 |
Case Report
Pseudotumor cerebri in pregnant obese patient: A case report
1 Edward Via College of Osteopathic Medicine—Auburn Campus, Auburn, AL, USA
2 Kirksville College of Osteopathic Medicine, Kirksville, MO, USA
3 Edward Via College of Osteopathic Medicine—Carolinas Campus, Spartanburg, SC, USA
4 Department of Obstetrics and Gynecology, Piedmont Columbus Midtown, Columbus, GA, USA
Address correspondence to:
Nga Tran
5295 Riverchase Drive, Apt 512, Phenix City, AL 36867,
USA
Message to Corresponding Author
Article ID: 100160Z08NT2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Tran N, Liu J, Harrison P, Jones II J. Pseudotumor cerebri in pregnant obese patient: A case report. J Case Rep Images Obstet Gynecol 2023;9(2):30–34.ABSTRACT
Introduction: Pseudotumor cerebri (PTC), idiopathic intracranial hypertension, is a serious condition that is most associated with pregnancy. It is believed that symptoms are due to increased stroke volume and fluid retention ultimately increasing intracranial pressure. This increased pressure can lead to cerebral edema and dysfunction of the optic nerve fibers. The initial workup for PTC is conducting a computed tomography (CT) or magnetic resonance imaging (MRI) brain scan to rule out structural abnormalities that may induce a headache. A lumbar puncture can be performed to acutely relieve the symptoms and definitively diagnose PTC; however, the definitive treatment is acetazolamide through the inhibition of carbonic anhydrase alleviating intracranial pressure.
Case Report: This case report discusses how a pseudotumor cerebri affected the pregnancy of a 29-year-old female who presented with headache, blurry vision with eye pain, and abdominal pain. Her pregnancy was complicated by several comorbidities. Ultrasound showed a viable intrauterine pregnancy, while an MRI without contrast of the head revealed bilateral papilledema. She was treated with acetazolamide and underwent a primary low transverse cesarean section due to fetal malpresentation and pseudotumor cerebri diagnosis.
Conclusion: It is imperative that symptoms of PTC are recognized as a larger diagnosis and that imaging confirms the increased intracranial pressure. The initial workup for PTC is conducting a CT or MRI brain scan to rule out structural abnormalities that may induce a headache. A lumbar puncture can relieve the symptoms and definitively diagnose PTC. The definitive treatment is acetazolamide through the inhibition of carbonic anhydrase alleviating intracranial pressure.
Keywords: Cerebral edema, Idiopathic intracranial hypertension, Papilledema, Pseudotumor cerebri
Introduction
Pseudotumor cerebri (PTC), also known as idiopathic intracranial hypertension, is a serious condition that is associated with obesity and medications. Although PTC can occur in anyone, it is most associated with pregnancy, which is a state of obesity where large amounts of weight are gained over a short period of time [1],[2]. This case report explores the pathophysiology of PTC, its comorbid outcomes, and the importance of proper identification, management, and treatment.
The exact pathophysiology of PTC is not completely understood. However, it is believed that pregnant women who develop PTC experience symptoms due to increased stroke volume and fluid retention ultimately increasing intracranial pressure [3]. This increased pressure can be harmful, leading to cerebral edema and dysfunction of intracranial structures, such as the optic nerve fibers, which can be compromised by the buildup of intracranial fluid [4]. The resulting cerebrospinal fluid stasis results in increased pressure, leading to symptoms such as headache, vision loss, and a large magnitude of dysfunction in other intracranial functions [5]. Therefore, it is crucial to properly identify and treat PTC, as a significant proportion of those diagnosed with PTC can develop chronic vision loss.
Pseudotumor cerebri is more commonly seen in women, 1.82 per 100,000 individuals, compared to men, 0.034 per 100,000 individuals [6]. During pregnancy, this risk doubles to 4.02 per 100,000 individuals [6]. The clinical features of PTC are identical in both men and women. However, it has been found that although obesity is associated with the development of PTC in women, it is not associated with the development of PTC in men [7]. Many men who were diagnosed with PTC had normal body weight [7].
