 |
Case Report
Left labial edema after kidney transplantation
1 Loma Linda University School of Medicine, Loma Linda, CA, USA
2 DO, MPH, FACOG, Assistant Professor, Department of Obstetrics and Gynecology, Loma Linda University Health, Loma Linda, CA, USA
Address correspondence to:
Andrea Salcedo
Loma Linda University Health, Loma Linda, CA,
USA
Message to Corresponding Author
Article ID: 100164Z08AM2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Maidan A, Salcedo A. Left labial edema after kidney transplantation. J Case Rep Images Obstet Gynecol 2023;9(2):47–50.ABSTRACT
Introduction: The differential diagnoses for labial edema are diverse. Labial edema after a kidney transplantation requires a thorough understanding of the various common and uncommon causes. Comprehensive history taking, physical examination, and awareness of anatomical knowledge will lead to proper diagnosis and treatment.
Case Report: We present the case of an 18-year-old female with a past medical history of end stage renal disease secondary to bilateral atrophic kidneys and grade 3 vesicoureteral reflux status post deceased donor kidney transplant. She presented to the emergency department on postoperative day 5 due to uncontrolled hypertension and significant left labia minora edema with extreme pain to palpation. Gynecology evaluation and consultation determined the lesion was not suspicious for infection, abscess, or hematoma, and supportive care and conservative measures were initiated. Computed tomography (CT) was performed to rule out other causes of the anasarca, and after conservative management and doses of furosemide on hospital days 3 and 4, the patient showed improvement of the labial edema and blood pressure.
Conclusion: A comprehensive differential diagnoses with reliance on anatomy and potential anomalies will lead clinicians and surgeons to properly treat potential postoperative complications. In this case, a thorough understanding of Mullerian anatomy and hemodynamic balance with implementation of conservative measures postoperatively resulted in resolution of the patient’s symptoms.
Keywords: Canal of Nuck, End stage renal disease, Kidney transplant, Labia edema, Mullerian anomaly
Introduction
An isolated cause of labia minora edema in an adolescent can be a rare finding, and various differential diagnoses may necessitate exploring until the underlying etiology is found. Embryological anomalies, fluid overload, or different medical conditions may all play a role in causing this issue. It is important for clinicians to thoroughly investigate and treat with the root cause in mind. History, physical examination, and when warranted, imaging studies are necessary for diagnosis and treatment. A broad differential diagnosis with a thorough understanding of anatomy is vital for unusual presentations of labial edema. We present an atypical presentation of labia minora edema in an adolescent patient.
Case Report
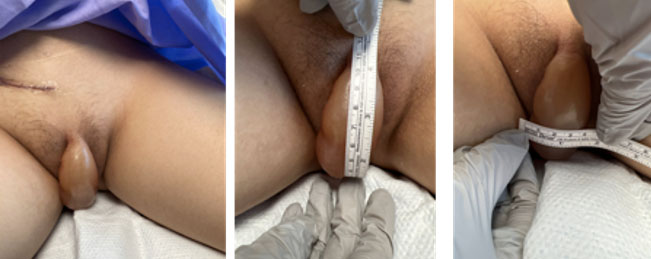
We present the case of an 18-year-old female with a past medical history of end stage renal disease secondary to bilateral atrophic kidneys and grade 3 vesicoureteral reflux status post deceased donor kidney transplant. She had a history of bilateral ureteral implantation surgery 13 years prior due to bilateral duplicated collecting systems, and most recently, a deceased donor kidney transplant (DDKT) seven days before presentation. She was on amlodipine 5 mg and losartan 12.5 mg orally daily. Her family history was significant for achondroplasia, autism, alcoholism, and liver disease. Prior to her kidney transplantation, she underwent daily peritoneal dialysis. Peritoneal dialysis was concluded two days before kidney transplantation and the peritoneal dialysis catheter was removed intraoperatively. She had an uncomplicated postoperative course with good graft function and was discharged home on postoperative day (POD) 3. During routine postoperative visit five days after surgery, she was noted to have significant left labia minora edema, measuring 11 cm × 4 cm in size (Figure 1) with extreme pain to palpation. The patient recalled the edema slowly initiated on postoperative day 3, and progressed abruptly on POD #4–5. Her blood pressure at this time was 184/128 and her heart rate was 75 bpm. Her temperature was 98 °F. Given her clinical presentation, she was referred to the Emergency Department (ED) for evaluation of left labial edema, related pain, as well as uncontrolled hypertension.
