 |
Case Report
Management of severe acute respiratory distress syndrome in a pregnant patient due to COVID-19 with ECMO
1 MetroHealth Medical Center, 2500 MetroHealth Drive, Cleveland, OH 44109, USA
Address correspondence to:
Jonathan A Alter
Anesthesiology, 2500 MetroHealth Dr., Cleveland, OH 44019,
USA
Message to Corresponding Author
Article ID: 100168Z08MF2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Fuhrmann ME, Samoon Q, Fuhrmann KA, Platten M, Alter JA. Management of severe acute respiratory distress syndrome in a pregnant patient due to COVID-19 with ECMO. J Case Rep Images Obstet Gynecol 2024;10(1):6–10.ABSTRACT
SARS-CoV-2 has become a devastating upper respiratory tract infection that may progress to severe acute respiratory distress syndrome (ARDS) which may cause long-term disability or even death. The severity of this disease has warranted intubation with ventilatory support, extracorporeal membrane oxygenation (ECMO), and lung transplantation in certain patient populations. Extracorporeal membrane oxygenation has been demonstrated and used as a treatment for severe ARDS due to COVID in various patient populations, with limited guidance in multiparous patients. This case report may be used as a guide to use ECMO in pregnant patients as patients of all demographics, including pregnant patients, are affected by COVID-19. Herein, we describe the management of a multiparous patient at 25 weeks gestational age who developed severe ARDS after COVID-19 infection, was subsequently taken to the operating room for cesarean section, and placed on ECMO with initial improvement in ventilation, oxygenation, and hemodynamics prior to transfer to a facility with capabilities to maintain patients on ECMO.
Keywords: Acute respiratory distress syndrome, COVID-19, ECMO, Pregnancy
Introduction
The SARS-CoV-2 pandemic has affected over 219 million people worldwide with over 4.5 million deaths reported [1]. Patient populations at risk for severe complications include pregnant patients and the management of this population can be extremely complex. Patients who have progressed to severe acute respiratory distress syndrome (ARDS) have required invasive mechanical ventilation, paralytic use, and prone positioning [2]. These management efforts may become complicated in the pregnant patient, especially prone positioning as the gravid uterus as well as continuous fetal monitoring may prevent placing the patient completely in the prone position. The use of extracorporeal membrane oxygenation (ECMO) has been described as rescue therapy for severe ARDS due to COVID-19 infection when pregnant patients have not improved despite maximum mechanical ventilation efforts [3],[4]. We present the management of a multiparous patient at 25 weeks gestational age presenting to the operating room for cesarean section followed by ECMO cannulation after failing mechanical ventilation support due to severe ARDS after COVID-19 infection. With limited data on this patient population, this case may be used as a guide in the presentation and management of multiparous patients using ECMO to care for both the mother and baby in high-risk obstetric (OB) patients with various comorbidities [5],[6],[7]. A written Health Insurance Portability and Accountability Act (HIPAA) authorization form for publication was obtained from the patient’s mother. This article adheres to the applicable Enhancing the Quality and Transparency of Health Research (EQUATOR) guideline.
Case Report
A 22-year-old G5P3013 female at 25w1d gestational age with a past medical history significant for attention deficit hyperactivity disorder, obesity, bipolar II disorder, and passive cigarette smoke exposure presented to the emergency department in respiratory distress complaining of severe shortness of breath, sore throat, fatigue, and worsening fevers for more than a week.