The identification of a patient with PTC starts with the presentation of a headache. Although the differential regarding headaches is vast, the patient’s sex and body mass index (BMI) should give a clue into whether PTC is higher or lower on the differential diagnosis. The initial workup for PTC is conducting a CT or MRI brain scan to rule out structural abnormalities that may induce a headache. A lumbar puncture can be performed to acutely relieve the symptoms and definitively diagnose PTC; however, the definitive treatment is acetazolamide through the inhibition of carbonic anhydrase alleviating intracranial pressure [8]. Ophthalmological consultation is particularly important as nearly 25% of patients develop visual loss or severe visual impairment in one or both eyes [9]. It was once thought that acetazolamide could cause birth defects; however, this theory has not been successfully proven and acetazolamide is still considered a safe standard of long-term PTC therapy in both pregnant and non-pregnant patients [10], [11]. If headache is present along with a negative brain scan and a lumbar puncture that acutely relieves the symptoms, then PTC should be very high in the differential diagnosis. This triad of symptoms is included in the modified Dandy Criteria that is used to accurately diagnose PTC (Table 1).

Case Report
A 29-year-old G8P4034 female at 34w1d with estimated delivery date (EDD) 03/06/2023 and a history of class III obesity, depression, gestational hypertension, gestational diabetes, fetal macrosomia, post-traumatic stress disorder (PTSD), postpartum psychosis, recurrent pregnancy loss, subchorionic hemorrhage, obstructive sleep apnea, and hypothyroidism presented to triage complaining of headache, abdominal pain, and bilateral eye pain. She reported abdominal pain for two days, located near the sternum, and a burning sensation. She has tried Omeprazole 20 mg, Tums (calcium carbonate), and Tylenol 500 mg every 4 hours without any improvement. She described a headache for one day, a 4/10 intensity, associated with bilateral eye pain, blurry vision, and nausea. She reported fetal movement and denied contractions, vaginal bleeding, and vaginal discharge. She was following up with Maternal Fetal Medicine and was placed on aspirin 81 mg daily, metformin 500mg at night, and NPH 4 units at night.
Upon admission, her vitals were blood pressure (BP) 134/57, pulse 93, temperature 98.1 °F (36.7 °C), respiratory rate (RR) 16, height 5’7” (1.702 m), weight 280 lb (127 kg), BMI 43.85 kg/m2, and last normal menstrual period (LNMP) 05/30/2022. Her prenatal labs included blood type B+, antibody was negative, human immunodeficiency virus (HIV) was non-reactive (NR), Hepatitis B was negative, rapid plasma reagin (RPR) was NR, Rubella Immune, Hgb was electro-normal, Hepatitis C virus (HCV) was NR, thyroid stimulating hormone (TSH) was 1.51, free thyroxine (FT4) was 0.69, thyroid function test (TFT) was euthyroid, and a normal thyroid ultrasound (US). An ultrasound was performed which showed a single viable intrauterine pregnancy, fetus in the cephalic presentation, fetal heart rate (FHR) was 133 bpm, placenta was fundal and grade 2, and fluid was normal with an amniotic fluid index (AFI) of 17.3 cm with deepest vertebral pocket (DVP) of 5.1. A biophysical profile was performed based on the documented indications with a score of 8/8 and antenatal testing was reassuring. An MRI brain without contrast showed mild increased fluid in the optic nerve sheaths bilaterally with papilledema and no intracranial abnormality. Magnetic resonance imaging venogram head without contrast was normal.
