 |
Case Report
Unveiling hemorrhagic shock from partial hydatidiform mole: A case study at Beja maternity ward
1 Tunis el Manar University, Beja Maternity Center, Tunis, Tunisia
Address correspondence to:
Montacer Hafsi
Medical Resident in Gynecology and Obstetrics, Bardo, Tunis 2000,
Tunisia
Message to Corresponding Author
Article ID: 100166Z08MH2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Hafsi M, Smaoui M, Moussi M, Mastouri S, Najar S, Dridi F, Mourali M. Unveiling hemorrhagic shock from partial hydatidiform mole: A case study at Beja maternity ward. J Case Rep Images Obstet Gynecol 2023;9(2):55–58.ABSTRACT
Introduction: Partial hydatidiform mole (PHM) is one of the gestational trophoblastic diseases characterized by cystic transformation of chorionic villi, retaining recognizable placental morphology, and an amniotic cavity with a fetus. Its incidence is approximately 3 per 1000 pregnancies. Symptomatology is marked by the occurrence of metrorrhagia following amenorrhea, most commonly in the first trimester and rarely in the second trimester.
Case Report: We present a case of threatened premature delivery complicated by hemorrhagic shock, revealing a partial hydatidiform mole at 23 weeks of gestation. The diagnosis of PHM in the context of such clinical presentation underscores the importance of recognizing this rare entity early in pregnancy to facilitate appropriate management and optimize maternal and fetal outcomes.
Conclusion: The provided text has already been divided into the Introduction, Case Report, and Conclusion sections as outlined above.
Keywords: Gestational trophoblastic disease, Hemorrhagic shock, Metrorrhagia, Partial hydatidiform mole, Pregnancy complications
Introduction
Partial hydatidiform mole (PHM) is categorized among gestational trophoblastic diseases, characterized by cystic transformation of chorionic villi while maintaining recognizable placental structure and an amniotic cavity with a fetus. Its incidence is estimated at approximately 3 per 1000 pregnancies. Symptomatically, metrorrhagia typically follows amenorrhea, predominantly occurring during the first trimester and rarely during the second trimester [1].
The genetic origin of PHM corresponds to triploid conception with an additional chromosomal set of paternal origin. This complex genetic configuration underlies the unique pathogenesis of PHM, contributing to its distinct clinical presentation and outcomes [2].
In this report, we present a case of threatened premature delivery complicated by hemorrhagic shock, unveiling a partial hydatidiform mole at 23 weeks of gestation. This presentation underscores the critical importance of early recognition and appropriate management of PHM, particularly in cases with severe clinical manifestations. Early diagnosis and intervention are pivotal for optimizing maternal and fetal outcomes and guiding subsequent medical decision-making.
Case Report
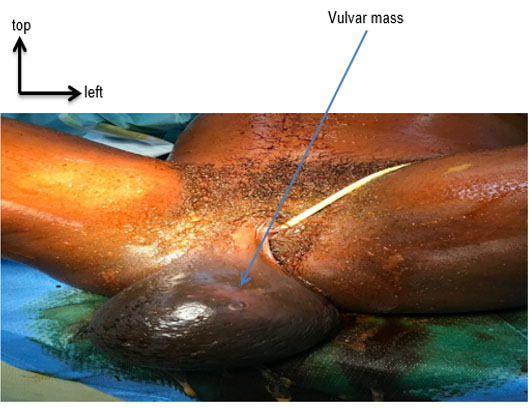
Our patient, a 27-year-old woman with no prior medical history, presented with acute pelvic pain and profuse abnormal uterine bleeding at 23 weeks of gestation. She had a history of a previous miscarriage that was managed with surgical evacuation. The severity of her condition led to her direct transfer by the Emergency Medical Services. Due to her compromised state, obtaining a detailed medical history was challenging, and she was promptly taken to the operating room.
