 |
Case Report
Chronic pelvic pain due to post-ablation tubal sterilization syndrome: A case report
1 Department of Obstetrics and Gynaecology, North Devon District Hospital, Barnstaple, Devon EX31 4JB, UK
2 Department of Histopathology, North Devon District Hospital, Barnstaple, Devon EX31 4JB, UK
Address correspondence to:
Osama Eskandar
Department of Obstetrics and Gynaecology, North Devon District Hospital, Barnstaple, Devon EX31 4JB,
UK
Message to Corresponding Author
Article ID: 100093Z08NS2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Shatry N, Alexander M, Eskandar O. Chronic pelvic pain due to post-ablation tubal sterilization syndrome: A case report. J Case Rep Images Obstet Gynecol 2021;7:100093Z08NS2021.ABSTRACT
Heavy menstrual bleeding is a common disorder with an estimated 1 in 20 women in the UK aged 30–49 years consulting their General Practitioner (GP) each year. One of the management options for heavy menstrual bleeding is ablation. This procedure aims to reduce heavy menstrual bleeding by thermally ablating the endometrial lining. In women who have had sterilization, this may result in pelvic pain as a result of tubal distension from occult bleeding into the obstructed tubes. This is a case of a 45-year-old female with history of sterilization by Filshie clips and endometrial ablation, who presented with chronic pelvic pain. This case report highlights the importance of discussing the potential long-term complication of post-ablation tubal sterilization syndrome with the patient. The clinician should have a high index of suspicion to prompt early gynecological referral.
Keywords: Ablation, Pelvic pain, Tubal sterilization
Introduction
Heavy menstrual bleeding is a common disorder with an estimated 1 in 20 women in the UK aged 30–49 years consulting their General Practitioner each year [1].
For some of these women, surgical options are advised including endometrial ablation; a technique that aims to reduce heavy bleeding by thermally ablating the endometrial lining of the uterus. It may not result in amenorrhea but is considered less invasive and uses fewer resources than hysterectomy [1].
Post-ablation tubal sterilization syndrome (PATSS) is one of the rare complications following a global endometrial ablation in women who have had previous tubal sterilization [2]. It presents as cyclic pelvic pain caused by tubal distension from occult bleeding into the obstructed tubes [2],[3].
Case Report
A 45-year-old para 3+0 female with history of sterilization by Filshie clips soon after her last delivery 17 years ago presented with heavy menstrual bleeding resulting in anemia which required iron supplement. Diagnostic hysteroscopy showed a normal uterine cavity with a 7 cm length and endometrial biopsy was benign. Treatment options were discussed with the patient and she opted for endometrial ablation. Four months after the procedure, she presented to accident and emergency (A & E) with continuous and excruciating pelvic pain responding only to morphine. This affected her quality of life and she was unable to perform her daily duties. She was seen in A & E multiple times and was eventually referred to the surgical team due to the fact that she also reported a change in her bowel habit. A colonoscopy was performed and it was normal and she was referred to the gynecology team. An ultrasound revealed avascular internal echoes within the myometrial cavity and another anechoic cystic area adjacent to the endometrial cavity as well as a posterior wall intramural fibroid measuring 22 mm (Figure 1).
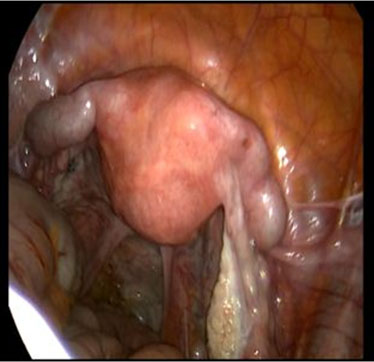
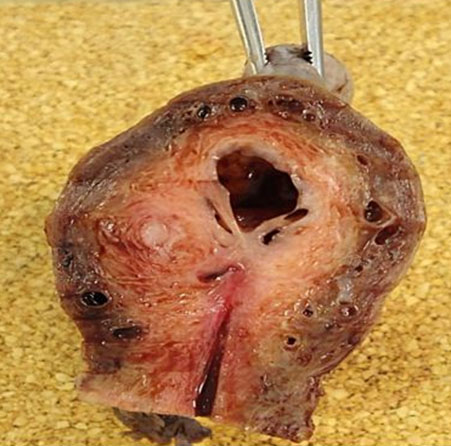
After a discussion with the gynecologist, the patient opted for a total laparoscopic hysterectomy and bilateral salpingo-oophorectomy. Intra-operative findings included bilaterally dilated tubes with Filshie clips but apart from a small posterior wall uterine fibroid, the uterus appeared grossly normal in external appearance (Figure 2). Histopathology examination revealed that there was a cystic area at the fundus lined by a thin layer of endometrial epithelium and scarring in the isthmic region of the endometrial cavity with cornual hematometra consistent with PATSS (Figure 3). She did well post-operatively with resolution of her pain.

Discussion
There are a number of complications that may follow an endometrial ablation, some of which include central hematometra, corneal hematometra, and post-ablation tubal sterilization syndrome [4]. Pathologically confirmed post-ablation tubal sterilization syndrome has an incidence of 6%, however this may be higher if assessed clinically [5].
Post-ablation tubal sterilization syndrome is a diagnosis suspected from clinical findings and imaging. As shown in this patient, it may go undiagnosed and be a source of chronic debilitating pain. Sonographic features include dilated proximal fallopian tubes with anechoic or hypoechoic fluid collections, which may contain low-level internal echoes [4].
Endometrial ablation usually causes scarring and stenosis in the upper endocervical canal or isthmic region. This is associated with development of central and corneal hematometra, usually due to incomplete ablation of the endometrium of these areas. Eventually this can lead to hematosalpnix with corresponding pain.
Treatment options include hysterectomy with salpingectomy but some have attempted bilateral excision of the tubal stumps alone [3],[4].
Conclusion
Post-ablation tubal sterilization syndrome is one of the long-term complications of endometrial ablation and should be discussed with the patients especially those with history of sterilization or when a clinician opts to do the two procedures simultaneously. One should have a high index of suspicion to prompt early gynecological referral in women presenting with chronic pelvic pain following endometrial ablation and tubal sterilization.
REFERENCES
1.
Fluid-filled thermal balloon and microwave endometrial ablation techniques for heavy menstrual bleeding. Technology appraisal guidance. Published: 28 April 2004, NICE 2019.

2.
Tam T, Elgar C, Jirschele K, Lombard E. Post-ablation tubal sterilization syndrome following NovaSure endometrial ablation: Two case reports. Gynecol Surg 2012;9:449–52. [CrossRef]
3.
Akinlaja O, Sherrow S. Postablation tubal sterilization syndrome—A case report. Austin J Obstet Gynecol 2014;1(1):2.
4.
Morrison JJ, Bronitsky BG, Sandberg SA, Craig B. Sonographic findings in postablation tubal sterilization syndrome. J Ultrasound Med 2013;32(8):1515–7. [CrossRef]
[Pubmed]
5.
Mall A, Shirk G, Van Voorhis BJ. Previous tubal ligation is a risk factor for hysterectomy after rollerball endometrial ablation. Obstet Gynecol 2002;100(4):659–4. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Naima Shatry - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mary Alexander - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Osama Eskandar - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Naima Shatry et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}