The patient’s treatment plans included admission until an anticipated delivery on 03/06/2023, fetal growth US every four weeks until delivery, and continued routine prenatal care. Her blood pressure was stable during admission but continued to be monitored serially due to concern for possible preeclampsia. Complete blood count (CBC), comprehensive metabolic panel (CMP), and protein creatinine were within normal limits and 24-hour urine protein was 194. Her point-of-care testing (POCT) since admission ran between 87 and 147 and her glucose was monitored during fasting and 2 hours postprandial. She was started on betamethasone 12 mg q24 hours for two doses for risk of preterm birth, Tylenol pro re nata (PRN) for headache, Morphine 2g q4 hours for pain, and Pepcid PRN for gastroesophageal reflux disease (GERD). She continued Aspirin 81 mg daily, metformin 500 mg nightly, and NPH 4 units nightly.
Neurology ordered acetazolamide 500 mg BID and a lumbar puncture was recommended to confirm diagnosis of pseudotumor cerebri. However, the patient declined the lumbar puncture and deferred it to after delivery. After taking acetazolamide, the patient developed an allergic reaction, and it was discontinued but neurology ordered for the patient to be premedicated with Benadryl prior to taking acetazolamide. Anesthesiology performed a spinal anesthesia at 34w2d which resolved her headache and blurry vision. She was scheduled for a primary low transverse cesarean section at 34w4d due to fetal malpresentation and symptomatic pseudotumor cerebri. Acetazolamide was discontinued prior to surgery. She delivered a healthy male infant who weighed 5 lb 5.9 oz and was placed in the neonatal intensive care unit (NICU) for further monitoring. During postpartum day 2, she was discharged with Lovenox 40 mg daily for seven days and oxycodone 5 mg for pain. The patient returned for her 2-week follow-up appointment and reported that she did not have any symptoms such as headache or change in vision. However, she reported feeling depressed and requested to be started on Zoloft 50 mg due to her history of PTSD and postpartum psychosis. At her 6-week follow-up appointment, she was feeling much better while on Zoloft and requested to continue it. She continued to deny any headache or any change in vision.
Discussion
This patient had multiple risk factors associated with pseudotumor cerebri. In addition to pregnancy, other risk factors include female sex and certain medications, such as Danazol, Growth Hormones, and Tetracyclines. Excessive Vitamin-A intake has also been documented to not only consider patients who are obese, but also those who are dieting and losing weight as many weight-loss diets consist of Vitamin-A rich foods that could lead to PTC [12].
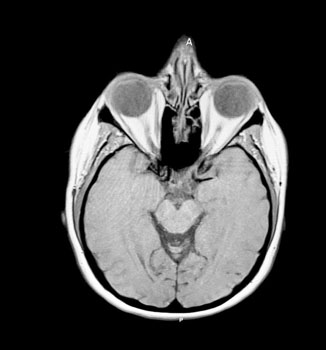
During the diagnostic process, several differentials were considered for this patient, including preeclampsia with severe features, an intracranial mass, and hypoparathyroidism. However, based on the patient’s history, comorbidities, and physical exam findings, a diagnosis of PTC was made. The patient’s symptoms and presentation met the criteria for diagnosing PTC, as outlined in the Dandy Criteria (Table 1). The patient had initially presented with a headache, blurry vision, and eye pain. As a result, an MRI without contrast of the head was performed, revealing bilateral increased fluid in the optic nerve sheaths with papilledema present (Figure 1). It is crucial to highlight that patients with suspected diagnosis of PTC should always undergo an ophthalmological consultation, as a fraction of these individuals may experience severe vision loss [13]. A question to consider moving forward is if treatment with a lumbar puncture would have been beneficial for the pregnancy resulting in a longer gestation and a later delivery date?
