 |
Clinical Image
Vaginal light bulb removal with ligature loop device
1 MD, Resident, University of Florida of Obstetrics and Gynecology, Gainesville, Florida 32605, United States
2 MD, Assistant Clinical Professor, University of Florida of Obstetrics and Gynecology, Gainesville, Florida 32605, United States
3 MD, Associate Clinical Professor, Division of Female Pelvic Medicine and Pelvic Reconstruction, University of Florida of Obstetrics and Gynecology, Gainesville, Florida 32605, United States
Address correspondence to:
Vasanti Jhaveri
1600 Southwest Archer Road, Gainesville, Florida 32605,
United States
Message to Corresponding Author
Article ID: 100112Z08VJ2022
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Jhaveri V, Larzelere M, Heft J. Vaginal light bulb removal with ligature loop device. J Case Rep Images Obstet Gynecol 2022;8:100112Z08VJ2022.ABSTRACT
No Abstract
Keywords: Ligature loop, Light bulb, Vaginal foreign body
Case Report
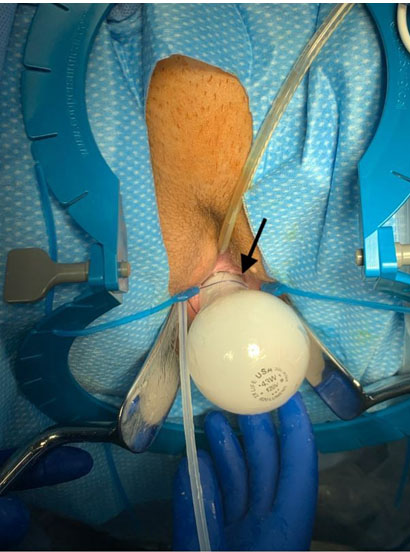
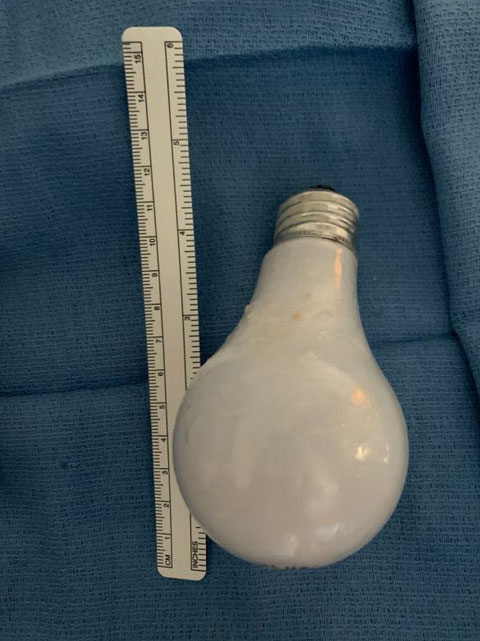
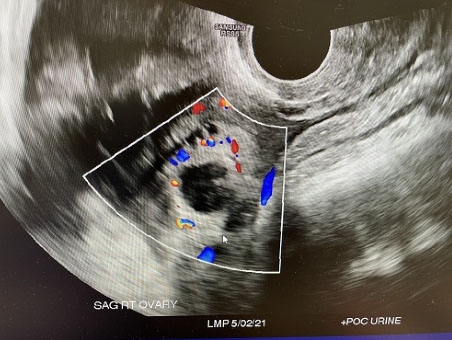
A 33-year-old woman, para 4004, presented as a transfer from an outside hospital for sexual assault. Per report, a light bulb had been inserted vaginally into the patient. While at the outside hospital, imaging showed one intact light bulb in the vagina (Figure 1 and Figure 2). After her computed tomography (CT) scan, the patient reported that she sat up and felt a sharp pain as if the bulb had broken. She was taken to the operating room for cystoscopy, exam under anesthesia, removal of foreign body from the vagina, and any other indicated procedures. Cystoscopy was performed first and was overall within normal limits. On pelvic exam, the dome of the light bulb was visualized and appeared intact but the metal base of the bulb was positioned more proximally and was unable to be seen. An ENDOLOOP ligature loop device was carefully placed circumferentially around the bulb and then tightened to provide gentle traction and aid in removal of the bulb (Figure 3). Although partially cracked, the bulb had remained intact (Figure 4). Copious irrigation was performed and close inspection confirmed no damage to the vaginal epithelium. Rectal exam was normal. Repeat cystoscopy showed bilateral ureteral efflux.


Discussion
Vaginal foreign bodies may present in female patients of all ages from prepuberty to adults [1]. In the adult patient population, vaginal foreign bodes have been cited in the literature as retained medical devices in the elderly, illicit substance in drug traffickers, and even retained gauze and surgical packing in a postpartum patient [2],[3],[4].
Adult women often self-report these injuries and present with abdominal pain, vaginal bleeding, or discharge. A careful history with details surrounding the initial event, timing of event, symptoms of the abdomen, and pelvic area are imperative. Along with physical exam, imaging may also be helpful including abdominal radiography, CT scan, and magnetic resonance imaging (MRI) of the abdomen and pelvis. In this case, an outside CT scan was used to guide next steps in evaluating this patient. The CT scan showed one light bulb in the vagina, which appeared intact. However, the patient self-reported that she felt that the light bulb may have broken in her vagina. Given the patient’s history which could entail a more extensive injury, the decision was made to proceed with general anesthesia prior to physical examination. In the operating room, extreme care was taken during the physical exam as shattered glass may have been present. Ultimately an ENDOLOOP ligature device was used to remove the light bulb. Retained foreign bodies are noted to have severe complications including infection, pelvic inflammation, ulceration, frequent urinary tract infections, rectal bleeding, and fistula formation [5].
Given the extreme risks that vaginal foreign bodies pose, they are considered clinically significant. Prompt evaluation with careful physical evaluation is vital to remove and reduce the risk of complications.
Conclusion
To our knowledge, this clinical image is the first in the medical literature of a light bulb in the vagina and describes its clinical and surgical management.
REFERENCES
1.
Stricker T, Navratil F, Sennhauser FH. Vaginal foreign bodies. J Paediatr Child Health 2004;40(4):205–7. [CrossRef]
[Pubmed]

2.
Abesamis MG, Taki N, Kaplan R. Uterine body stuffing confirmed by computed tomography. Clin Pract Cases Emerg Med 2017;1(4):365–9. [CrossRef]
[Pubmed]
3.
Wankhade VK, Chikhalkar BG. Body packing and intra-vaginal body pushing of cocaine: A case report. Leg Med (Tokyo) 2018;31:10–3. [CrossRef]
[Pubmed]
4.
Wu CC, Hsieh ML, Wang TM. Retained vaginal gauze with unusual complication: A case report. Changgeng Yi Xue Za Zhi 1997;20(1):62–5.
[Pubmed]
5.
Anderson J, Paterek E. Vaginal Foreign Body Evaluation and Treatment. 2021 May 19. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Vasanti Jhaveri - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Michelle Larzelere - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jessica Heft - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2022 Vasanti Jhaveri et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}