 |
Case Report
Quadruplet pregnancy with widespread Tenney-Parker changes: A case report
1 Department of Obstetrics and Gynecology, Texas Tech University Health Sciences Center, Permian Basin, Odessa, Texas, USA
2 Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, School of Medicine, Texas Tech University Health Sciences Center, Permian Basin, Odessa, Texas, USA
3 School of Medicine Research Laboratory, Department of Obstetrics and Gynecology, Texas Tech University Health Sciences Center, Permian Basin, Odessa, Texas, USA
Address correspondence to:
Gary Ventolini
MD, FACOG, FAAFP, Professor of Obstetrics and Gynecology, University Distinguished Professor, Texas Tech University Health Sciences Center at the Permian Basin, 800 W. 4th Street, Odessa, TX 79763,
USA
Message to Corresponding Author
Article ID: 100120Z08ST2022
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Thomas S, Enakpene C, Sanchez A, Ventolini G. Quadruplet pregnancy with widespread Tenney-Parker changes: A case report. J Case Rep Images Obstet Gynecol 2022;8(1):24–28.ABSTRACT
Introduction: The incidence of multiple pregnancies has increased tremendously over the last 3–4 decades due to the advent of assisted reproductive technology treatment. Generally, multifetal pregnancy is associated with increase in maternal and perinatal morbidity and mortality, which are directly proportional with increasing numbers of fetuses in higher order multiple pregnancies.
Case Report: We present a case of a 26-year-old G1P0104 female with a 3-year history of anovulatory infertility. After the third cycle of ovarian stimulation with clomiphene citrate, she became pregnant with quadruplets. She had no significant past medical or surgical history. The pregnancy was a tetrachorionic-tetraamniotic quadruplet and it was relatively uncomplicated during the first and second trimesters. However, the patient had prolonged antepartum admission from 25w6d due to symptomatic preterm uterine contractions. At 31w3d, the patient underwent primary cesarean section due to non-reassuring fetal heart tracing and biophysical profile of quadruplet A. Four viable neonates were delivered, three females and one male. All four quadruplets were admitted to the Neonatal Intensive Care Unit (NICU) with varying degrees of neonatal complications due to prematurity, but they were discharged home between 8 and 9 weeks of life. The placental pathology showed Tenney-Parker changes, but it did not adversely affect the outcome of these infants.
Conclusion: Higher-order multifetal pregnancies can pose serious management challenges because of increased preterm delivery. Hence, management should be in a tertiary medical center with a multi-disciplinary team that includes an Obstetrician, Perinatologist, and Neonatologist.
Keywords: Antenatal surveillance, Cesarean section, Placental pathology and syncytial knots, Preterm contractions, Quadruplet pregnancy
Introduction
Triplet and higher-order multifetal gestations are a rare occurrence, accounting for only 87.7 per 100,000 live births in the United States in 2019 even with the contributing factor of assisted reproductive technologies [1]. Multifetal gestation comes with increased risk of significant maternal, perinatal, and neonatal complications. Majority of multiple pregnancies are delivered prematurely, and nearly all higher-order multifetal gestations result in premature delivery. Premature births come with a host of complications either due to underlying perinatal conditions or simply arise from the underdeveloped fetus’ exposure to the outside environment.
Antenatal care and surveillance of these pregnancies can often be quite complex and is aimed at minimizing these significant complications. Pathologies that affect premature infants often severely impair their development or even prove to be fatal if not identified and treated promptly. Among them are respiratory distress syndrome (RDS), necrotizing enterocolitis (NEC), neonatal hypoglycemia and hyperbilirubinemia, intraventricular hemorrhage, and bronchopulmonary dysplasia. Necrotizing enterocolitis is a relatively common condition that affects about 7% of premature neonates, and it poses a devastating threat to their well-being and development [1]. Mortality from NEC ranges from 20% to 40% in preterm infants and, like most complications of prematurity, it has an inverse relationship with gestational age at delivery and birth weight [2]. Although the etiology of NEC is not fully understood, the most important risk factor is prematurity. Other risk factors include formula feeding and congenital malformations, particularly congenital heart disease. However, it is not uncommon for NEC to develop even with no predisposing risk factors. Respiratory distress syndrome occurs in the premature infant due to surfactant deficiency in the underdeveloped lungs. One-third of infants born at 28 to 34 weeks gestation are affected by RDS [3]. This case report of a quadruplet pregnancy showed widespread placental Tenney-Parker changes, and infants with neonatal complications secondary to prematurity.
