 |
Case Report
Peritoneal bile granuloma formation at the site of caesarean surgical scar
1 Department of Obstetrics and Gynecology, University of Rochester Medical Center, Rochester, NY, USA
2 Department of Pathology, University of Rochester Medical Center, Rochester, NY, USA
3 Trillium Health, Rochester, NY, USA
Address correspondence to:
Lila Marshall
MD, University of Rochester Medical Center, 601 Elmwood Ave, Box #668, Rochester, NY 14642,
USA
Message to Corresponding Author
Article ID: 100176Z08LM2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Marshall L, Varghese S, Ciranni-Callon M. Peritoneal bile granuloma formation at the site of caesarean surgical scar. J Case Rep Images Obstet Gynecol 2024;10(2):6–10.ABSTRACT
Bile granuloma is a rare complication associated with cholecystectomy about which few case reports have been written. Herein we present the case of a patient who underwent laparoscopic bilateral salpingectomy for the purpose of sterilization and was incidentally found to have a linear collection of bile granulomas along the site of adhesions from her cesarean section. We also present a review of case reports on bile granuloma that have presented in OB/GYN and suggest that this rare pathology should be cited as a differential more often when considering intra-abdominal pathology, particularly for pelvic surgeons. We argue that this condition is likely more common than previously thought and suggest that without further research into this topic, routine biopsy or removal of encountered lesions may not always be necessary in patients at low likelihood for having a malignant pathology.
Keywords: Bile granuloma, Cesarean scar, Endometriosis
Introduction
The formation of peritoneal bile granulomas is a rare complication after cholecystectomy thought to stem from bile or gallstone spillage at the time of surgery [1]. To our knowledge, fewer than ten case reports have been published on this topic. While most bile granulomas seem to encompass crystalized bile and represent an immune granulomatous reaction to this material, others have been reported to encapsulate whole gallstones. Bile or gallstone spillage is reported in 10–40% of cholecystectomies, and is thought to occur with greater frequency in the laparoscopic approach [1],[2],[3]. They are generally considered to be benign, but some suggest that bile granulomas may be associated with pelvic pain and even infertility [4],[5],[6]. They can also mimic the appearance of peritoneal seeding in the setting of malignancy, often resulting in surgical intervention for affected patients [7],[8],[9]. The incidence of bile granuloma is unknown, but we suggest that this finding is likely more common than previously thought given the prevalence of gallbladder surgery in the general population and the relatively high rate of bile or stone spillage in this surgery.
Herein we present the case of a patient in her 30s who presented for laparoscopic tubal sterilization and was found to have a linear collection of lesions along adhesions from her cesarean section which were found to be consistent with bile granulomas. We hope to contribute to the limited body of literature available on this topic and increase awareness of this possible complication after cholecystectomy and its variable presentations, particularly in pelvic surgery. And with limited clinical information on bile granuloma, we argue that biopsy and removal of these lesions may not always be indicated and might instead pose undue risk for patients.
Case Report
Initial presentation
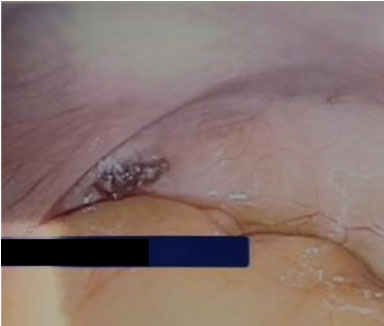
A patient in her 30s presented to the hospital for scheduled laparoscopic bilateral salpingectomy for permanent tubal sterilization. Her medical history was notable for obesity, hypertension, polycystic ovarian syndrome, cholelithiasis, and gastroesophageal reflux disease. Her surgical history included laparoscopic sleeve gastrectomy, laparoscopic cholecystectomy, and one cesarean section. She was otherwise medically uncomplicated and had no reported history of chronic pelvic pain. Survey of the abdomen and pelvis at the time of surgery revealed normal-appearing bowel, liver, uterus, fallopian tubes, and ovaries. The uterus was adhered to the anterior abdominal wall along a horizontal, linear area of scar tissue consistent with the site of the patient’s cesarean section. A linear collection of dark brown-red lesions was appreciated along this scar tissue (Figure 1). Another collection of similar-appearing lesions was noted in the posterior cul-de-sac, just posterior to the left utero-sacral ligament in an area otherwise devoid of scar tissue (Figure 2). No other lesions were appreciated on detailed survey of the abdomen and pelvis and no other adhesive disease was noted. Due to the location of accumulation of the lesions, these were thought to possibly be consistent with endometriosis. A biopsy of the lesions along the anterior abdominal wall adhesions was collected using atraumatic laparoscopic graspers. On gross examination, the lesions were hard in consistency and the contents appeared crystalline, with an amber hue. Both fallopian tubes were removed laparoscopically without complication. The patient’s post-operative course was unremarkable and she was discharged home in stable condition on the same day of surgery.
