 |
Case Report
Medical management of hepatic ectopic pregnancy with systemic methotrexate, MRI and serial HCG monitoring
1 MD, MSPH, Clinical Fellow in the Division of Complex Family Planning, Department of Obstetrics & Gynecology, OHSU, Portland, OR, USA
2 MD, MPH, Resident Physician, Department of Obstetrics & Gynecology, OHSU, Portland, OR, USA
3 BS, School of Medicine, OHSU, Portland, OR, USA
4 MD, MCR, Assistant Professor & Complex Family Planning Clinical Lead, Department of Obstetrics & Gynecology, OHSU, Portland, OR, USA
Address correspondence to:
Abigail Liberty
MD, MSPH, Kohler Pavilion, 808 SW Campus Dr., Portland, OR 97239,
USA
Message to Corresponding Author
Article ID: 100134Z08AL2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Liberty A, Nacev E, Doshi U, Colwill A. Medical management of hepatic ectopic pregnancy with systemic methotrexate, MRI and serial HCG monitoring. J Case Rep Images Obstet Gynecol 2023;9(1):1–6.ABSTRACT
Introduction: Hepatic ectopic pregnancies remain a diagnostic challenge which contributes to high morbidity. Little is known about the efficacy of medical management of hepatic ectopic pregnancies. As early pregnancy diagnosis continues to improve, more abdominal ectopic pregnancies will be identified before a complication occurs and patients may be candidates for less invasive management approaches.
Case Report: A reproductive age G2P0010 presented with pleuritic RUQ pain and was ultimately diagnosed with a hepatic ectopic pregnancy. Given the location of the pregnancy and the difficulty accessing it from both an interventional radiology and surgical perspective, inpatient medical management with methotrexate was pursued. A multidisciplinary team including gynecology, interventional radiology, hepatobiliary surgery, and trauma surgery all participated in perioperative planning in case of an acute deterioration. The patient remained hemodynamically stable and exhibited an appropriate response to methotrexate therapy using the multi-dose regimen. Persistent radiographic changes were still evident in the liver six months later despite resolution of the human chorionic gonadotropic (HCG) values.
Conclusion: This case represents a conservative approach to a complex diagnosis and should inform future clinicians expeditious administration of methotrexate therapy and careful consideration of interval imaging for treatment response.
Keywords: Abnormal pregnancy, Ectopic pregnancy, Methotrexate therapy
Introduction
Ectopic pregnancies are uncommon but potentially devastating complication of pregnancy. Of these, 1.3% occur in the abdomen which poses a diagnostic challenge as the standard ultrasonographic assessments of pregnancy may not localize the pregnancy [1]. Patients may desire to avoid radiation exposure associated with computed tomography (CT) imaging in early desired pregnancies. These diagnostic challenges further increase the morbidity of abdominal ectopic pregnancies.
Due to this morbidity, the mainstay of treatment of abdominal ectopic pregnancy, including hepatic pregnancies, is surgical. Our understanding of the role of surgery in management is likely confounded by patients presenting in extremis prior to diagnosis. While there are case reports of combination medical and minimally invasive surgical management of abdominal ectopic pregnancies [2], there is little known about utilizing standard methotrexate regimens. As early pregnancy diagnosis continues to improve through access to first trimester ultrasounds and highly sensitive HCG tests, more abdominal ectopic pregnancies will be identified before a complication occurs. Understanding the appropriate minimally invasive surgical or medical approach to these pregnancies can greatly reduce morbidity to patients and families affected.
Case Report
A reproductive age G2P0010 presented to hospital A on Day 1 with right trapezius pain which extended to the right upper quadrant and flank. The pain had both positional and pleuritic exacerbations. The patient was hemodynamically stable but pain causing tearfulness and emesis. Her medical history was notable for tobacco use, history of anxiety and depression, and mild asthma. She had chlamydia several months prior with a negative test of cure at an appropriate interval. Her prior pregnancy ended in miscarriage at seven weeks, managed expectantly with complete resolution by a negative human chorionic gonadotropin (HCG) level. She had experienced one prior gynecologic procedure, a stringless IUD removal, but otherwise had no history of intra-abdominal procedures. She reported not using contraception prior to conception.
