 |
Case Report
Unique presentation of previable HELLP syndrome
1 Department of Obstetrics and Gynecology, Summa Health, Akron, Ohio, USA
2 Department of Obstetrics and Gynecology, Northeast Ohio Medical University, Rootstown, Ohio, USA
Address correspondence to:
Kylan Hill
DO, Department of Obstetrics and Gynecology, Summa Health, 141 N Forge St, Akron, OH 44304,
USA
Message to Corresponding Author
Article ID: 100171Z08KH2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Hill K, Jackson R, Tran P. Unique presentation of previable HELLP syndrome. J Case Rep Images Obstet Gynecol 2024;10(1):29–33.ABSTRACT
Introduction: Hemolysis, elevated liver enzymes, low platelets (HELLP) syndrome is a serious complication of pregnancy characterized by hemolysis, elevated liver enzymes, and low platelets. This condition typically affects pregnant women in the third trimester or postpartum states, with only a handful of reported cases in previable pregnancies. The symptoms of HELLP syndrome can mimic those of other critical conditions during pregnancy, such as acute fatty liver of pregnancy (AFLP), thrombotic thrombocytopenic purpura (TTP), hemolytic-uremic syndrome (HUS), systemic lupus erythematosus (SLE), and antiphospholipid syndrome (APS), making early diagnosis crucial to prevent maternal and fetal harm.
Case Report: We report the case of a 23-year-old nulliparous woman who developed HELLP syndrome at 21 weeks gestation. We highlight the importance of recognizing early onset HELLP syndrome and differentiating it from other potential diagnoses to ensure prompt and appropriate treatment.
Conclusion: This case of previable HELLP syndrome in a nulliparous patient without other risk factors highlights the importance of early detection and intervention as life saving measures. By understanding the clinical and laboratory findings specific to HELLP syndrome, healthcare providers can improve maternal and fetal outcomes in cases of this rare and serious complication of pregnancy.
Keywords: Elevated lactate dehydrogenase, HELLP syndrome, Pregnancy
Introduction
Hemolysis, elevated liver enzymes, low platelets (HELLP) syndrome, a serious pregnancy complication with hemolysis, liver enzyme elevation, and low platelets, affects expectant and postpartum individuals. Most common between 27 0/7 and 37 0/7 weeks of gestation, roughly 10% of cases occur before the 27th gestational week [1]. Rare but reported previable cases have been associated with hydatidiform mole or antiphospholipid-antibody syndrome [2],[3],[4],[5],[6]. Symptoms encompass hypertension, abdominal pain, nausea, vomiting, and flu-like indications. Labs reveal schistocytes, liver function shifts, elevated lactate dehydrogenase, decreased platelets, raised bilirubin, and proteinuria. Hemolysis, elevated liver enzymes, low platelets (HELLP) leads to maternal complications like disseminated intravascular coagulation (DIC), placental abruption, and kidney issues [6]. Prompt differentiation from other pregnancy complications such as acute fatty liver of pregnancy (AFLP), thrombotic thrombocytopenic purpura (TTP), hemolytic-uremic syndrome (HUS), systemic lupus erythematosus (SLE), and antiphospholipid syndrome (APS) is vital for maternal and fetal safety. This case reports previable HELLP at 21 weeks in a nulliparous patient lacking risk factors. Collaborative efforts of maternal-fetal medicine, hematology, and critical care led to diagnosis. Due to severe maternal risk, termination was advised. Early recognition and intervention are crucial for maternal well-being, highlighting subsequent pregnancy complication counseling.
Case Report
A 23-year-old woman (G2P0010) presented to the obstetrics (OB) triage unit at 20 weeks and 3 days of gestation with left-sided abdominal pain and decreased fetal movement. Her prenatal care had been satisfactory, and she had no significant medical or surgical history. A fetal anatomy ultrasound at 19 weeks and 4 days revealed findings suggestive of fetal growth restriction, with the head circumference measuring at the 3rd percentile, abdominal circumference in the 4th percentile, and femur length in the 7th percentile. However, the rest of the fetal anatomy appeared normal. Upon admission to OB triage, her vital signs were stable and blood pressure was normotensive. Clinical exam findings were positive for epigastric tenderness and preterm labor was ruled out. Her abdominal pain resolved with the administration of acetaminophen and famotidine. A bedside ultrasound and basic laboratory tests were within normal limits, and she was discharged with instructions for return precautions.
