 |
Case Report
A rare case of early abdominal pregnancy (EAP)
1 MBChB, BMedSci, Foundation Year Two doctor, University Hospitals Sussex Trust, Brighton, Sussex, United Kingdom
2 MD, MRCOG, Senior clinical fellow, Kingston Hospitals NHS Trust, Kingston upon Thames, London, United Kingdom
3 FRCOG, MSc in Advanced Gynaecological Endoscopy, Consultant Obstetrics and Gynaecology, Frimley Health NHS Foundation Trust, Frimley, Surrey, United Kingdom
Address correspondence to:
Marta Mungai Ndungu
64B Springfield Road, Brighton, Sussex BN1 6DE,
United Kingdom
Message to Corresponding Author
Article ID: 100183Z08MN2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Ndungu MM, Thing R, Sankaran S. A rare case of early abdominal pregnancy (EAP). J Case Rep Images Obstet Gynecol 2024;10(2):34–40.ABSTRACT
Introduction: Abdominal pregnancy comprises 1% of ectopic pregnancies and is challenging to manage due to the associated significant morbidity and mortality. Abdominal pregnancy may be classified according to gestation and implantation site. Ultrasound imaging is the mainstay of diagnosis. Confirmatory tests include magnetic resonance imaging (MRI) and diagnostic laparoscopy.
Case Report: A 36-year-old patient, amenorrheic for 9–10 weeks, presented to the early pregnancy unit complaining of a one-day history of abdominal pain associated with an episode of vomiting. She denied vaginal bleeding and examination revealed left lower quadrant tenderness. Ultrasound imaging demonstrated a live abdominal pregnancy around 12 weeks’ gestation implanted on the left uterine surface. Following appropriate counselling, she opted for surgical management and consented to the termination of pregnancy. She underwent diagnostic laparoscopy which confirmed that the gestational sac was arising from the left lateral uterine angle and was densely adherent to the omentum and bowel. The procedure was converted to laparotomy to enable safe adhesiolysis and excision of the entire gestational sac. Postoperatively, she represented on day 12 with abdominal pain, fever and bleeding. Computed tomography of abdomen and pelvis (CT-AP) suggested left ureteric injury and she underwent retrograde double J urethral stent (JJ stenting) of the left ureter. Fortunately, the same healed with conservative management.
Conclusion: Abdominal pregnancy is rare and poses challenges in diagnosis and management. Once diagnosed, urgent surgical management is recommended given the high risk of complications including intra-abdominal bleeding and visceral injury. Therefore, each case requires a careful and considered treatment approach by a multi-disciplinary team.
Keywords: Abdominal pregnancy, Ectopic pregnancy, Non-tubal ectopic, Rare ectopic pregnancy
Introduction
Abdominal pregnancy is defined as pregnancy which occurs in the abdominal cavity outside the female reproductive organs. It is extremely rare, comprising of 1% of all ectopic pregnancies. It occurs in 1/2200 to 1/10,200 pregnancies [1]. An abdominal pregnancy is challenging to manage due to the associated significant morbidity and mortality. Mortality rates are 7.7 times higher than in tubal ectopic pregnancy and 89.8 times higher than in intrauterine pregnancy [2].
Abdominal pregnancies can be classified by gestation into early (<20 weeks) or late (>20 weeks), as well as into primary or secondary depending on implantation site. Primary abdominal pregnancies implant directly into the abdominal cavity and its organs, apart from the Fallopian tubes and ovaries. Whereas secondary abdominal pregnancies initially start in the female reproductive organs but then become expelled and subsequently become implanted within the abdominal cavity [1].
Studdiford characterized the first case of a primary abdominal pregnancy in 1944 and established diagnostic criteria for primary abdominal pregnancy: (1) normal tubes and ovaries, (2) no evidence of uteroperitoneal fistula, (3) pregnancy related solely to the peritoneal surface, and (4) no evidence of secondary implantation following initial primary tubal nidation [3].