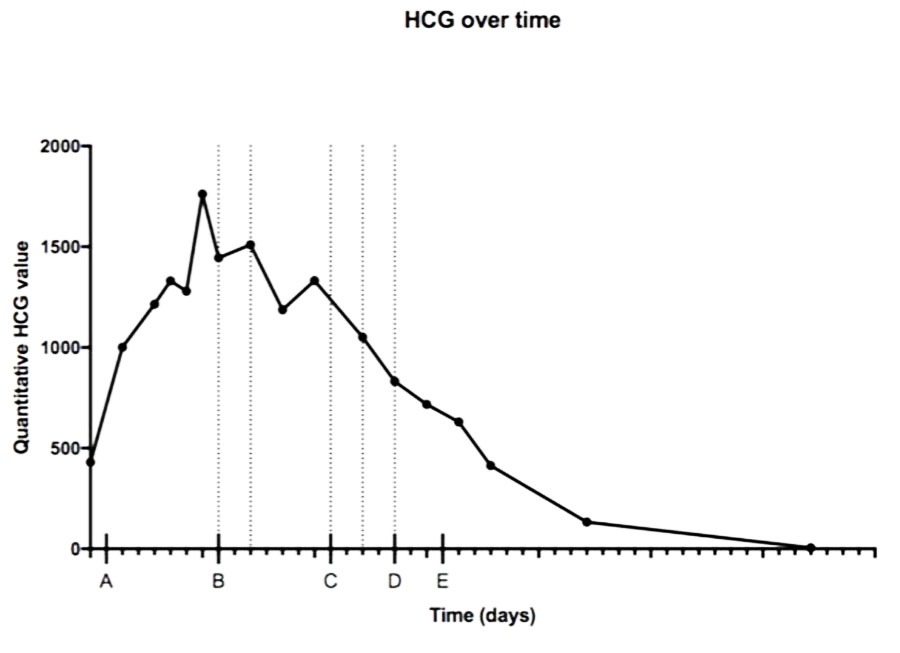
At the time of initial presentation, the leading differential diagnosis was cholecystitis, pyelonephritis, or nephrolithiasis. Upon initial evaluation, a positive pregnancy test was noted, which elevated the suspicion for ectopic pregnancy. The patient’s last menstrual period was six weeks prior to presentation. The patient reported a desire to continue the pregnancy. She endorsed vaginal bleeding similar to menses the week prior to presentation but denied any ongoing vaginal bleeding. Ultrasound imaging revealed no cholecystitis or right renal anomalies, but there was trace free fluid in the right upper quadrant. Pelvic imaging revealed an endometrial thickness of 6.3 mm and moderate echogenic free fluid throughout the pelvis, with absence of intrauterine pregnancy. Urinalysis and blood work did not suggest an infectious process. A quantitative HCG was 430 (Figure 1).
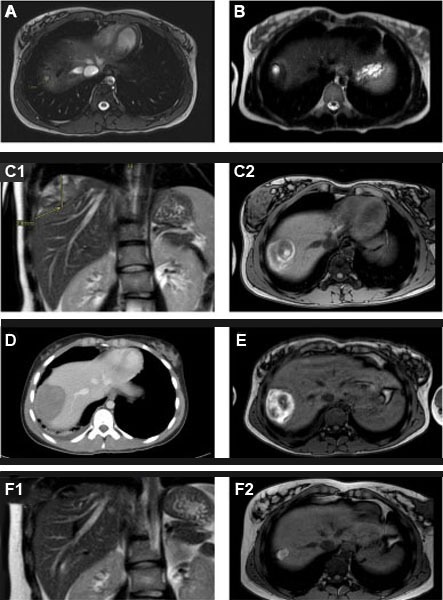
On Day 2 during the same emergency department evaluation, the patient underwent an uncomplicated laparoscopy for suspected ectopic pregnancy which was notable for normal appearing fallopian tubes and a large clot spanning the majority of the cephalad liver edge. Filmy adhesions were noted between bowel, gallbladder, and inferior liver edge. No active bleeding was observed. Intraoperative consultation to general surgery recommended additional imaging. Computed tomography scan of the abdomen suggested liver hemangioma. Subsequent abdominal MRI at that time did not comment on a liver lesion at that time (Figure 2A with identification of an area that was later determined to be an early pregnancy). The patient was discharged on Day 2.
