 |
Clinical Video
Laparoscopic management of external iliac vein injury
1 Associate Professor, Gynecologic Oncology Department, Samsun Ondokuz Mayıs University, Samsun, Turkey
2 Medical Doctor, Gynecologic Oncology Department, Sanlıurfa Research and Training Hospital, Sanlıurfa, Turkey
Address correspondence to:
Gozde Sahin
Sanlıurfa Research and Training Hospital, Sanlıurfa,
Turkey
Message to Corresponding Author
Article ID: 100101Z08IY2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Yalcin I, Sahin G. Laparoscopic management of external iliac vein injury. J Case Rep Images Obstet Gynecol 2021;7:100101Z08IY2021.ABSTRACT
No Abstract
Keywords: Complete hydatidiform mole, Human serum chorionic gonadotropin, Intrauterine pregnancy
Case Report
A 57-year-old white woman was referred to our division for incomplete surgically staged endometrial cancer. She was taken to the operating room for laparoscopic surgical staging. Incidental right external vein injury occurred during pelvic lymphadenectomy.
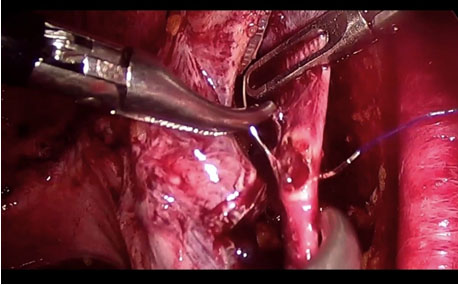
Video 1 shows an incidental thermal full thickness injury of right external iliac vein and repairing it laparoscopically during a pelvic lymphadenectomy procedure.
A 3 mm laceration to the right external iliac vein occurred while right pelvic lymphadenectomy (Figure 1). After immediate clamping of the injury site with graspers, the laceration on the right external iliac vein was primarily repaired by use of a running intracorporeal 4-0 polypropylene suture (Figure 2). The insufflation pressure was increased to 20 mmHg for the duration of primary repair for 60 seconds to limit the hemorrhage. The patient was not obese and her body mass index (BMI) was 24.
Access video on other devices

Discussion
Minimal invasive techniques are more popular in cancer surgery. Laparoscopy has lots of advantages in cancer patients as early mobilization and short hospitalisation. It is one of the most commonly performed procedures. Injury to a major retroperitoneal vessel occurs in 0.3–1.0% of procedures, most commonly during laparoscopic entry while placing the Veress needle or primary trocar. Veins have much thinner walls compared with arteries so veins might be at greatest risk of laceration during surgical dissection [1],[2]. Risk of injury is more in obese patients and after previous surgeries.
Vessel injuries can occur during trocar placement or insertion of Veress needle mostly [2] but dissections, uncontrol tractions and electricity, as in our case, can cause damage in vessels. The most common vessels injured are branches of distal aorta, iliac vessels, and inferior vena cava. The second most common cause of death during laparoscopy is major vascular injury with a mortality rate of 6.37% [3],[4].
Management of vascular injuries needs immediate recognition of injury and rapid hemostasis and they can be done by laparoscopy with experienced surgeons or laparotomy.
Lymphadenectomy is a part of operation in gynecological cancer staging surgeries. In our case we had injury on right external iliac vein during lymphadenectomy for endometrial cancer. Energy sources must be used carefully during lymphadenectomy, in old patients vessel walls are more fragile and vein walls are thinner than arteries. Coagulation can be used in injuries smaller than 2 mm, but injuries larger than 2 mm must be repaired. In our case we had 3 mm injury and we repaired it laparoscopically [5]. If there is no availability of experienced surgeon when a major vessel injury occurs during laparoscopy, vascular surgeon is recommended.
Conclusion
Repair of external iliac vein injury, during laparoscopy can be performed successfully and safely by experienced laparoscopic surgeons.
REFERENCES
1.
Makai G, Isaacson K. Complications of gynecologic laparoscopy. Clin Obstet Gynecol 2009;52(3):401–11. [CrossRef]
[Pubmed]

2.
Sandadi S, Johannigman JA, Wong VL, Blebea J, Altose MD, Hurd WW. Recognition and management of major vessel injury during laparoscopy. J Minim Invasive Gynecol 2010;17(6):692–702. [CrossRef]
[Pubmed]
3.
Barros MB, Lozano FS, Queral L. Vascular injuries during gynecological laparoscopy—The vascular surgeon’s advice. Sao Paulo Med J 2005;123(1):38–41. [CrossRef]
[Pubmed]
4.
Dixon M, Carrillo EH. Iliac vascular injuries during elective laparoscopic surgery. Surg Endosc 1999;13(12):1230–3. [CrossRef]
[Pubmed]
5.
Chiantera V, Erdemoglu E, Vercellino G, Straube M, Schneider A. Laparoscopic management of external iliac artery injury using yasargil clamps and intracorporeal suture. J Minim Invasive Gynecol 2011;18(4):516–9. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Ibrahim Yalcin - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Gozde Sahin - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Ibrahim Yalcin et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}