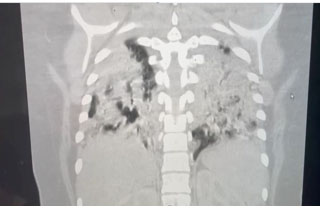
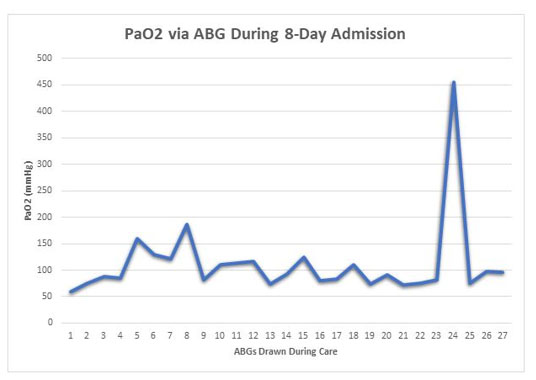
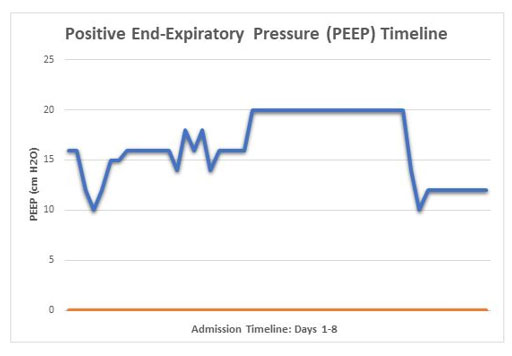
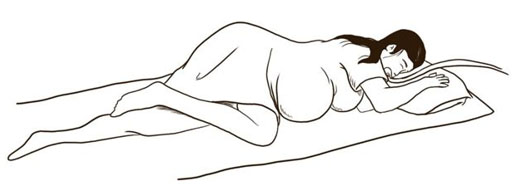
The patient was anxious, tachypneic with an SpO2 of 37%, febrile, and physical exam revealed bilateral rhonchi. She was placed on supplemental oxygen at 15 liters with minimal improvement of her oxygen saturation. Computed tomography (CT) scan of the chest showed diffuse ground glass opacities (Figure 1) and due to her worsening respiratory status, she was admitted to the intensive care unit for management and was intubated upon arrival to her room. She was started on high dose dexamethasone, remdesivir, and required norepinephrine for hemodynamic support. Continuous fetal monitoring and an increased steroid dose for lung maturity in case of early delivery were recommended by the Obstetrics team. With the patient’s PaO2 being of concern, she received many arterial blood gas analyses (ABGs) during her care, with a total of 27 ABGs analyzed (Figure 2). These results were consistent with COVID sepsis and acute hypoxic respiratory failure. The patient’s positive end-expiratory pressure (PEEP) (Figure 3) and oxygen requirements continued to rise with little improvement in clinical status, so the decision was made to start her on a paralytic infusion as well as place her in a semi-prone position (Figure 4) to allow for continuous fetal monitoring and uterine displacement. Initially, oxygenation improved with the semi-prone position. However, on hospital day 7, significant subcutaneous emphysema was noted as well as the continuous need for a PEEP value of 20 cmH2O and 100% FiO2 to maintain appropriate oxygenation.
Due to her worsening condition and increasing ventilation settings with minimal clinical improvement, a multidisciplinary decision to place the patient on ECMO was made. Careful coordination between intensive care unit (ICU), Obstetrics, Neonatal intensive care unit (NICU), Cardiothoracic, Respiratory Therapy, and Anesthesia teams was necessary to allow for safe transport to the operating room, rapid delivery of the baby, and placement of the patient on ECMO. Prior to the start of the cesarean section, both the right internal jugular and right femoral veins were accessed, and wires were left in place to allow for eventual ECMO cannulation. During the cesarean section, the patient’s hemodynamic status rapidly declined and both vasopressin and norepinephrine infusions were required to maintain adequate perfusion. The baby was delivered quickly via cesarean section, intravenous heparin was dosed after the obstetric team achieved adequate hemostasis, cannulation for ECMO was performed, and the patient was placed on veno-venous ECMO. Oxygen saturations quickly improved, and the patient was transferred to a facility with the capability of maintenance on ECMO. After delivery, the baby was intubated and moved to the NICU for further resuscitation and closer monitoring. The patient was maintained on ECMO for two weeks, initially with improvement in her hemodynamics and mental status; however, she suffered a rapid decline, and her family made the decision to withdraw care. After a three-month course in the NICU, the baby was discharged home to family, however, suffered from complications of prematurity including retinopathy of prematurity requiring laser therapy and poor feeding requiring gastric tube placement.
Discussion
The SARS-CoV-2 virus was identified as a global pandemic in March 2020 and has been responsible for severe acute respiratory distress syndrome that has, in some cases, led to multiorgan failure and death. Pregnant women have been among those affected, with the Centers for Disease Control (CDC) reporting over 120,000 pregnant women with COVID-19 and over 21,000 reported cases requiring hospitalization for progression of disease [1],[4],[7]. Although pregnancy alone has not been shown to increase the risk for severe disease, physiologic changes that occur during pregnancy in conjunction with the presence of certain comorbidities including asthma, smoking, and obesity could increase the risk of progression to severe disease requiring hospitalization and potential ventilatory support.
The management and treatment plan of care for a multiparous parturient patient is intricate as the physiology of the mother and baby is intrinsically different [8]. Therefore, during this case, the baby was under continuous, around-the-clock fetal monitoring as directed by the Obstetrics team. This altered the plan of care for this patient dramatically, as each specialty team was utilizing the fetal monitoring as a guide in managing the health of both the mother and the baby. Ultimately, the changes observed within the fetal monitoring were the deciding factor in many of the decisions that were made when caring for this patient, especially on when to intervene and perform the cesarean section and place the patient on ECMO. These fetal changes were the answer to the rigorous question of when the baby was safe enough to maturely deliver and what the best mediation to save the mother was. This concordance in care allowed for the thought process during these challenging clinical decisions to incorporate the best possible outcomes for both the mother and baby, as we were caring for both patients [4],[9].
