 |
Case Report
Verrucous carcinoma of the vulva: About a case report
1 Mohamed VI Center for the Treatment of Gyneco-Mammary Cancers, CHU IBN Rochd, Casablanca, Morocco
Address correspondence to:
Imane El Abbassi
Mohamed VI Center for the Treatment of Gyneco-Mammary Cancers, CHU IBN Rochd, Casablanca,
Morocco
Message to Corresponding Author
Article ID: 100145Z08IA2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
El Abbassi I, Tangara S, El Karoini D, Sakim M, Ennachit M, Benhessou M, El Kerroumi M. Verrucous carcinoma of the vulva: About a case report. J Case Rep Images Obstet Gynecol 2023;9(1):49–52.ABSTRACT
Introduction: Verrucous carcinoma of the vulva is a rare lesion, mainly affecting postmenopausal women, this lesion is a distinct and particular entity in the classification of vulvar carcinomas and its progression is uncertain and unpredictable. It is characterized by its extensive exophytic growth without infiltration of the basement membrane.
Case Report: We report a case of verrucous carcinoma of the vulva collected at the Mohamed VI cancer treatment center in Casablanca, we will discuss through a literature review, its therapeutic and evolutionary diagnostic modalities.
Conclusion: Therefore, verrucous carcinoma is a rare entity and its evolution is mainly local, rarely metastatic. It is the indication for exclusive surgical treatment with wide excision without lymphadenectomy in principle. Radiation therapy provides no survival benefit. The prognosis is relatively good but burdened by local recurrences.
Keywords: Verrucous carcinoma, Vulva, Vulvectomy
Introduction
Vulvar cancers represent less than 5% of all female genital cancers, and most often affect postmenopausal women over the age of 60 [1]. Verrucous cancer is a rare entity constituting less than 1% of vulvar cancers, and is characterized by an exophytic appearance and slow growth, rarely metastatic to the lymph nodes [2]. Indeed, it is a well-differentiated form of squamous cell carcinoma linked to viral infection by HPV 6, having the appearance of giant condyloma without invasion of the basement membrane [3]. It has a mainly local evolution, therefore represents the indication for exclusive surgical treatment with local resection in a healthy zone without systematic inguinal lymph node control [4],[5]. We report a case of verrucous carcinoma of the vulva, treated at the Mohamed VI cancer treatment center in Casablanca, reflecting the diagnostic and therapeutic particularities of this pathology.
Case Report
We report the case of a 64-year-old patient, nulligest, menopausal for 10 years, having a history as her sister followed for breast cancer. She consulted for a whitish vulvar lesion associated with vulvar itching evolving for 10 months before her admission, without associated digestive or urinary signs. All evolving in a context of conservation of the general state.
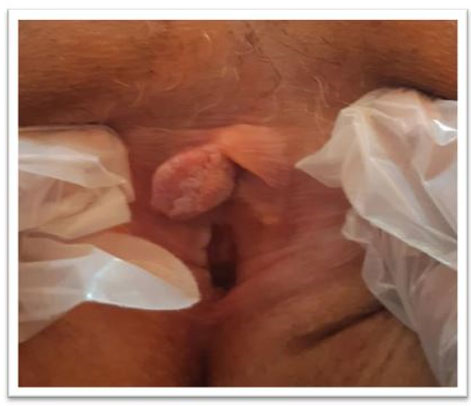
The clinical examination revealed a whitish exophytic lesion of the vulva involving both the right labia minora and the clitoris measuring 3×2.5 cm, the lymph node areas were unharmed (Figure 1).
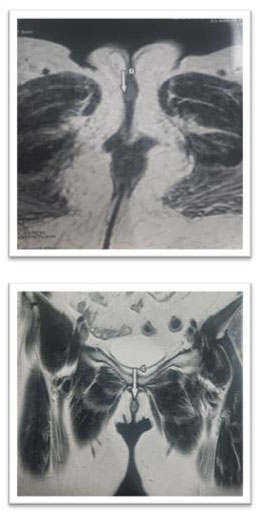
A vulvar biopsy was performed at this level, showing a well-differentiated verrucous carcinoma. The pelvic ultrasound was without abnormality, a pelvic and inguinal magnetic resonance image (MRI) was done highlighting a tissue thickening of the right labia minora with an intermediate signal on T2, in hypersignal intermediate apparent diffusion coefficient (ADC) diffusion, enhanced after injection of the phosphatidyl choline (PDC), measuring 20×17×6 mm. Laterally this process comes into contact with the large homolateral lip with loss of the fibrous border of separation. It respects the ureteral meatus (Figure 2).
