 |
Case Report
Spinal stenosis secondary to engorged Batson’s plexus in pregnancy
1 Promedica Neuroscience Institute, Promedica Toledo Hospital, University of Toledo, Toledo, OH, USA
Address correspondence to:
Brandon Sharkey
and Brooklyn McGue,
Promedica Neuroscience Institute, Promedica Toledo Hospital, University of Toledo, Toledo, OH 43606
USA
Message to Corresponding Author
Article ID: 100167Z08BS2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Sharkey B, McGue B, Conner K, Brodsky C, Azeem N, Brodsky B, Gabel B. Spinal stenosis secondary to engorged Batson’s plexus in pregnancy. J Case Rep Images Obstet Gynecol 2024;10(1):1–5.ABSTRACT
Introduction: Lumbar venous plexus engorgement is a rare condition. It can be caused by compression or thrombosis of abdominal venous structures. Proper diagnosis requires attention to radiologic details in order to rule out other disc pathologies. Treatment of pregnancy-induced venous plexus engorgement includes positional maneuvers to prevent obstruction of venous return. Complete resolution of symptoms is achieved through delivery.
Case Report: We present the case of a patient with recurrent lower extremity weakness and pain secondary to spinal stenosis caused by epidural venous plexus engorgement in multiple separate pregnancies.
Conclusion: This case highlights a unique recurrent presentation with earlier onset and increasingly more severe symptoms with each subsequent pregnancy.
Keywords: Pregnancy, Spinal stenosis, Spinal venous plexus
Introduction
The vertebral venous plexus was originally described by Gilbert Breschet as a network of valveless veins spanning the length of the spine. In 1940, Oscar Batson described the function of this plexus in the spread of pelvic metastases [1],[2]. Additionally, its role in providing an alternate route for venous return when the inferior vena cava (IVC) is occluded has been described as well. There are many conditions that can affect the abdominal and pelvic venous structures including thrombosis, malignancies, and pregnancy [3]. Reports have shown engorgement of the venous plexus from occlusion of the IVC in third-trimester pregnancies. Some cases were asymptomatic, others led to acute onset of low back pain, radicular pain, or leg weakness [4],[5],[6],[7]. Cases have shown symptom improvement after delivery [8]. However, there have been no reported cases with IVC obstruction by a gravid uterus occurring earlier than the third trimester. We present a patient with recurrent engorgement of the vertebral venous plexus in consecutive pregnancies leading to bilateral radicular pain occurring at 35 weeks, 29 weeks, and then 19 weeks gestation.
Case Report
The patient is a 21-year-old who presented in her second trimester of her third pregnancy with complaints of bilateral lower extremity paresthesia, minor saddle anesthesia without bowel or bladder incontinence, and subjective weakness for the past month. Her symptoms were worsened with ambulation. She had previously carried two other pregnancies at other hospitals and had presented with similar symptoms that resolved after delivery. Interestingly, the patient experienced similar symptoms during her first pregnancy starting around 35 weeks gestation. She again developed similar symptoms starting around 29 weeks with her second pregnancy.
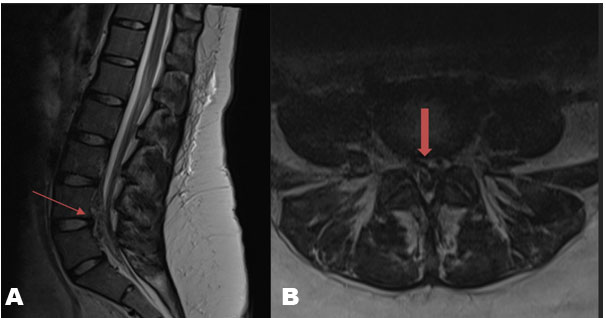
Physical exam was notable for 5/5 strength in the patient’s upper extremities and 4/5 strength with knee extension, plantarflexion, dorsiflexion, extensor hallucis longus, hip abduction, and hip adduction bilaterally. Reflexes were 2+ at the biceps, triceps, patella, and Achilles bilaterally. No Hoffman’s reflex, clonus, or Babinski sign was appreciated. Sensation to light touch, pinprick, and temperature was decreased symmetrically below the level of the mid-thigh with intact proprioception and vibration. Straight leg raise and FABER testing were negative. Initial magnetic resonance imaging (MRI) of the lumbar spine revealed severe canal stenosis extending from the L3–L4 disc space through S1 disc space secondary to an anterior epidural heterogeneous signal abnormality that was predominately posterior to the L4 and L5 vertebral bodies (Figure 1). This appearance was considered most consistent with epidural venous plexus engorgement. A transabdominal ultrasound was then performed that demonstrated a single intrauterine pregnancy with an estimated fetal weight 461 g, corresponding to a gestation age of 23 w 4 d.