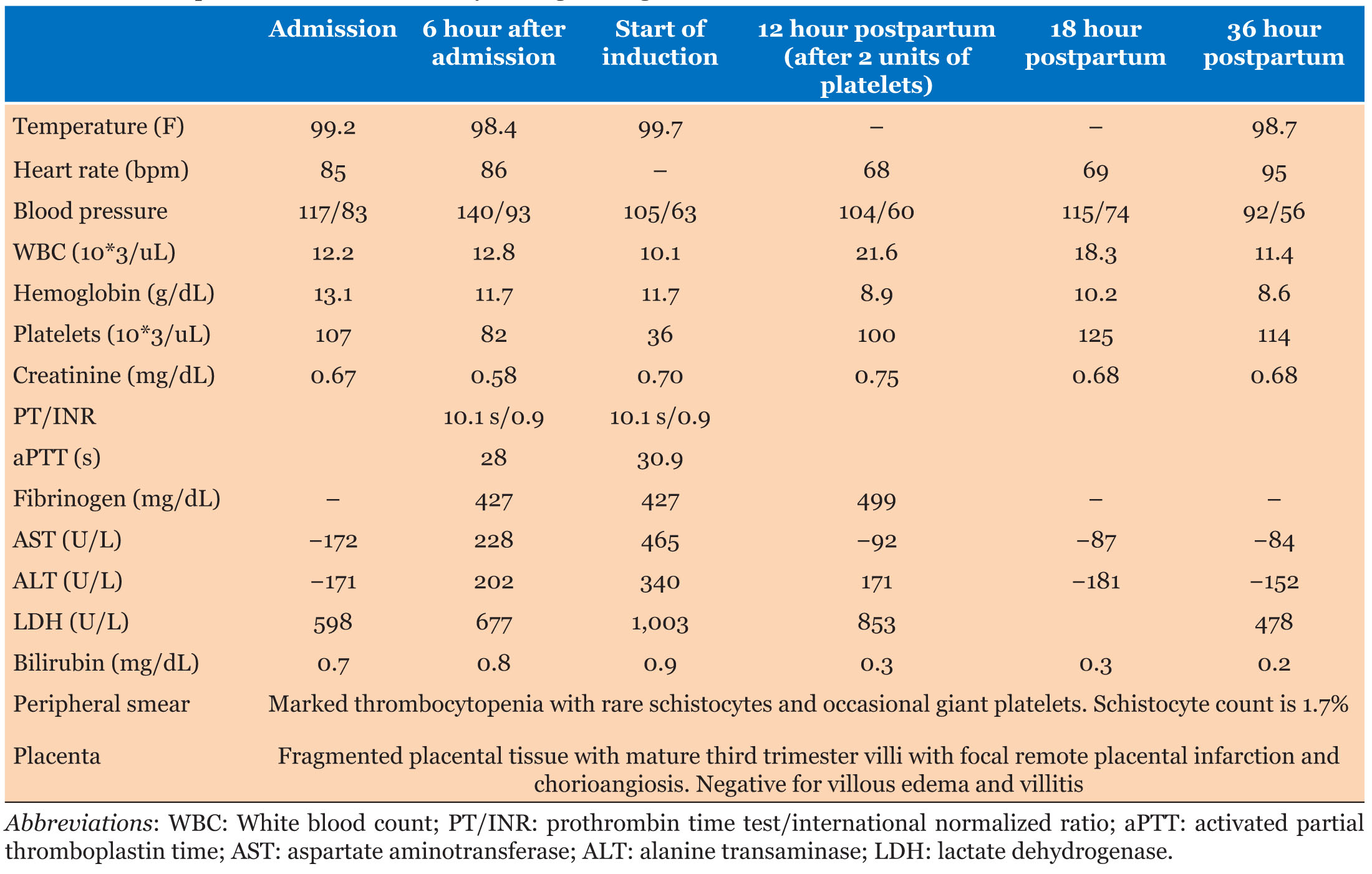
Two days later, at 20 weeks and 5 days, the patient returned to OB triage with intense pain in the right upper quadrant (RUQ) of the abdomen. Her vital signs remained stable, blood pressure was normotensive, and her abdominal examination was unremarkable. She was discharged again after evaluation. However, at 21 weeks and 0 days, she returned to OB triage with worsening epigastric pain that did not respond to previous interventions and inability to tolerate oral intake. Laboratory tests were ordered, and she was admitted for observation. Her vital signs and laboratory results, which are shown in Table 1, revealed thrombocytopenia, liver function tests (LFTs) twice the upper limit of normal, and lactate dehydrogenase (LDH) approaching 600 U/L. An abdominal ultrasound showed normal liver, gallbladder, pancreas, and bilateral kidneys. Labs were repeated 6 hours later and showed an acute worsening of LDH (>600) and platelets (<100). Due to the concern for HELLP syndrome and worsening maternal condition, magnesium sulfate was initiated for seizure prophylaxis. The maternal fetal medicine team was consulted, and medical termination of pregnancy was recommended.