A total vulvectomy alone without lymph node dissection was performed. The anatomopathological result confirmed the diagnosis of a verrucous squamous cell carcinoma with healthy resection limits.
Discussion
Verrucous carcinoma is a rare histological variety, only 68 cases have been reported in the literature [6], is characterized by diagnostic and prognostic particularities that should be known to adapt the therapeutic attitude. Indeed, it can occur in the vulva, the ear, nose, throat (ENT) sphere, the penis, the scrotum, or the rectum [7]. Diagnosis, too, can be difficult to make. For this reason, large biopsies should be performed to avoid misdiagnosis and inadequate treatment [8].
Verrucous carcinomas exhibit several histological diagnostic criteria such as a “pushed” tumor-dermis interface with minimal stroma between the acanthotic epithelium, minimal nuclear atypia, hyperkeratotic areas on the surface of the tumor with little keratin formation at inside the tumor and diffuse chronic inflammation of the stroma [9]. It is locally invasive but rarely metastasizing, usually affecting older postmenopausal women, which is consistent with our study. However, its incidence is currently increasing in young women [2],[10]. Indeed, it is a well-differentiated form of squamous cell carcinoma linked to viral infection by HPV 6, found in more than 50% of cases [3],[5], sometimes associated with polyviral involvement, which explains the frequent association of verrucous carcinoma of the vulva with intraepithelial neoplasia and invasive carcinoma of the vulva [5],[11].
Its appearance is characterized by its significant exophytic growth [12]: it is a budding lesion, cauliflower, sometimes associated with a superficial ulceration. This aspect can lead to the incorrect diagnosis of condyloma acuminata or well-differentiated squamous cell carcinoma [7],[13]. Thus, a biopsy that is too superficial and does not include the underlying stroma may underestimate the lesion giving an erroneous diagnosis of condyloma acuminata or overestimate it giving a wrong diagnosis of squamous cell carcinoma of another degree of differentiation [14].
It is therefore essential that the biopsy includes the entire thickness of the lesion: the epithelium and a sufficient quantity of chorion in order to avoid an inadequate diagnosis and treatment [2],[5]. Microscopic examination shows hyperplasia with hyperacanthosis, papillomatosis, and sometimes surface hyperkeratosis. Cellular atypia and mitosis are rare. Epithelial buds are branched but rounded pushing back the underlying chorion. As for the basal membrane, it is always respected [7],[15].
The treatment of verrucous carcinomas of the vulva differs from that proposed for squamous cell carcinomas [16]. However, although it is still a subject of discussion, verrucous carcinoma of the vulva is the indication for exclusive surgical treatment even in the event of recurrence. Indeed, wide resection with a centimetric margin without dissection in principle is the reference treatment because of its attenuated local malignancy [17]. However, the extension of the lesions can nevertheless make the gesture dilapidating. Thus, dissection can only be justified if the definitive examination revealed the presence of a true invasive zone [3],[5], since it exposes to the risk of complications such as lymphocele (40%), scar infection (39%), lymphedema (28%), and suture disunity (17%) [8]. Moreover, radiotherapy does not provide any survival benefit. It can even induce post-radiation anaplastic transformation with the appearance of lesions with high metastatic potential [18].
The prognosis is relatively good in the event of wide excision but is burdened by local recurrences and the risk of appearance of secondary localizations in the event of persistence of the etiological factors (atrophic lichen sclerosis or HPV) [2],[4],[5]. This justifies clinical monitoring every four months during the first year, every six months for two years then every year with a clinical examination of the vulva, perineum, and lymph node areas, possibly supplemented by ultrasound, cytopuncture, and smear screening [4].
Conclusion
Therefore, verrucous carcinoma is a rare entity, well-differentiated histological form of squamous cell carcinoma which is distinguished by its particular diagnostic, therapeutic, and evolutionary modalities. Its treatment is exclusively surgical based on wide excision without lymph node dissection. The prognosis of these lesions is good but burdened by local recurrences.
REFERENCES
1.