Human chorionic gonadotropin levels collected on Day 3 and Day 5 continued to rise. The patient re-presented to hospital A with worsening pleuritic shoulder pain on Day 6 after their initial presentation. Abdominopelvic ultrasound revealed moderate complex free fluid and no intrauterine pregnancy. Computed tomography of abdomen showed the interval development of a 5.2×1.9 cm lenticular-shaped hematoma inferior to the right hemidiaphragm without obvious source (images not available). In the setting of hemodynamic stability, the patient discharged to home.
In the setting of possible plateau or rising HCG, the patient underwent an office endometrial biopsy on Day 7 which showed fragments of secretory endometrium, no chorionic villi or products of conception. At this time point, abdominal ectopic pregnancy was considered by the patient’s primary OBGYN and the diagnosis was discussed with the patient at an office visit. Human chorionic gonadotropin was 1279. The patient continued to desire outpatient management.
On Day 8, HCG rose to 1762. The patient presented to a tertiary care center at Hospital B as recommended. Repeat pelvic US again showed no evidence of an intrauterine pregnancy. Magnetic resonance imaging demonstrated a subcapsular hematoma overlying liver dome in the same location as the previous CT scan, now containing a 1.8 cm fluid filled structure (Figure 2B). No other location suspicious for ectopic pregnancy in the abdomen or pelvic were identified.
The initial differential diagnosis of right upper quadrant pain was broad and included nephrolithiasis, pyelonephritis, and cholecystitis. Imaging supporting liver abnormalities further broadened the differential to include suprahepatic clot as an incidental finding in the setting of hemoperitoneum or ectopic pregnancy upon result of a positive HCG. Interval imaging did not initially narrow the differential diagnosis to abdominal pregnancy as the imaging was nonspecific suggesting a possible hemangioma, a common benign lesion among people of reproductive age.
Ultimately, failure to locate a tubal ectopic pregnancy at the time of diagnostic laparoscopy, intraoperative evidence of RUQ pathology, short-interval serial imaging with an increasingly complex lesion containing cystic structure and a rising HCG strongly suggested a hepatic ectopic pregnancy. Absence of intrauterine pregnancy or concurrent heterotopic pregnancy was also confirmed by lack of chorionic villi on intrauterine aspirate and multiple pelvic ultrasounds showing a stable, thin endometrial stripe.
The patient was admitted on Day 9 to a medical/surgical floor and remained hemodynamically stable during admission. An interdisciplinary approach in management was initiated including General Surgery, Hepatobiliary Surgery, Thoracic Surgery, and Interventional Radiology alongside Gynecology. The surgical teams and interventional radiology affirmed that the only way to access the pregnancy for resection or injection would be through a thoracotomy and transdiaphragmatic approach. Given the patients stability, prior case reports of minimally invasive approaching combining medical and surgical interventions at later gestational ages and the morbidity of this approach, the patient was offered systemic methotrexate. In accordance with the patient’s goals, we pursued a plan of exclusive medical management with a multidose methotrexate regimen. The potential risks of this approach were thoroughly explained, particularly the risk of rupture with life-threatening hemorrhage even if medical management was initiated and successful.
The multidose regimen was chosen given the overall increased steady state of methotrexate. This regimen includes serum HCG and methotrexate 1 mg/kg intramuscular dosing every other day. Treatment is stopped when a 15% decline in HCG values is observed or at 5 doses. Rescue leucovorin is administered on alternating days. The patient exhibited a 21% decline following the second dose of MTX and the third dose was held. In hopes of accruing additional data about ongoing response to facilitate possible discharge, an additional HCG was drawn which surprisingly showed a 12% rise. Magnetic resonance imaging completed at that time to evaluate for possible changes in the hepatic lesion (Figure 2C) revealed an increase in the size of the hepatic pregnancy. In light of this HCG rise and increased size, the decision was made to resume intramuscular (IM) methotrexate for a total of 5 doses regardless of intervening HCG changes. Following the 4th treatment dose, the patient had a self-limited episode of chest pain for which a CT scan was ordered (Figure 2D) which showed a stable hepatic lesion. The patient received a total of 5 doses over the course of 12 days and exhibited a sustained drop in HCG at 4 days post completion of methotrexate treatment. Magnetic resonance imaging was completed 3 days following the 5th dose of methotrexate to monitor involution of the pregnancy prior to discharge and showed a stable hepatic lesion (Figure 2E). She was discharged on hospital day 17, which was Day 24 after diagnosis. She received IM Depo Provera for contraception prior to discharge.