In the Emergency Department, her blood pressure was treated with amlodipine 5 mg PO. Her blood pressure control improved to 146/89 mmHg. She was noted to have an Enterobacter clocae urinary tract infection treated with intravenous cefepime. Pediatric Urology was called to discuss possible removal of the ureteral stent in the setting of urinary tract infection (UTI). However, Urology recommended gynecology consultation to treat her labial swelling prior to stent removal due to difficulty visualizing the urethra with the degree of labial swelling. The decision was made to defer inpatient ureteral stent removal given improved leukocytosis with broadened antibiotics and overall clinical stability from the infection standpoint. She was admitted to the hospital under the transplantation service.
Upon gynecology consultation, the labial edema was noted to be 11 cm × 4 cm, the skin was noted to be taut and translucent upon light transillumination, and was not indurated. The Gynecology service considered a differential diagnoses of dependent labial edema due to peritoneal communication of the canal of Nuck, versus post-surgical seroma from surgery, leading to mons/labia minora edema. It was determined that the lesion was not suspicious for infection, abscess, or hematoma given the translucency of the lesion. Initial recommendation of supportive care and conservation measures with alternation of ice and heat packs on the affected area, compression of the site, sitz baths, barrier cream, lidocaine spray, and pelvic elevation for resorption of dependent edema were initiated. Surgical or drainage intervention was not recommended due to concern of possible infectious seeding into the peritoneal cavity that could threaten her recent kidney transplantation. After one day of adherence to these measures, the lesion was noted to show clinical improvement. However, given the uncertain etiology of the swelling, it was decided to perform a CT abdomen/pelvis, which revealed a subcutaneous fluid collection of the left labia with no clear tract seen from the abdomen and mild abdominal anasarca. Given these results, the team discussed with the patient the options of continued conservative measures as described above, or the option of drainage of the swollen area. However, since the patient experienced notable clinical improvement with conservative measures, she opted to continue this management.
On the hospital day 3, although asymptomatic from her UTI, she had worsening leukocytosis. Thus, cefepime was changed to piperacillin-tazobactam to broaden coverage given her worsening leukocytosis. After these adjustments were made, she began to have down trending leukocytosis. After consultation with pediatric nephrology, intravenous furosemide was given after the patient was noted to be approximately 7 kg over her dry weight before transplantation surgery. It was suspected to be contributing to the mild anasarca as well as the hypertension which had originally brought the patient to the ED. Thus, furosemide 40 mg intravenously (IV) was administered, with a maintenance goal of negative fluid balance. An additional dose of furosemide was given on hospital day 4 due to noted improvement of the labial edema and blood pressure. On the day of discharge, the anasarca, labial edema, and hypertension had improved from admission with the above interventions. Thus, the decision was made to not pursue further imaging or drainage of the fluid collection, and she was sent home with instructions to follow up with pediatric nephrology in two days.
She was seen in the outpatient setting nine days after hospital discharge and was found to have resolution of labial edema. She was recommended to follow-up in three months due to primary amenorrhea in the setting of a hypoplastic uterus without visualized ovaries seen on US or magnetic resonance imaging (MRI).
Discussion
In the case of the patient discussed above, several differential diagnoses were considered. Specifically, postsurgical seroma, leading to mons/labia minora edema versus peritoneal leak into processus vaginalis from peritoneal dialysis leak. Labial abscess was not considered because the skin was not erythematous or indurated, and was translucent upon light illumination. Additionally, the patient displayed no fever, chills, or other clinical signs of related infection. Ultimately, her competing diagnoses were peritoneal serous fluid, peritoneal urine accumulation via the canal of Nuck, and anasarca. The canal of Nuck, first described by the Dutch anatomist Anton Nuck in 1691, is a peritoneal evagination that descends along with the round ligament to the labia majora during a female fetus’ development [1],[2]. The canal normally obliterates from around the seventh month of gestation up to one year of age. However, if persists, elevates the risk for hydrocele or even hernia development [1],[2],[3].