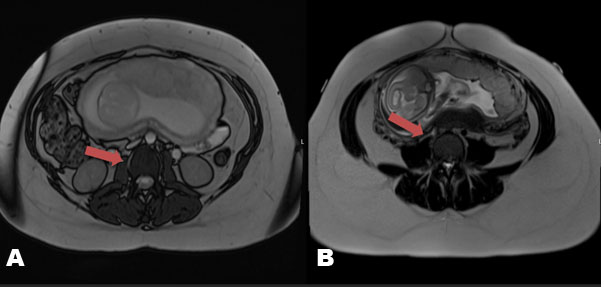
Given concern for venous plexus engorgement, an MR venography of the pelvis was ordered and revealed compression of the inferior vena cava and proximal portions of the common iliac veins at the L3 through L5 levels secondary to the patient’s gravid uterus (Figure 2). Small bilateral collateral veins extending from the distal common iliac veins to the epidural venous plexus at the L5 and S1 levels were also identified. Magnetic resonance angiography of the pelvis was unremarkable. At this point, no neurosurgical intervention was recommended. In discussion with our obstetrics colleagues, it was decided to keep the patient on relative bed rest in the left lateral decubitus positioning as much as possible. Following a three day stay in the hospital, she was discharged with plans to follow up with neurology and her obstetrician for further prenatal care.
Two months following discharge from the hospital, the patient presented to the Obstetrics Emergency Department, now at 30 weeks and 5 days gestation, with complaints of worsening lower back and left lower leg pain. The patient’s pain improved with lidocaine patches and conservative management, and she was discharged the following day. Acetaminophen and lidocaine patches were prescribed for pain management at home. She ultimately delivered via C-section at 39 weeks, which was roughly 16 weeks after her initial neurologic presentation. The post-operative C-section course was uneventful, and she noted significant improvement of her lower extremity symptoms after delivery. The final diagnosis was concluded to be spinal stenosis secondary to an engorged Batson’s plexus.
Discussion
Previous case studies of patients with venous plexus engorgement have revealed different treatment strategies depending on the etiology or suspicion of venous plexus engorgement. In the case of venous plexus engorgement due to pregnancy, management of symptoms and disease course are different due to etiology. As mentioned above, many patients experience venous plexus engorgement from thrombosis and mass effect from other etiologies like tumors.
A 47-year-old male with leukocytosis due to streptococcus viridans septicemia presented with two weeks of left lower extremity paraparesis and urinary incontinence [9]. He was found to have venous thrombosis for which he was receiving antibiotics, anticoagulation, and a stent. During stent placement his venous blood clot extended from the left popliteal vein to the IVC demonstrating significant filling defects due to the occlusion. Lumbar MRI was not specific for epidural venous plexus engorgement and thus the patient underwent subsequent laminectomy for the mass in the L5-S1 epidural space. During the procedure, the mass was revealed to be a significantly engorged venous plexus rather than an abscess. Due to the compressive nature of this engorged plexus, it was cauterized and resected. The patient had resolution of symptoms within 24 hours and continued to have resolution of symptoms even eight months later [9].
Interestingly, MRI of venous plexus engorgement may mimic disk herniation. Thus, there have been reports of operations performed for radiculopathy presumed to be due to herniated discs where all that was found intraoperatively was dilated epidural veins [10],[11]. In fact, one study demonstrated 25 different reports prior to 2019 documenting 55 cases of venous plexus engorgement that presented as disk herniations [12]. The most common initial presentation was radiculopathy followed by symptoms of spinal stenosis and cauda equina syndrome [12].
A different case study of a 37-year-old male with a history of poorly controlled type II diabetes was reported in 2017 [13]. He presented with acute kidney injury, transverse myelitis, as well as paresthesia of his bilateral lower extremities. He did not have any incontinence but had 0/5 motor strength of his bilateral lower extremities. Further, he had decreased sensation distally and areflexia in his bilateral lower extremities although he did not have any saddle anesthesia [13]. Imaging with MRI revealed engorgement of epidural venous plexus with subsequent crowding of the cauda equina. Further, MRI revealed severely enlarged bladder. Upon catheterization, he was able to have resolution of his epidural venous plexus engorgement on MRI and relief of compressive symptoms [13]. This case study demonstrated that even an enlarged bladder could cause significant mass effect resulting in a reversible venous plexus engorgement.
Mass effect is so important in engorgement of epidural venous plexuses that it may be of value to consider this diagnosis in the evaluation of radiculopathy in morbidly obese patients. One 15-year-old male presented with severe lumbar radiculopathy and MRI revealed plexus engorgement causing compression of the lumbar spinal canal [14]. Despite thorough workup there was no underlying etiology for the engorgement. He did not have any abdominal masses or tumors, no vascular abnormalities, and no blood clots. He has been followed for the next few years and continues to need pain management for his severe radiculopathy. He is also being encouraged and directed to follow body mass index (BMI) reduction through diet and movement [14].