Dahbi Z, Elmejjatti F, Naciri F, et al. Vulvar cancer treatment options: Experience in the Oncology Center in Oujda. [Article in French]. Pan Afr Med J 2018;31:182. [CrossRef]
[Pubmed]

2.
Greer BE, Koh WJ. New NCCN guidelines for vulvar cancer. J Natl Compr Canc Netw 2016;14(5 Suppl):656–8. [CrossRef]
[Pubmed]
3.
Khouchani M, Benchakroun N, Tahri A, et al. Breast metastasis from vulvar carcinoma: Case report and review of literature. [Article in French]. Cancer Radiother 2008;12(2):120–5. [CrossRef]
[Pubmed]
4.
Leblanc E, Narducci F, Boukerrou M, Querleu D. Chirurgie du cancer de la vulve. EMC - Techniques Chirurgicales - Gynécologie 2007;23(1):1–16. [CrossRef]
5.
Allouache N, Blanc-Fournier C, Crouet H, et al. Vulvar cancers: Diagnostic and therapeutic management. RRC_GYN_Vulva Update February 2011.
6.
Louis-Sylvestre C, Chopin N, Constancis E, Plantier F, Paniel BJ. Verrucous carcinoma of the vulva: A tailored treatment. [Article in French]. J Gynecol Obstet Biol Reprod (Paris) 2003;32(7):634–7.
[Pubmed]
7.
de Koning MNC, Quint WGV, Pirog EC. Prevalence of mucosal and cutaneous human papillomaviruses in different histologic subtypes of vulvar carcinoma. Mod Pathol 2008;21(3):334–44. [CrossRef]
[Pubmed]
8.
Aynaud O, Asselain B, Bergeron C, et al. Intraepithelial carcinoma and invasive carcinoma of the vulva, vagina and penis in Ile-de-france. Enquete PETRI on 423 cases. [Article in French]. Ann Dermatol Venereol 2000;127(5):479–83.
[Pubmed]
9.
Pape O, Lopès P, Bouquin R, et al. Interest of selective lymphadenectomy in patients with vulvar cancer. [Article in French]. Gynecol Obstet Fertil 2006;34(12):1105–10. [CrossRef]
[Pubmed]
10.
Baldwin P, Latimer J. Vulvar cancer. Current Obstetrics & Gynecology 2005;15(2):113–22.
11.
Zaidi H, Mouhajir N, El Mejjaou S, et al. Cancers primitifs invasifs de la vulve: Expérience de l’Institut National d’Oncologie de Rabat. Pan African Medical Journal 2013;15:146. [CrossRef]
12.
Raspagliesi F, Hanozet F, Ditto A, et al. Clinical and pathological prognostic factors in squamous cell carcinoma of the vulva. Gynecol Oncol 2006;102(2):333–7. [CrossRef]
[Pubmed]
13.
Ghurani GB, Penalver MA. An update on vulvar cancer. Am J Obstet Gynecol 2001;185(2):294–9. [CrossRef]
[Pubmed]
14.
van der Steen S, van de Nieuwenhof HP, Massuger L, Bulten J, de Hullu JA. New FIGO staging system of vulvar cancer indeed provides a better reflection of prognosis. Gynecol Oncol 2010;119(3):520–5. [CrossRef]
[Pubmed]
15.
Boutas I, Sofoudis C, Kalampokas E, Anastasopoulos C, Kalampokas T, Salakos N. Verrucous carcinoma of the vulva: A case report. Case Rep Obstet Gynecol 2013;2013:932712. [CrossRef]
[Pubmed]
16.
Lanneau GS, Argenta PA, Lanneau MS, et al. Vulvar cancer in young women: Demographic features and outcome evaluation. Am J Obstet Gynecol 2009;200(6):645.e1–5. [CrossRef]
[Pubmed]
17.
Johann S, Klaeser B, Krause T, Mueller MD. Comparison of outcome and recurrence-free survival after sentinel lymph node biopsy and lymphadenectomy in vulvar cancer. Gynecol Oncol 2008;110(3):324–8. [CrossRef]
[Pubmed]
18.
Moore DH. Chemotherapy and radiation therapy in the treatment of squamous cell carcinoma of the vulva: Are two therapies better than one? Gynecol Oncol 2009;113(3):379–83. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Imane El Abbassi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
S Tangara - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
D El Karoini - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
M Sakim - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
M Ennachit - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
M Benhessou - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
M El Kerroumi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Imane El Abbassi et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}