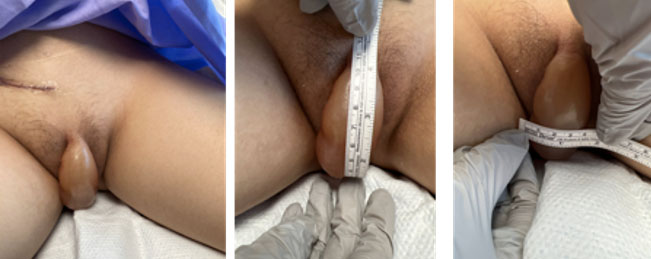
Upon examination, the patient exhibited cutaneous and mucosal pallor. Her blood pressure was measured at 75/50 mmHg, and her heart rate was 120 beats per minute. A significant amount of externalized, clotted red bleeding was observed during the vaginal examination. The cervix was dilated to 1 cm and posteriorly elongated.
An ultrasound examination revealed a fetus with absent cardiac activity, anhydramnios, and a placenta with no evidence of detachment, hypertrophy, or vesicular appearance (Figure 1).
In the operating room, the patient’s hemoglobin level was found to be 4.9 g/dL. An emergency cesarean section was performed to ensure maternal well-being. Intraoperatively, the uterus appeared enlarged and consistent with a gravid state. A segmental incision was made, resulting in the delivery of a morphologically normal female fetus weighing 450 grams but without signs of life.
The placenta exhibited a vesicular appearance and weighed 2520 grams. An anatomopathological examination of the placenta confirmed the diagnosis of a partial hydatidiform mole (PHM) (Figure 2).
In the postpartum period, the weekly beta-human chorionic gonadotropin (bhCG) levels showed a declining trend.


Discussion
The recognition and comprehensive understanding of hydatidiform moles (HMs) play a pivotal role in guiding clinical management and predicting patient outcomes. Within the spectrum of gestational trophoblastic diseases (GTDs) [3], HM constitutes a significant entity characterized by its unique histopathological features and clinical implications. In this context, the present discussion delves deeper into the intricate aspects of HM, particularly focusing on the partial hydatidiform mole (PHM), as exemplified by our presented case [4].
Hydatidiform moles are aberrations of fertilization and embryonic development, resulting in an abnormal proliferation of trophoblastic tissue within the gestational sac. In the case of PHM, a distinct fertilization pattern emerges, involving the fertilization of an empty ovum by two spermatozoa, leading to a triploid chromosomal composition. This genetic configuration underpins the unique pathogenesis of PHM, influencing its clinical presentation and behavior [2].
Histologically, PHM is characterized by placental villi exhibiting focal edema, areas of degeneration, and a pathological proliferation of trophoblastic cells [2]. This histopathological heterogeneity translates into a spectrum of clinical presentations. While the fetus is often nonviable in PHM, there have been documented instances of a viable, albeit small, fetus. In rare cases, a full-term live birth may even occur, adding to the complexity of PHM’s clinical manifestations [5].
The diagnosis of PHM, guided by clinical presentation, ultrasound findings, and histopathological examination, is pivotal in determining appropriate management strategies. Patients with PHM typically present with vaginal bleeding, uterine enlargement, and elevated serum hCG levels. Ultrasonography plays a crucial role in visualizing characteristic features, such as the heterogeneous appearance of placental tissue and the absence of the characteristic “snowstorm” pattern seen in complete moles [6].
Timely and appropriate management is vital in ensuring optimal outcomes for patients with PHM. Uterine evacuation is often necessary, particularly in cases of symptomatic disease or when persistent trophoblastic tissue is suspected. In the presented case, the urgency of the situation warranted an emergency cesarean section to safeguard maternal well-being. Postoperative care involves diligent follow-up, monitoring serum hCG levels, and assessing for potential complications such as persistent trophoblastic disease [7].
While the prognosis for PHM is generally favorable, vigilance and proper follow-up remain paramount due to the potential for persistent trophoblastic disease. In cases of non-resolving or recurrent trophoblastic disease, additional therapeutic measures, such as chemotherapy, may be considered to prevent potential complications and optimize patient outcomes [8].