The patient was advised to continue weekly then monthly HCG follow-up until HCG was negative. She had a negative urine pregnancy test when presenting for routine follow-up 87 days after discharge. She was advised to use contraception for at least six months due to the methotrexate and continued Depo Provera for contraception given prior positive experience with this method.
Repeat imaging was recommended at six months following treatment to evaluate for possible long-term hepatic changes. A MRI at six months after completion of the last dose of methotrexate showed persistence of a subscapular liver hematoma at the site of the ectopic pregnancy which had continued to involute from 5.5 to 2.5 cm (Figure 2F).
At outpatient follow-up, the patient and their partner reported some psychological stress associated with the diagnosis and hospitalization but reported recovering well, appreciation for their care and outcome and no maladaptive coping. They plan to try to conceive six months after conclusion of treatment and were advised to initiate prenatal vitamins prior to conception and establish early prenatal care for early pregnancy localization per institutional guidelines. The patient conceived after this waiting period and is currently in their third trimester.
Discussion
The diagnosis and treatment of hepatic pregnancies is challenging on several fronts. The mainstay of diagnosis for a tubal ectopic pregnancy is trending serum HCG values with interval ultrasonographic imaging of pelvic organs [3]. In cases of abnormal trends without ultrasonographic evidence of an intrauterine gestation, a uterine evacuation procedure with suction aspiration can provide diagnostic evidence of an ectopic pregnancy without localizing the pregnancy itself. In this case, the uterine sampling by endometrial biopsy without pathologic evidence of an intrauterine pregnancy was a critical point in broadening the diagnosis and pursing MRI. Of note, political restrictions to abortion care through obstructing safe procedures such as dilation and evacuation or provision of methotrexate are known barriers to diagnosis and treatment of life-threatening abdominal and ectopic pregnancies [4],[5]. This case report adds to the literature because of the wealth of radiographic imaging, including multiple modalities which illuminate the dynamic changes following treatment, both acute and long-term. High index of suspicion and MRI were critical for diagnosis and monitoring the hepatic pregnancy. While MRI is optimal for complex hepatic lesions, CT as well as ultrasound can be considered. Although this patient did not have a liver ultrasound, it is unknown whether this would have aided in expediting the diagnosis. In this case, MRI ultimately identified subtle small changes that were not visible by CT, which is consistent with other studies highlighting the superiority of MRI over CT for cystic liver lesions [6]. Computed tomography imaging was employed for acute changes, particularly given the symptomatology of hepatic pregnancies located under the diaphragm which have pleuritic pain concerning for other acute processes such as pulmonary embolism.
Abdominal ectopic pregnancies have been successfully managed with methotrexate in the past but growing literature highlights the nuances of medical management for abdominal ectopic pregnancies. Medical management of tubal ectopic pregnancies involves evaluation for expected declines in HCG following treatment. However, the exposure of the pregnancy to the methotrexate is more variable in abdominal ectopic pregnancies due to altered vasculature. In the case of a hepatic pregnancy, the pregnancy implants into highly vascular area with unknown intrahepatic concentrations of methotrexate. The optimal systemic dosing of methotrexate treatment in abdominal ectopic pregnancies is unknown. A case report of a bowel ectopic pregnancy resolved with 2 doses of intramuscular methotrexate [7].
While systemic exposure is likely superior to local injection for treatment of nontubal ectopic pregnancies, there are increased side effects and, in some instances, local injection might be preferred. A case report described methotrexate directly injected into a hepatic pregnancy on the inferior aspect of the liver at the time of laparoscopy [8]. Advantages of intra-sac methotrexate is a targeted approach with limited systemic exposure to methotrexate. Disadvantages include longer resolution of HCG values compared to systemic methotrexate when used for uterine ectopic pregnancies; during the resolution of HCG, patients remain at risk of ectopic rupture [9]. In the case presented above, intra-sac injection of methotrexate carried increased morbidity due to the anatomic inaccessibility of the pregnancy under the diaphragm which would require thoracotomy and therefore increased the procedural risk without clear advantage over a systemic methotrexate approach.