Pathology and disposition
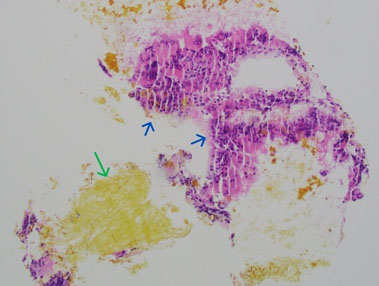
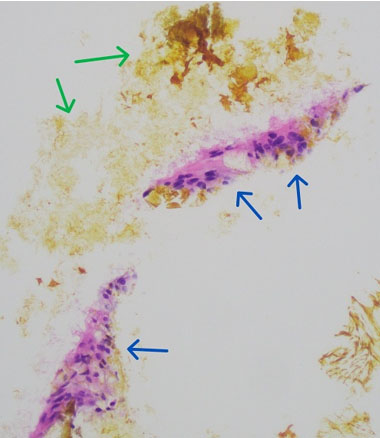
Gross examination of the biopsied anterior abdominal wall lesion described a 0.7 × 0.5 × 0.2 cm aggregate of brown-red material. Histologic evaluation revealed yellow pigmented bile-like material, histiocytes (Figure 3), and giant cells (Figure 4). The favored diagnosis was bile granuloma. Pathology review of the fallopian tubes revealed normal histology for both tubes.
Given that the patient was asymptomatic, a plan was made to proceed with routine post-operative care of the patient with no further intervention or monitoring planned. At the time of publication of this report, over one year after surgery, the patient continues to be in good health.

Discussion
Herein we have presented the case of a patient in her 30s who underwent laparoscopic bilateral salpingectomy for tubal sterilization and was ultimately found on pathology review to have evidence of bile granuloma formation along adhesions from her cesarean section. While the small number of case reports on the phenomenon precludes the ability to ascertain a clear pathogenesis, it seems reasonable to suggest that bile granulomas likely form as a result of a localized inflammatory response due to the presence of bile or gallstones in the peritoneal space. The particular accumulation of bile granulomas along a horizontal region of cesarean scar adhesions in the presented patient supports this idea: we propose that in the area of active tissue healing and immune activity of the site of cesarean surgery, bile may have been encountered by immune cells and granulomas subsequently formed. In the presented case, lesions were also noted in the posterior cul-de-sac. While the patient denied a history of pelvic inflammatory disease or chronic pelvic pain, an immune response to subclinical pathology in the pelvis could conceivably have incorporated bile and resulted in the formation of bile granulomas in that space. With the scant number of available reports, not enough information about bile granuloma is available to provide clear explanation for their development. Without further study into this topic, we can only provide conjecture to explain their formation. However, we propose that the immune response, including post-surgical healing, may provide an avenue for insight.
There are several considerations of bile granuloma that are particular to obstetric and gynecologic surgeons. Several case reports have suggested a possible association of bile granulomas with chronic pelvic pain and have noted that they can mimic endometriosis lesions, as they did in the presented case [4],[5]. In patients undergoing surgical evaluation of pelvic pain or resection of endometriosis, gynecologic surgeons should be aware of the visual similarities of bile granuloma and endometriosis. Further research is needed into the optimal visual differentiation of these separate lesions, so as to spare patients possibly unnecessary surgical intervention in removing benign granulomatous lesions supposed to be consistent with endometriosis. There is also insufficient clinical information to characterize the association of bile granuloma with pelvic pain, but study into this topic could lead to advancements in the differential diagnosis and management of chronic pelvic pain. Another phenomenon pertinent to OB/GYN surgeons is the potential for bile granulomas to form in the omentum. Two case reports have documented the diagnosis of bile granuloma after biopsy of hardened nodules discovered in the omentum during cesarean section [2],[7]. In these reports, the discovery of nodules in the omentum raised concern for malignancy, and biopsies ultimately confirmed otherwise. Both patients were noted to have had cholecystectomies in the past. Awareness of this possible presentation of bile granuloma is important as patients at low risk for malignancy may not require omental biopsy, which could expose patients to undue risk. And finally, the rare phenomenon of ovarian cholelithiasis has been presented in at least three case reports [6],[10],[11]. In two of the presented patients, adnexal masses and peritoneal nodularity raised concern for malignancy and surgery was ultimately performed. The reports note tissue deposits on the ovary and surrounding organs and peritoneum, with biopsies ultimately noting presence of bile and gallstones. One of these patients experienced intra-abdominal hemorrhage that was found to stem from the area of gallstone implantation in the pelvis [11]. In another patient, surgery was performed to explore possible structural causes of infertility and tissue deposits were noted on the ovaries, ultimately found to contain bile and gallstones [6]. These reports demonstrate how complications of cholecystectomy can present in ways that mimic gynecologic conditions; OB/GYNs should be aware of these variable presentations of bile granuloma, albeit rare.