Expulsion of the fetus occurred at 21 weeks and 1 day. She required dilation and curettage for retained placenta. At this time, her platelets were noted to be 36 10*3/uL, and she received two units of platelets before being taken to the operating room. After delivery, laboratory tests showed a dramatic improvement, as shown in Table 1, and were trended at 12 hours, 18 hours, and 36 hours postpartum. Her symptoms also improved, and she was ultimately discharged on postpartum day two. She was closely followed in the outpatient setting, where she remained stable, without any complaints.
Discussion
Hemolysis, elevated liver enzymes, low platelets syndrome is a rare but life-threatening condition characterized by hemolysis, elevated liver enzymes, and low platelet count. It is crucial to diagnose and treat this condition in a timely manner to prevent maternal morbidity and mortality. However, there are several pregnancy-related problems that can present with similar signs and symptoms, including acute fatty liver of pregnancy (AFLP), thrombotic thrombocytopenic purpura (TTP), hemolytic-uremic syndrome (HUS), exacerbation of systemic lupus erythematosus (SLE), and antiphospholipid syndrome (APS). Each of these conditions is associated with high rates of maternal morbidity and mortality, and they can present with various signs and symptoms, such as hypertension, proteinuria, fever, jaundice, nausea and vomiting, abdominal pain, and central nervous system involvement. To make an accurate diagnosis, it is crucial to discern each condition and its unique clinical features. For example, AFLP is characterized by fatty infiltration of the liver and is often associated with nausea and vomiting, while TTP is characterized by microangiopathic hemolytic anemia and thrombocytopenia and can present with neurologic symptoms. Distinguishing between these pregnancy-related problems is crucial in determining an appropriate course of treatment in a timely manner. Healthcare providers should be aware of the clinical features of each condition and should consider them in the differential diagnosis when a pregnant patient presents with signs and symptoms consistent with HELLP syndrome.
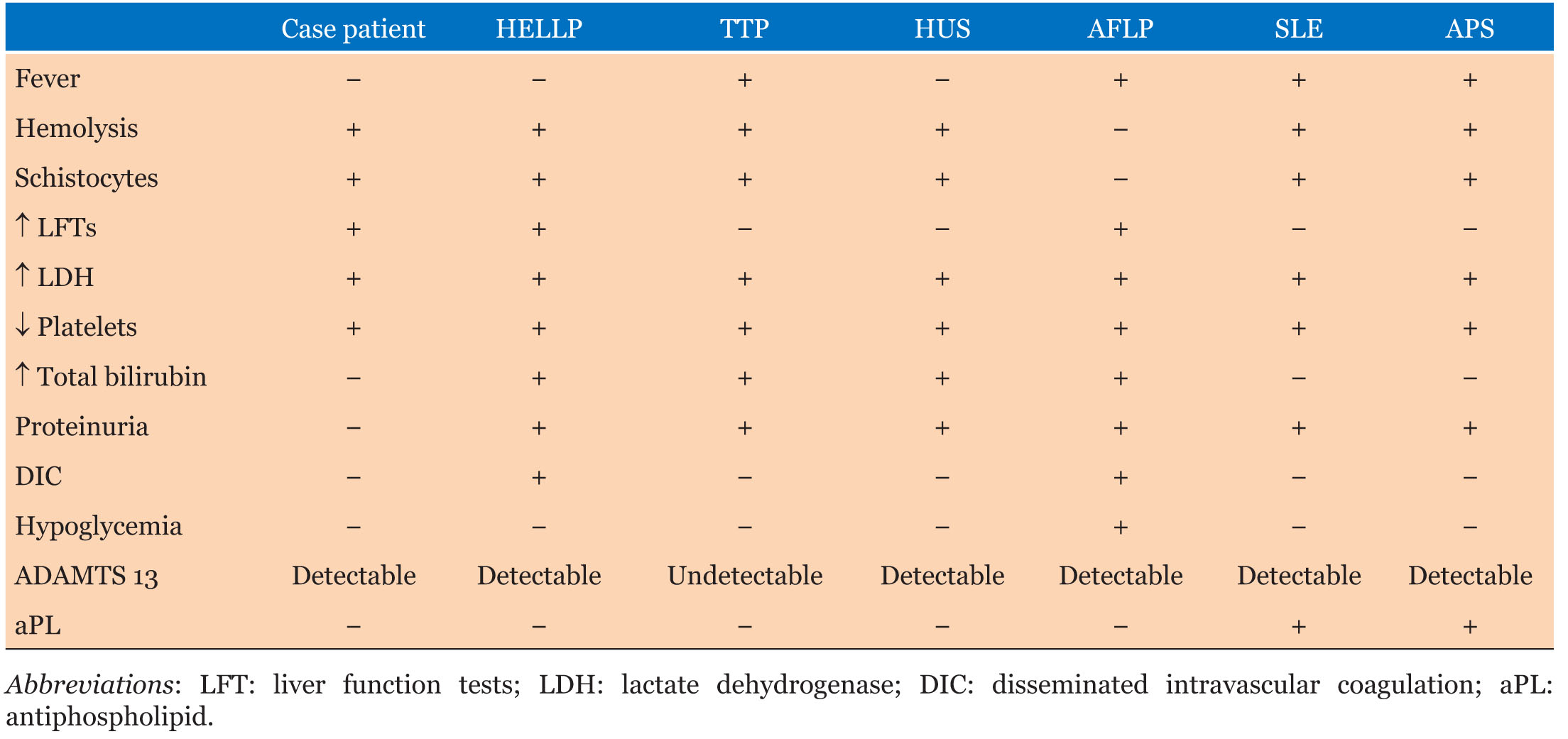