Case Report
The patient was a 26-year-old G1P0104 female with a 3-year history of infertility. Her work-up by a reproductive infertility endocrinologist (REI) showed normal semen analysis, normal hysterosalpingography with bilateral tubal patency, but she had ovulatory dysfunction (anovulatory cycles). The couple underwent ovarian stimulation for ovulation induction with clomiphene citrate that was started at 50 mg from day 5 to day 9 of the cycle, increased to 100 mg for the second cycle, and 150 mg on the third cycle. At the completion of the third cycle of clomiphene citrate, the patient became pregnant, which resulted in quadruplets.
She was followed up by a general obstetrician and maternal fetal medicine (MFM) specialist. She was admitted to the prenatal unit at 25 weeks and 6 days for bed rest and prolong monitoring due to frequent symptomatic premature uterine contractions. At the gestational age of 31 weeks and 3 days, the patient underwent emergent primary cesarean delivery due to a non-reassuring biophysical profile and fetal heart tracing of one of the quadruplet fetuses. She was delivered of four live neonates, three females and one male with Apgar scores ranging between 5 to 7 in 1 minute and 7 to 9 in 5 minutes. Quadruplet A weighted 1505 g, quadruplet B 1566 g, quadruplet C 1588 g, and quadruplet D 1428 g.
All of the four quadruplets were admitted to the Neonatal Intensive Care Unit (NICU), and they developed various degrees of RDS. In addition, quadruplet A was diagnosed and treated with mild NEC, quadruplet B developed grade 1 intraventricular hemorrhage, quadruplet C had severe RDS, and quadruplet D had several episodes of apnea, bradycardia, anemia that required blood transfusions, and unable to maintain body temperature for several weeks. They were all discharged between 8 and 9 weeks, one at a time and in excellent condition. The patient returned to the OBGYN clinic for a 2-week follow-up for a wound check and at six weeks for a postpartum visit. Her overall postpartum period was uneventful except that she expressed being tired of her daily visits to the NICU.
Discussion
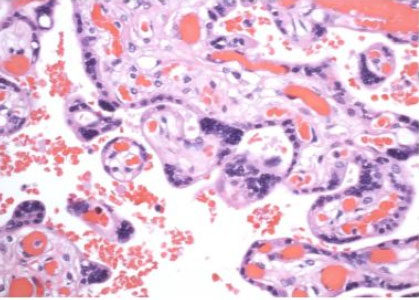
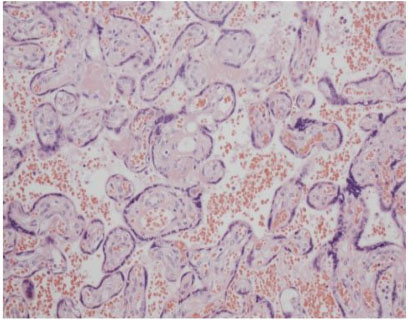
This is a case of a 26-year-old now G1P0104 woman with three years of anovulatory infertility. She became pregnant through controlled ovarian stimulation at the completion of her third cycle of clomiphene citrate and the pregnancy resulted in quadruplets. She had a prolonged history of symptomatic uterine contractions resulting in a hospitalization from 26 to 31 weeks. However, she underwent urgent cesarean delivery due to non-reassuring biophysical profile of one of the quadruplets. She was delivered of four live neonates; three females and one male. The placenta retrieved (Figure 1) showed widespread Tenney-Parker changes upon histologic examination. Figure 2 depicts the widespread Tenney-Parker changes in the retrieved placenta, but Figure 3 shows a normal placenta histology for comparison. Multifetal pregnancies are often associated with increased pregnancy complications, adverse perinatal outcomes, and increased maternal morbidity. Women with multifetal pregnancy are 6 times more likely to have a premature delivery and 13 times more likely to deliver before 32 weeks [4]. There is also an increased risk of short- and long-term neonatal and infant morbidity associated with multifetal gestations.
Most of these complications are as a result of prematurity and chorionicity. Though there is an increase in neonatal and infant morbidity with higher order gestations, there have been several reports of quadruplet pregnancies with resultant healthy neonates. Hafizi et al. described a quadruplet pregnancy case delivered at 32w4d with four healthy neonates [5]. In a study by Basit et al., which looked at the mode of conception for triplet or higher order multiple pregnancies, only 15.8% pregnancies resulted from ovulation induction using clomiphene citrate [6]. There have also been multiple reports of prophylactic cerclages placed to prolong gestation in higher order multiple pregnancy. A case report by Carrara et al. described a quadruplet pregnancy with a prophylactic cerclage placed at 23 weeks, and delivered at 34 weeks [7]. In this patient, despite symptomatic preterm contractions with cerclages in place, the pregnancy was further prolonged for approximately five weeks from the onset of uterine contractions.