Intra-arterial methotrexate has been used alone and in combination with uterine artery embolization for adjuvant treatment of cervical ectopic pregnancies and cesarean scar ectopic pregnancies. When used as an adjuvant for uterine artery embolization in the setting of cesarean scar ectopic pregnancies, the HCG values dropped more rapidly, however there was no change in overall success or adverse events [10]. The theoretical advantage of using intra-arterial methotrexate for cesarean scar ectopic pregnancies is that the scar represents a watershed area with altered blood flow that may decrease exposure to systemic methotrexate. The cesarean scar environment differs from the liver, where vascularity is increased. A rapid decline of HCG has also been observed when using intra-arterial methotrexate for cervical ectopic pregnancies as well [11]. Intra-arterial hepatic methotrexate exhibits pharmacokinetics similar to intravenous methotrexate [12] but has not been directly compared to intramuscular methotrexate. One case of hepatic embolization with intra-arterial methotrexate has been described for a partially resected hepatic pregnancy on the inferior aspect of the liver [13] although no cases as primary management have been described. In this case, targeted intra-arterial methotrexate was considered but given the vascular location was not considered preferable to systemic methotrexate.
Conclusion
This case demonstrated successful medical management of a hepatic ectopic pregnancy whose subdiaphragmatic location precluded minimally invasive surgical management. This clinical course is robust with a multitude of imaging and lab values which can aid future clinicians both diagnostically and in management. Systemic methotrexate can be considered for people with early ectopic hepatic pregnancies who are hemodynamically stable in settings that permit close follow-up and access to potential emergent surgery.
REFERENCES
1.
Panelli DM, Phillips CH, Brady PC. Incidence, diagnosis and management of tubal and nontubal ectopic pregnancies: A review. Fertil Res Pract 2015;1:15. [CrossRef]
[Pubmed]

2.
Wang J, Su Z, Lu S, et al. Diagnosis and management of primary hepatic pregnancy: Literature review of 31 cases. Arch Gynecol Obstet 2018;298(2):235–42. [CrossRef]
[Pubmed]
3.
Committee on Practice Bulletins—Gynecology. ACOG Practice Bulletin No. 191: Tubal ectopic pregnancy. Obstet Gynecol 2018;131(2):e65–77. [CrossRef]
[Pubmed]
4.
Foster AM, Dennis A, Smith F. Do religious restrictions influence ectopic pregnancy management? A national qualitative study. Womens Health Issues 2011;21(2):104–9. [CrossRef]
[Pubmed]
5.
Tucker K, Bhardwaj NR, Clark E, Espey E. Delayed diagnosis and management of second trimester abdominal pregnancy. BMJ Case Rep 2017;2017:bcr2017221433. [CrossRef]
[Pubmed]
6.
Azizaddini S, Mani N. Liver Imaging. 2022 Jul 18. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
[Pubmed]
7.
Trail CE, Watson A, Schofield AM. Case of hepatic flexure ectopic pregnancy medically managed with methotrexate. BMJ Case Rep 2018;2018:bcr2017220480. [CrossRef]
[Pubmed]
8.
Nichols C, Koong D, Faulkner K, Thompson G. A hepatic ectopic pregnancy treated with direct methotrexate injection. Aust N Z J Obstet Gynaecol 1995;35(2):221–3. [CrossRef]
[Pubmed]
9.
Koch M, Schwab S, Meyer E, et al. Management of uterine ectopic pregnancy – Local vs. systemic methotrexate. Acta Obstet Gynecol Scand 2018;97(7):824–9. [CrossRef]
[Pubmed]
10.
Gao L, Hou YY, Sun F, et al. A retrospective comparative study evaluating the efficacy of adding intra-arterial methotrexate infusion to uterine artery embolisation followed by curettage for cesarean scar pregnancy. Arch Gynecol Obstet 2018;297(5):1205–11. [CrossRef]
[Pubmed]
11.
Zhang S, Yan H, Ji WT. Uterine artery embolization combined with intra-arterial MTX infusion: Its application in treatment of cervical pregnancy. Arch Gynecol Obstet 2016;293(5):1043–7. [CrossRef]
[Pubmed]
12.
Ignoffo RJ, Oie S, Friedman MA. Pharmacokinetics of methotrexate administered via the hepatic artery. Cancer Chemother Pharmacol 1981;5(4):217–20. [CrossRef]
[Pubmed]
13.
Ma J, Zhou C, Duan Z, Jiang Y. Successful management of primary hepatic pregnancy with selective hepatic artery embolization and intra-arterial methotrexate infusion. Int J Gynaecol Obstet 2013;122(1):78–9. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Abigail Liberty - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Erin Nacev - Acquisition of data, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Uma Doshi - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Alyssa Colwill - Conception of the work, Design of the work, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Abigail Liberty et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}