We argue that with a high prevalence of cholecystectomy in the American population and an estimated 300,000 cases performed per year [12] , the prevalence of bile granuloma may be higher than previously thought. Further, the incidence is likely to increase with the increasing likelihood of patients undergoing laparoscopic or robot-assisted cholecystectomy. If peritoneal lesions or other suspicious findings are encountered on abdominopelvic survey during surgery, surgeons should be aware of the phenomenon of bile granuloma and include this in their differential, particularly in patients with history of laparoscopic cholecystectomy. Given that there is insufficient clinical information to suggest that bile granulomas are hazardous to patient health and should be removed, we suggest that confirmatory biopsy or complete excision of lesions may not always be necessary. In an asymptomatic patient with low risk for malignancy or other pathology that could otherwise lead to formation of peritoneal lesions, biopsy may not provide clinically useful information and, depending on the site of the lesions, removal could be surgically complicated and pose undue risk to the patient. The psychological and emotional strain of a potentially confusing diagnosis could also pose an undue burden on patients. Further research is indicated into the complications of bile granulomas and their long-term significance for patient health.
Conclusion
Bile granuloma formation is a possible complication of cholecystectomy and can present in a variety of ways pertinent to obstetricians and gynecologists. This phenomenon is thought to be intrinsically benign, but further research is needed to elucidate their long-term significance.
REFERENCES
1.
Jeong H, Lee HW, Jung HR, et al. Bile granuloma mimicking peritoneal seeding: A case report. J Pathol Transl Med 2018;52(5):339–43. [CrossRef]
[Pubmed]

2.
McVeigh G, McComiskey M, McCluggage WG. Peritoneal bile granulomas identified at cesarean section and mimicking disseminated malignancy. Int J Surg Pathol 2012;20(1):89–91. [CrossRef]
[Pubmed]
3.
Woodfield JC, Rodgers M, Windsor JA. Peritoneal gallstones following laparoscopic cholecystectomy: Incidence, complications, and management. Surg Endosc 2004;18(8):1200–7. [CrossRef]
[Pubmed]
4.
Lamvu-Schooler G, Steege JF. Postlaparoscopic cholecystectomy pelvic gallstones associated with chronic pain. J Am Assoc Gynecol Laparosc 2000;7(2):273–5. [CrossRef]
[Pubmed]
5.
Merchant SH, Haghir S, Gordon GB. Granulomatous peritonitis after laparoscopic cholecystectomy mimicking pelvic endometriosis. Obstet Gynecol 2000;96(5 Pt 2):830–1. [CrossRef]
[Pubmed]
6.
Vadlamudi G, Graebe R, Khoo M, Schinella R. Gallstones implanting in the ovary. A complication of laparoscopic cholecystectomy. Arch Pathol Lab Med 1997;121(2):155–8.
[Pubmed]
7.
Suarez-Zamora DA, Barrera-Herrera LE, Caceres-Mileo R, et al. Intraperitoneal granulomas unexpectedly found during a cesarean delivery: A late complication of dropped gallstones. Case Rep Pathol 2017;2017:4873273. [CrossRef]
[Pubmed]
8.
Famularo G, Remotti D, Galluzzo M, Gasbarrone L. Granulomatous peritonitis after laparoscopic cholecystectomy. JSLS 2012;16(3):481–4. [CrossRef]
[Pubmed]
9.
Warren CW, Wyatt JI. Gallstones split at laparoscopic cholecystectomy: A new cause of intraperitoneal granulomas. J Clin Pathol 1996;49(1):84–5. [CrossRef]
[Pubmed]
10.
Pantanowitz L, Prefontaine M, Hunt JP. Cholelithiasis of the ovary after laparoscopic cholecystectomy: A case report. J Reprod Med 2007;52(10):968–70.
[Pubmed]
11.
Tursi JP, Reddy UM, Huggins G. Cholelithiasis of the ovary. Obstet Gynecol 1993;82(4 Pt 2 Suppl):653–4.
[Pubmed]
12.
Hassler KR, Collins JT, Philip K, Jones MW. Laparoscopic Cholecystectomy. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Lila Marshall - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sharlin Varghese - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mary Ciranni-Callon - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Lila Marshall et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}