The placenta starts to develop at the time of implantation of the blastocyst into the endometrium. Trophoblasts form the outer lining of the blastocysts and they are one of the primary cell types. The trophoblasts can develop into undifferentiated cytotrophoblasts and fully differentiated syncytiotrophoblasts [8]. Syncytiotrophoblast (STB) are multinucleated specialized epithelial cells that cover the entire surface of the placental villi and form the maternal fetal interface that is responsible for exchange between the fetal and maternal circulation. The nuclei within the syncytiotrophoblasts can aggregate forming true and false syncytial knots and syncytial sprouts [9]. Nuclei within true knots are highly condensed and are considered to be aged and have low levels of transcriptional activity. Increased or excessive number of true knots is called Tenney-Parker changes [9]. They can be prominent findings in post-term placentas and as well as complicated pregnancies [9].
In our case, widespread Tenney-Parker changes were noted in the placenta pathology. Tenney-Parker changes are thought to be evidence of oxidative damage [9]. Knots are rarely seen prior to 20 weeks of gestation [9]. The knots are thought to be indicative of placental maturity; however, increased knotting can be associated with uteroplacental malperfusion [10]. These changes have been linked to placental changes of women with pre-eclampsia, but they have not been established to be a pathological finding associated with higher order multiple gestations [10]. The full clinical significance of Tenney-Parker changes is yet to be thoroughly defined but the associations with higher order gestations is one that needs further research.

Conclusion
We presented a case of a 26-year-old G1P0104 who had a complicated antepartum course after ovulation induction using clomiphene citrate that resulted in quadruplet pregnancy. Although she had a complicated pregnancy course requiring prolonged hospitalization and urgent cesarean section at 31 weeks of gestation, she was delivered of four live infants who were admitted in the NICU. Despite some neonatal complications as expected, the infants were all discharged home between 8 and 9 weeks after delivery in excellent conditions. Tenney-Parker changes were a unique finding that was observed within the placenta.
REFERENCES
1.
Martin JA, Hamilton BE, Osterman MJ, Driscoll AK. Births: Final data for 2019. Natl Vital Stat Rep 2021;70(2):1–51.
[Pubmed]

2.
Rich BS, Dolgin SE. Necrotizing enterocolitis. Pediatr Rev 2017;38(12):552–9. [CrossRef]
[Pubmed]
3.
Wertheimer F, Arcinue R, Niklas V. Necrotizing enterocolitis: Enhancing awareness for the general practitioner. Pediatr Rev 2019;40(10):517–27. [CrossRef]
[Pubmed]
4.
Hermansen CL, Lorah KN. Respiratory distress in the newborn. Am Fam Physician 2007;76(7):987–94.
[Pubmed]
5.
Hafizi L, Rezaii Asgarieh E, Taheri N, Ghomian N. Successful management of spontaneous quadruplet pregnancy: A case report. J Family Reprod Health 2018;12(3):173–6.
[Pubmed]
6.
Basit I, Johnson SN, Mocanu E, Geary M, Daly S, Wingfield M. Mode of conception of triplets and high order multiple pregnancies. Ir Med J 2012;105(3):80–3.
[Pubmed]
7.
Carrara S, Cavaliere A, Ermito S, Dinatale A, Pappalardo EM, Militello M. Case report: Successful of a spontaneous quadruplet pregnancy. J Prenat Med 2009;3(1):10–1
[Pubmed]
8.
Wang Y, Zhao S. Vascular Biology of the Placenta. San Rafael (CA): Morgan & Claypool Life Sciences; 2010. Chapter 4, Cell Types of the Placenta. [Available at: https://www.ncbi.nlm.nih.gov/books/NBK53245/]
9.
Fogarty NME, Ferguson-Smith AC, Burton GJ. Syncytial knots (Tenney-Parker changes) in the human placenta: Evidence of loss of transcriptional activity and oxidative damage. Am J Pathol 2013;183(1):144–52. [CrossRef]
[Pubmed]
10.
Loukeris K, Sela R, Baergen RN. Syncytial knots as a reflection of placental maturity: Reference values for 20 to 40 weeks’ gestational age. Pediatr Dev Pathol 2010;13(4):305–9. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Serin Thomas - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Christopher Enakpene - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Asley Sanchez - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Gary Ventolini - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2022 Serin Thomas et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}