When appropriate, ECMO should be considered for pregnant patients with severe disease caused by COVID-19 [5],[6],[10]. Discussion of the timing of the start of ECMO support, delivery, as well as maternal risks and benefits must be considered for both maternal and neonatal benefit. In this case, ECMO was the only option for both the mother and baby. Extracorporeal membrane oxygenation was the safest way to ensure that the baby would be able to survive as the disease had caused an advanced decline in the mother. Therefore, this case can be used as a guide to expand the use of ECMO into other specialties, such as obstetrics, to care for patients in down-trending hypoxemic conditions.
A multidisciplinary approach is vital to the success of critical care in a parturient. The integration of all specialties caring for the patient is essential as communication between the teams will allow for the best plan of care. During our care for this patient, there were routine daily briefings between the various different specialties, with each specialty combining their strategies to effectuate the best plan of care the patient could receive. This was extremely advantageous as each specialty brought their own ideas and plan of care to the meetings and adjusted their plans after thorough discussion before agreeing to a holistic approach. These routine daily meetings were extremely significant in coordinating the safe and timely delivery of the baby and the placement of the mother on ECMO to allow for a chance at recovery. Therefore, this report also emphasizes the necessity of various specialties and subspecialties in medicine working collectively to bring about the ultimate plan of care for each patient.
Conclusion
Extracorporeal membrane oxygenation can be considered as a care option for parturient patients suffering from ARDS. The pregnancy was viable at 25 weeks gestation, the patient was unable to maintain appropriate oxygenation with endotracheal intubation and mechanical ventilation, and there was a possibility of disease recovery. Thus, ECMO may provide the best chance of recovery for both the mother and the baby. The management of the patient should be intricately coordinated between the various teams involved in the care of the patient. Through the multidisciplinary approach, all teams will be informed on the status of the patient, able to revise the plan of care as needed to maximize the chance of recovery for both the mother and baby.
REFERENCES
1.
CDC COVID Data tracker. Centers for Disease Control and Prevention. [Available at: https://covid.cdc.gov/covid-data-tracker/#datatracker-home]

2.
COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. [Available at: https://www.covid19treatmentguidelines.nih.gov]
3.
Barrantes JH, Ortoleva J, O'Neil ER, et al. Successful treatment of pregnant and postpartum women with severe COVID-19 associated acute respiratory distress syndrome with extracorporeal membrane oxygenation. ASAIO J 2021;67(2):132–6. [CrossRef]
[Pubmed]
4.
Li Y, Xu C, Li F, et al. Five critically ill pregnant women/parturients treated with extracorporeal membrane oxygenation. J Cardiothorac Surg 2022;17(1):321. [CrossRef]
[Pubmed]
5.
Jacobs JP, Stammers AH, St Louis J, et al. Extracorporeal membrane oxygenation in the treatment of severe pulmonary and cardiac compromise in coronavirus disease 2019: Experience with 32 patients. ASAIO J 2020;66(7):722–30. [CrossRef]
[Pubmed]
6.
The Extracorporeal Life Support Organization (ELSO): ECMO in COVID-19. [Available at: https://elso.org]
7.
Lankford AS, Chow JH, Jackson AM, et al. Clinical outcomes of pregnant and postpartum extracorporeal membrane oxygenation patients. Anesth Analg 2021;132(3):777–87. [CrossRef]
[Pubmed]
8.
Diago-Muñoz D, Martínez-Varea A, Pérez-Sancho E, Diago-Almela V. Severe COVID-19 infection during pregnancy requiring ECMO: Case report and review of the literature. J Pers Med 2023;13(2):263. [CrossRef]
[Pubmed]
9.
Federici L, Picone O, Dreyfuss D, Sibiude J. Successful continuation of pregnancy in a patient with COVID-19-related ARDS. BMJ Case Rep 2020;13(8):e237511. [CrossRef]
[Pubmed]
10.
Webster CM, Smith KA, Manuck TA. Extracorporeal membrane oxygenation in pregnant and postpartum women: A ten-year case series. Am J Obstet Gynecol MFM 2020;2(2):100108. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
The authors are grateful to Luis Tollinche, MD, FASA, Department Chair of Anesthesiology, Case Western School of Medicine at MetroHealth Medical Center, Cleveland, OH for his support, critical review of the case report, and significant editorial assistance. The authors also thank Jessie Ciccarelli for providing a wonderful drawing for our case report.
Author ContributionsMeaghan E Fuhrmann - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Quratulain Samoon - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kurt A Fuhrmann - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Michael Platten - Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jonathan A Alter - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Meaghan E Fuhrmann et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}