In conclusion, the intricate interplay between genetics, histopathology, and clinical presentation underscores the complexity of partial hydatidiform moles within the realm of gestational trophoblastic diseases. Through a thorough understanding of its distinct characteristics, clinicians can make informed decisions regarding diagnosis, management, and follow-up. The presented case highlights the importance of early recognition and tailored interventions, ultimately contributing to improved maternal health and enhanced patient care [9].
Conclusion
The case report highlights the complex nature of partial hydatidiform moles (PHM) within gestational trophoblastic diseases. Partial hydatidiform mole, characterized by triploid chromosomal composition and distinct histopathological features, presents diagnostic challenges and diverse clinical presentations. Clinical symptoms, including vaginal bleeding and elevated hCG levels, reflect underlying trophoblastic proliferation. Early and accurate diagnosis through clinical suspicion, ultrasound, and histopathology is crucial for effective management.
Management of PHM necessitates tailored interventions. Uterine evacuation, as demonstrated in the case, addresses immediate health risks and potential persistent trophoblastic disease. Postoperative monitoring, including hCG measurements, aids in detecting recurrence or complications. While prognosis is generally favorable with prompt intervention, vigilant follow-up is essential due to potential complications.
A multidisciplinary approach is vital, integrating obstetric, pathology, and follow-up aspects for comprehensive patient care. Understanding the intricate genetic, histopathological, and clinical nuances empowers clinicians to make informed decisions. This case underscores the significance of recognizing, managing, and continuously monitoring PHM to optimize maternal health, patient well-being, and expand our understanding of this condition.
REFERENCES
1.
Ghassemzadeh S, Farci F, Kang M. Hydatidiform Mole. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
[Pubmed]

2.
Capozzi VA, Butera D, Armano G, et al. Obstetrics outcomes after complete and partial molar pregnancy: Review of the literature and meta-analysis. Eur J Obstet Gynecol Reprod Biol 2021;259:18–25. [CrossRef]
[Pubmed]
3.
Mrozowska J. Partial hydatiform mole. [Article in Polish]. Ginekol Pol 1960;31:675–8.
[Pubmed]
4.
Ben Salah I, Najeh H, Dhouha B, Oueslati H. Partial hydatiform mole associated with a pregnancy at 22 weeks of Amenorrhea. J Obstet Gynaecol Can 2017;39(7):511. [CrossRef]
[Pubmed]
5.
Chelli D, Dimassi K, Bouaziz M, et al. Imaging of gestational trophoblastic disease. [Article in French]. J Gynecol Obstet Biol Reprod (Paris) 2008;37(6):559–67. [CrossRef]
[Pubmed]
6.
Indraccolo U, Giannone L, Canonico S, Giannone E. Sensitivity, specificity, predictive positive and negative value of the main clinical signs and symptoms of hydatiform mole. [Article in Italian]. Minerva Ginecol 2006;58(3):249–54.
[Pubmed]
7.
Gadducci A, Lanfredini N, Cosio S. Reproductive outcomes after hydatiform mole and gestational trophoblastic neoplasia. Gynecol Endocrinol 2015;31(9):673–8. [CrossRef]
[Pubmed]
8.
Golfier F, Clerc J, Hajri T, et al. Contribution of referent pathologists to the quality of trophoblastic diseases diagnosis. Hum Reprod 2011;26(10):2651–7. [CrossRef]
[Pubmed]
9.
de Andrade JM. Hydatidiform mole and gestational trophoblastic disease. [Article in Portuguese]. Rev Bras Ginecol Obstet 2009;31(2):94–101. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Montacer Hafsi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Maroua Smaoui - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Marwa Moussi - Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sinda Mastouri - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Souhir Najar - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Faten Dridi - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mechaal Mourali - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Montacer Hafsi et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}