358–64. [CrossRef]
[Pubmed]
10.
Yahya S, Bhatt L, King M, et al. Survival and toxicity following chemoradiation for carcinoma of the cervix – impact of multiple-phase treatment and shielding. Anticancer Res 2015;35(10):5567–74.
[Pubmed]
11.
Zelga P, Tchórzewski M, Zelga M, Sobotkowski J, Dziki A. Radiation-induced rectovaginal fistulas in locally advanced gynaecological malignancies-new patients, old problem? Langenbecks Arch Surg 2017;402(7):1079–88. [CrossRef]
[Pubmed]
12.
Eifel PJ, Jhingran A, Bodurka DC, Levenback C, Thames H. Correlation of smoking history and other patient characteristics with major complications of pelvic radiation therapy for cervical cancer. J Clin Oncol 2002;20(17):3651–7. [CrossRef]
[Pubmed]
13.
Güth U, Ella WA, Olaitan A, Hadwin RJ, Arora R, McCormack M. Total vaginal necrosis: A representative example of underreporting severe late toxic reaction after concomitant chemoradiation for cervical cancer. Int J Gynecol Cancer 2010;20(1):54–60. [CrossRef]
[Pubmed]
14.
Perez CA, Breaux S, Bedwinek JM, et al. Radiation therapy alone in the treatment of carcinoma of the uterine cervix. II. Analysis of complications. Cancer 1984;54(2):235–46. [CrossRef]
[Pubmed]
15.
Tewari KS, Sill MW, Penson RT, et al. Bevacizumab for advanced cervical cancer: Final overall survival and adverse event analysis of a randomised, controlled, open-label, phase 3 trial (Gynecologic Oncology Group 240). Lancet 2017;390(10103):1654–63. [CrossRef]
[Pubmed]
16.
Randall ME, Ibbott GS. Intensity-modulated radiation therapy for gynecologic cancers: Pitfalls, hazards, and cautions to be considered. Semin Radiat Oncol 2006;16(3):138–43. [CrossRef]
[Pubmed]
17.
Gupta S, Zura RD, Hendershot EF, Peterson AC. Pubic symphysis osteomyelitis in the prostate cancer survivor: Clinical presentation, evaluation, and management. Urology 2015;85(3):684–90. [CrossRef]
[Pubmed]
18.
Eswara JR, Raup VT, Heningburg AM, Brandes SB. Pelvic radiation is associated with urinary fistulae repair failure and need for permanent urinary diversion. Urology 2015;85(4):932–6. [CrossRef]
[Pubmed]
19.
Scozzari G, Arezzo A, Morino M. Enterovesical fistulas: Diagnosis and management. Tech Coloproctol 2010;14(4):293–300. [CrossRef]
[Pubmed]
20.
Shackley DC, Brew CJ, Bryden AA, et al. The staged management of complex entero-urinary fistulae. BJU Int 2000;86(6):624–9. [CrossRef]
[Pubmed]
21.
Lane BR, Stein DE, Remzi FH, Strong SA, Fazio VW, Angermeier KW. Management of radiotherapy induced rectourethral fistula. J Urol 2006;175(4):1382–7. [CrossRef]
[Pubmed]
22.
Piekarski JH, Jereczek-Fossa BA, Nejc D, et al. Does fecal diversion offer any chance for spontaneous closure of the radiation-induced rectovaginal fistula? Int J Gynecol Cancer 2008;18(1):66–70. [CrossRef]
[Pubmed]
23.
Vanni AJ, Buckley JC, Zinman LN. Management of surgical and radiation induced rectourethral fistulas with an interposition muscle flap and selective buccal mucosal onlay graft. J Urol 2010;184(6):2400–4. [CrossRef]
[Pubmed]
24.
Maher EJ, Denton A. Survivorship, late effects and cancer of the cervix. Clin Oncol (R Coll Radiol) 2008;20(6):479–87. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
The authors of this manuscript thank to both patients whose clinical cases have been exposed their help to the contribution of medical science development. We would like to thank Dr. Carmen Esteban, Medical Oncologist of Medical Oncology Department in Hospital Virgen de la Salud, for her contribution to the education of new oncologist residents. She has always been open to help and guide clinical and researching projects and she is the light that leads this report and many other researching activities. We would like to thank Dr. Chacón, Head of Medical Oncology Department in Hospital Virgen de la Salud, for his contribution to the education of new oncologist residents and his support in every researching project. As head of department, he has always been approachable and has provided us his experience and science.
Author ContributionsMiguel Borregón Rivilla - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Vicente Serrano Romero de Ávila - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mercedes Acevedo Ribó - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Juan David Cárdenas - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
José Ignacio Chacón López-Muñiz - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Carmen Esteban Esteban - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Miguel Borregón Rivilla et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}