Conclusion
This case report discusses the complications that arise with a pseudotumor cerebri during pregnancy. The patient presented with headache, blurry vision, and abdominal pain and has a history of obesity, thus pseudotumor cerebri should be considered. Confirmation of papilledema on examination suggested increased intracranial pressure. While a lumbar puncture would have been both diagnostic and therapeutic for this patient, she deferred the procedure until after delivery. Thus, acetazolamide was prescribed to decrease cerebrospinal fluid (CSF) production and a spinal block helped alleviate the patient’s symptoms. The patient did have an allergic reaction to a previously unknown allergy, acetazolamide, but that was quickly noticed by the neurologist and resolved with the addition of Benadryl. In addition to the workup that was done, the patient could have undergone imaging studies to evaluate for the possibility of structural abnormalities that induced her headache. Three days following admission, the patient successfully delivered a healthy baby boy via cesarean section. The patient was stable and followed up for a 6-week postpartum visit.
With pseudotumor cerebri being an uncommon diagnosis, it was imperative that the symptoms were recognized as a much larger diagnosis and that imaging was done promptly to affirm the increased intracranial pressure. If consent for a lumbar puncture were given, the patient may have experienced more symptomatic relief. However, she ultimately received the definitive treatment, acetazolamide. This patient’s presentation is incredibly important due to the seemingly stable condition the patient presented with in juxtaposition to the seriousness of the state of her health.
REFERENCES
1.
Abu-Raya B, Michalski C, Sadarangani M, Lavoie PM. Maternal immunological adaptation during normal pregnancy. Front Immunol 2020;11:575197. [CrossRef]
[Pubmed]

2.
Mor G, Cardenas I. The immune system in pregnancy: A unique complexity. Am J Reprod Immunol 2010;63(6):425–33. [CrossRef]
[Pubmed]
3.
Alves S, Sousa N, Cardoso LÍ, Alves J. Multidisciplinary management of idiopathic intracranial hypertension in pregnancy: Case series and narrative review. Braz J Anesthesiol 2022;72(6):790–4. [CrossRef]
[Pubmed]
4.
Chih A, Patel B. Idiopathic intracranial hypertension in pregnancy. Fed Pract 2015;32(11):36–40.
[Pubmed]
5.
Donahue SP. Recurrence of idiopathic intracranial hypertension after weight loss: The carrot craver. Am J Ophthalmol 2000;130(6):850–1. [CrossRef]
[Pubmed]
6.
Kesler A, Gadoth N. Epidemiology of idiopathic intracranial hypertension in Israel. J Neuroophthalmol 2001;21(1):12–4. [CrossRef]
[Pubmed]
7.
Biousse V, Bruce BB, Newman NJ. Update on the pathophysiology and management of idiopathic intracranial hypertension. J Neurol Neurosurg Psychiatry 2012;83(5):488–94. [CrossRef]
[Pubmed]
8.
Al-Saleem AI, Al-Jobair AM. Possible association between acetazolamide administration during pregnancy and multiple congenital malformations. Drug Des Devel Ther 2016;10:1471–6. [CrossRef]
[Pubmed]
9.
Corbett JJ, Savino PJ, Thompson HS, et al. Visual loss in pseudotumor cerebri. Follow-up of 57 patients from five to 41 years and a profile of 14 patients with permanent severe visual loss. Arch Neurol 1982;39(8):461–74. [CrossRef]
[Pubmed]
10.
Digre KB, Varner MW, Corbett JJ. Pseudotumor cerebri and pregnancy. Neurology 1984;34(6):721–9. [CrossRef]
[Pubmed]
11.
Moore DM, Meela M, Kealy D, Crowley L, McMorrow R, O’Kelly B. An intrathecal catheter in a pregnant patient with idiopathic intracranial hypertension: Analgesia, monitor and therapy? Int J Obstet Anesth 2014;23(2):175–8. [CrossRef]
[Pubmed]
12.
Wall M, Lee AG. Idiopathic intracranial hypertension (pseudotumor cerebri): Prognosis and treatment. UpToDate 2017.
13.
Tang RA. Management of idiopathic intracranial hypertension in pregnancy. MedGenMed 2005;7(4):40.
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
Amirah Nicole Hill, DO contributed to the work but does not qualify for authorship.
Author ContributionsNga Tran - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
James Liu - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Paige Harrison - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jefferson Jones II - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Nga Tran et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}