General medical conditions can also result in edema formation [4],[5],[6]. Changes in normal fluid homeostasis that cause an increased secretion or impaired removal of fluid can cause edema. In the case of kidney failure, there is impaired removal of fluid from the body, causing an increase in intravascular hydrostatic pressure and edema [4],[6], [7]. Areas with loose, distensible skin are particularly at risk for fluid collection, the genitalia included [7].
Surgical procedures may also lead to genital edema. Approximately 4–10% of patients on peritoneal dialysis are found to have acute genital edema, causes of which include leaks from the catheter insertion site, a general fluid overload state, hernias, peritoneal tears, or malignancy [5]. Operative laparoscopy has also been found to cause both bilateral and unilateral vulvar edema. This can be due to a patent canal of Nuck as discussed above, which would cause unilateral labial edema [2],[7]. Another proposed mechanism is escape of solution from a lower trocar site during a laparoscopic procedure, which tracks along subcutaneous planes to reach dependent regions of the body (e.g., the vulva) [7].
First-line management of vulvar edema in this case is treatment of the underlying medical condition. In the case of fluid-overload state, diuretics should be considered as an option [4],[7]. Conservative management includes pelvic elevation of the genital area, which decreases fluid accumulation in dependent regions, helping to lessen edema formation. Compression of the site as well as manual manipulation/massage also aids in decongesting the area [7].
Given proximal timing of labial edema onset to the recent transplant surgery, it was hypothesized the left labial edema was related to recent kidney transplantation surgery. Given her recent peritoneal dialysis status, it was plausible for accumulating dialysate fluid to communicate via the inguinal canal through the canal of Nuck [5]. Alternatively, the labial edema may have been a function of anasarca. Computed tomography imaging did not reveal a clear tract from the peritoneal cavity into the vulvar area, yet magnetic resonance imaging is the imaging modality of choice to evaluate reproductive soft tissue structures. Furthermore, as previously mentioned, the canal terminates at the labia majora, which was not the affected labia in this presentation [1],[2]. Thus, the patient may have presented with swelling of the labia majora, not the labia minora as in this case. Given the patient presented with labia minora, not majora, edema may be a distortion of her anatomy, as indicated by her Mullerian anomaly.
Although a definitive cause of the patient’s swelling was not found, conservative management proved to resolve her symptoms. With understanding of postoperative homeostatic mechanisms and anatomical variation, invasive treatment options were ultimately avoided. Furthermore, the patient was content with these options, and the shared goal of relieving her symptoms was reached.
Conclusion
A wide differential diagnosis with awareness of both infectious and anatomical variants can lead to a focused treatment method in the postoperative period. In this case a cautious treatment approach was implemented, understanding that invasive treatment measures could threaten her recent transplantation. In this case, conservative measures led to resolution of her postoperative complication.
REFERENCES
1.
Fikatas P, Megas IF, Mantouvalou K, et al. Hydroceles of the canal of Nuck in adults-diagnostic, treatment and results of a rare condition in females. J Clin Med 2020;9(12):4026. [CrossRef]
[Pubmed]

2.
Keeratibharat N, Chansangrat J. Hydrocele of the canal of Nuck: A review. Cureus 2022;14(4):e23757. [CrossRef]
[Pubmed]
3.
Vinoth T, Lalchandani A, Bharadwaj S, Pandya B. Revisiting the clinico-radiological features of an unusual inguino-labial swelling in an adult female. Int J Surg Case Rep 2022;98:107515. [CrossRef]
[Pubmed]
4.
Abassi Z, Khoury EE, Karram T, Aronson D. Edema formation in congestive heart failure and the underlying mechanisms. Front Cardiovasc Med 2022;9:933215. [CrossRef]
[Pubmed]
5.
Jorge J, Haggerty SP. Acute genital edema during peritoneal dialysis: A review for surgeons. Am Surg 2015;81(11):1187–94.
[Pubmed]
6.
Siddall EC, Radhakrishnan J. The pathophysiology of edema formation in the nephrotic syndrome. Kidney Int 2012;82(6):635–42. [CrossRef]
[Pubmed]
7.
Amankwah Y, Haefner H. Vulvar edema. Dermatol Clin 2010;28(4):765–77. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Alexandra Maidan - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Andrea Salcedo - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Alexandra Maidan et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}