Our patient presented similarly to previous case study examples with bilateral lower extremity paresthesia and minor saddle anesthesia. Given the patient’s history of similar symptoms with prior pregnancies and resolution of symptoms upon delivery, association between pregnancy and current presentation was highly likely. Magnetic resonance imaging was helpful in excluding other non-gravid causes and determining the cause of these symptoms to be due to venous plexus enlargement. Delivery usually results in resolution of symptoms. The patient was advised that future pregnancies would likely result in the same condition and symptoms. Little to no literature exists on the consequences of long term or recurrent venous plexus engorgement. In the case above, the 15-year-old male needed long-term pain management with lifestyle coaching [14],[15]. However, this patient is vastly different from our patient in age, gender, etiology, and management.
Conclusion
This patient has a unique recurrent presentation with earlier onset and increasingly more severe symptoms with each subsequent pregnancy. Our case highlights the need to have a high index of suspicion for epidural venous engorgement as an etiology for neurologic symptoms in a gravid individual.
REFERENCES
1.
Nathoo N, Caris EC, Wiener JA, Mendel E. History of the vertebral venous plexus and the significant contributions of Breschet and Batson. Neurosurgery 2011;69(5):1007–14. [CrossRef]
[Pubmed]

2.
Batson OV. The Function of the vertebral veins and their role in the spread of metastases. Ann Surg 1940;112(1):138–49. [CrossRef]
[Pubmed]
3.
Paksoy Y, Gormus N. Epidural venous plexus enlargements presenting with radiculopathy and back pain in patients with inferior vena cava obstruction or occlusion. Spine (Phila Pa 1976) 2004;29(21):2419–24. [CrossRef]
[Pubmed]
4.
Hirabayashi Y, Shimizu R, Fukuda H, Saitoh K, Igarashi T. Effects of the pregnant uterus on the extradural venous plexus in the supine and lateral positions, as determined by magnetic resonance imaging. Br J Anaesth 1997;78(3):317–9. [CrossRef]
[Pubmed]
5.
Hughes EJ, Price AN, McCabe L, et al. The effect of maternal position on venous return for pregnant women during MRI. NMR Biomed 2021;34(4):e4475. [CrossRef]
[Pubmed]
6.
Hirabayashi Y, Shimizu R, Fukuda H, Saitoh K, Igarashi T. Soft tissue anatomy within the vertebral canal in pregnant women. Br J Anaesth 1996;77(2):153–6. [CrossRef]
[Pubmed]
7.
Takiguchi T, Yamaguchi S, Tezuka M, Furukawa N, Kitajima T. Compression of the subarachnoid space by the engorged epidural venous plexus in pregnant women. Anesthesiology 2006;105(4):848–51. [CrossRef]
[Pubmed]
8.
Franco MJ, Vendrame M, Haneef Z, Azizi SA. Teaching NeuroImage: Acute spastic monoplegia secondary to spinal epidural venous engorgement in pregnancy. Neurology 2008;71(1):e1. [CrossRef]
[Pubmed]
9.
Wong TW, Gridley DG, Feiz-Erfan I. Epidural venous plexus engorgement due to inferior vena cava thrombosis resulting in cauda equina syndrome: Case report and literature review. Surg Neurol Int 2018;9:129. [CrossRef]
[Pubmed]
10.
Uhl E, Brückmann H, Goetz C. Congestion of epidural venous plexus secondary to vertebral artery occlusion mimicking a herniated cervical disc. Clin Neurol Neurosurg 2007;109(4):357–60. [CrossRef]
[Pubmed]
11.
Demaerel P, Petré C, Wilms G, Plets C. Sciatica caused by a dilated epidural vein: MR findings. Eur Radiol 1999;9(1):113–4. [CrossRef]
[Pubmed]
12.
Hassan O, Lewis CS, Aradhyula L, Hirshman BR, Pham MH. Engorged venous plexus mimicking adjacent segment disease: Case report and review of the literature. Surg Neurol Int 2020;11:104. [CrossRef]
[Pubmed]
13.
Tuan AS, Nabavizadeh SA, Pukenas B, Mohan S, Learned KO. Reversible dilatation of lumbar epidural venous plexus secondary to pelvic venous compression: Mimicker of pathology. BJR Case Rep 2016;3(1):20150287. [CrossRef]
[Pubmed]
14.
Jeong HJ, Sim WS, Park HJ, et al. Severe lumbar radiculopathy with epidural venous plexus engorgement in a morbidly obese pediatric patient: A case report. Medicine (Baltimore) 2019;98(33):e16842. [CrossRef]
[Pubmed]
15.
Donmez FY. Epidural venous plexus engorgement: What lies beneath? Case Rep Radiol 2015;2015:965106. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Brandon Sharkey - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Brooklyn McGue - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kaitlin Conner - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Chason Brodsky - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nabila Azeem - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Burton Brodsky - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Brandon Gabel - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Brandon Sharkey et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}