The patient’s presentation included hemolysis and thrombocytopenia, which are also observed in microangiopathic hemolytic anemias such as thrombotic thrombocytopenic purpura (TTP), and hemolytic-uremic syndrome (HUS). In TTP and HUS, red blood cells are sheared along the damaged endothelium, which consumes platelets that adhere to the endothelial membrane, leading to thrombocytopenia. This results in the presence of schistocytes and elevated serum lactate dehydrogenase (LDH) levels due to hemolysis. In addition, platelet microthrombi may form, break off, and travel through the bloodstream, causing proteinuria by depositing into the kidney [7]. However, our patient did not exhibit proteinuria, and their total bilirubin levels were normal (Table 2), despite having increased LDH and schistocytes. Furthermore, TTP was ruled out as our patient had detectable ADAMTS13 levels. Hemolytic-uremic syndrome typically occurs post-gastroenteritis and is caused by Shiga toxin-induced endothelial damage, which is unlikely in our patient’s case based on her presenting history.
Acute fatty liver of pregnancy (AFLP) shares some similarities with HELLP syndrome in terms of laboratory findings, such as elevated liver function tests, bilirubin, impaired renal function, possible disseminated intravascular coagulation (DIC), hemolysis, and thrombocytopenia. However, there are specific features that differentiate AFLP from HELLP syndrome. Hypoglycemia and a fibrinogen level below 300 mg/dL are characteristic findings of AFLP, which were not present in our patient (Table 2). On the other hand, hemolytic anemia and schistocytes are typically seen in HELLP syndrome but not in AFLP. It is important to distinguish between these two disorders because women with AFLP are at high risk of developing rapid liver failure, encephalopathy, and severe hypoglycemia. Since our patient did not have these specific features, AFLP was ruled out as a possible diagnosis.
Systemic lupus erythematosus (SLE) is characterized by immune complex deposits in blood vessels and the kidney, which can result in a clinical picture consistent with microangiopathic hemolytic diseases. However, SLE is commonly associated with increased levels of antiphospholipid antibodies, including lupus anticoagulant and anticardiolipin antibodies, which our patient tested negative for. Therefore, SLE was an unlikely diagnosis in this patient due to the absence of these antibodies. Antiphospholipid syndrome (APS) can occur as a primary condition or with underlying SLE and presents with clinical features similar to those of SLE, including hypertension, proteinuria, and thrombocytopenia. However, the presence of antiphospholipid antibodies (aPL) is the key diagnostic feature of APS [8], which our patient did not have. As a result, APS was also ruled out in this patient.
After considering various possible diagnoses with similar clinical symptoms and laboratory markers, it was concluded that this patient was most likely suffering from HELLP syndrome. Although cases of HELLP syndrome detected before 24 weeks are rare, they are more likely to result in severe morbidity [2]. A retrospective cohort study of 26 pregnancies with early-onset preeclampsia [9]. While premature onset of HELLP syndrome is typically associated with other comorbidities such as fetal triploidy, partial hydatidiform mole, or preeclampsia [3],[8],[10], the patient’s placenta pathology results were negative for these conditions, and genetic testing for fetal triploidy was also negative. She also did not have any obvious risk factors for preeclampsia such as hypertension or proteinuria early in her presentation, although she did have several elevated blood pressure readings later in her course. This case is unique in that it presented early without evidence of other conditions or typical risk factors.
Conclusion
In conclusion, this case report describes a rare presentation of HELLP syndrome at 21 weeks gestation without any evidence of other conditions or typical risk factors. The differential diagnosis was extensive and included other conditions with similar clinical and laboratory features. After ruling out multiple differentials, HELLP syndrome was diagnosed, and termination was recommended due to the risk of severe maternal morbidity. Early detection and intervention are crucial for improving maternal outcomes, and patients should be counseled on the risk of obstetric complications in subsequent pregnancies. This case highlights the need for obstetricians to consider HELLP syndrome as a potential diagnosis in patients presenting with new onset transaminitis, severe thrombocytopenia, and epigastric pain, even in the absence of typical risk factors or at an earlier gestational age.
REFERENCES
1.
Magann EF, Martin JN Jr. Twelve steps to optimal management of HELLP syndrome. Clin Obstet Gynecol 1999;42(3):532–50. [CrossRef]
[Pubmed]

2.
Bornstein E, Barnhard Y, Atkin R, Divon MY. HELLP syndrome: A rare, early presentation at 17 weeks of gestation. Obstet Gynecol 2007;110(2 Pt 2):525–7. [CrossRef]
[Pubmed]
3.
Sherer DM, Dalloul M, Stimphil R, et al. Acute onset of severe hemolysis, elevated liver enzymes, and low platelet count syndrome in a patient with a partial hydatidiform mole at 17 weeks gestation. Am J Perinatol 2006;23(3):163–6. [CrossRef]
[Pubmed]
4.
Stefos T, Plachouras N, Mari G, Cosmi E, Lolis D. A case of partial mole and atypical type I triploidy associated with severe HELLP syndrome at 18 weeks’ gestation. Ultrasound Obstet Gynecol 2002;20(4):403–4. [CrossRef]
[Pubmed]
5.
Haram K, Trovik J, Sandset PM, Hordnes K. Severe syndrome of hemolysis, elevated liver enzymes and low platelets (HELLP) in the 18th week of pregnancy associated with the antiphospholipid-antibody syndrome. Acta Obstet Gynecol Scand 2003;82(7):679–80. [CrossRef]
[Pubmed]
6.
Myer E, Hill J. First trimester hemolysis, Elevated liver enzymes, low platelets syndrome in a surrogate pregnancy. AJP Rep 2015;5(2):e212–4. [CrossRef]
[Pubmed]
7.
Berry EL, Iqbal SN. HELLP syndrome at 17 weeks gestation: A rare and catastrophic phenomenon. J Clin Gynecol Obstet 2014;3(4):147–50.
[Pubmed]
8.
August P, Helseth G, Cook EF, Sison C. A prediction model for superimposed preeclampsia in women with chronic hypertension during pregnancy. Am J Obstet Gynecol 2004;191(5):1666–72. [CrossRef]
[Pubmed]
9.
Gaugler-Senden IPM, Huijssoon AG, Visser W, Steegers EAP, de Groot CJM. Maternal and perinatal outcome of preeclampsia with an onset before 24 weeks’ gestation. Audit in a tertiary referral center. Eur J Obstet Gynecol Reprod Biol 2006;128(1– 2):216–21. [CrossRef]
[Pubmed]
10.
Karumanchi SA, Maynard SE, Stillman IE, Epstein FH, Sukhatme VP. Preeclampsia: A renal perspective. Kidney Int 2005;67(6):2101–13. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Kylan Hill - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Renae Jackson - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Phuong Tran - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Kylan Hill et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}