There are no clinical symptoms of abdominal pregnancy that distinguish it from a tubal ectopic pregnancy, so it requires a low threshold of suspicion. Diagnosis may be reached through transvaginal ultrasound imaging in combination with an elevated ß-human chorionic gonadotropin (hCG) level. Although transvaginal ultrasound is the diagnostic modality of choice, it is limited in accurately differentiating early abdominal pregnancy from other more common types of ectopic pregnancies. Other diagnostic modalities include MRI which may be valuable in planning surgical management, and diagnostic laparoscopy [1],[4].
The management of early abdominal pregnancy (EAP) remains challenging due to the increased risk of complications and high mortality rates. Early abdominal pregnancies are therefore usually treated as non-viable pregnancies and the aim of management is to terminate the pregnancy either medically or surgically, depending on patient factors and wishes [1]. Cases of abdominal pregnancies have been reported globally, yet fewer have been reported in the United Kingdom perhaps due to the accessibility of extensive antenatal care available. We present a case of an early abdominal pregnancy with extensive adhesions to various abdominal viscera and how the case was managed through surgical intervention.
Case Report
A 36-year-old woman gravida 3 para 1+1 presented to the emergency department with a one day history of worsening abdominal pain not alleviated by paracetamol and one episode of vomiting. She had no vaginal bleeding, bowel, or urinary symptoms. She was amenorrheic with a positive pregnancy test, estimated 9–10 weeks pregnant through natural conception.
She had a background of irregular periods, two in vitro fertilization (IVF) pregnancies (one successful and one failed) and history of laparoscopic ovarian cystectomy for endometrioma. Her previous successful pregnancy was conceived through IVF and she had a spontaneous vaginal delivery at 36 weeks’ gestation three years ago.
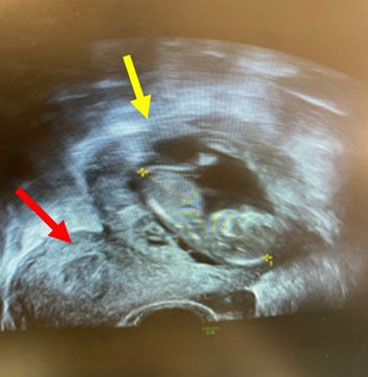
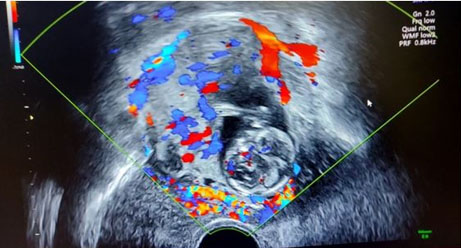
On abdominal examination she was tender on palpation at the umbilicus and left lower quadrant. Speculum examination showed normal findings. Blood pressure was 95/56 mmHg and other observations were in normal range. Routine blood tests were normal. Transabdominal and transvaginal ultrasound scans were performed in early pregnancy unit (EPU). They revealed an abdominal pregnancy in the left adnexa, close to the superior surface of the uterus (Figure 1). The pregnancy measured 12+ weeks gestation with a crown-rump-length (CRL) of 57 mm and with a positive heartbeat. There was adequate liquor, and no significant free fluid was seen. Empty uterine cavity and gestational sac surrounded by bowel were the criteria used to diagnose abdominal pregnancy in her case (Figure 2 and Figure 3). The diagnosis was confirmed by second consultant and a multidisciplinary team (MDT) discussion of management occurred. She was in significant discomfort and was admitted to the hospital. She and her partner were counseled about the risks of continuing the pregnancy, explaining the significantly increased morbidity and mortality of this kind of pregnancy. They opted for surgical management of the abdominal pregnancy which was carried out promptly the following day. Blood was crossmatched and requested in time for the surgery. The general surgical team was alerted prior to the surgery as loops of bowel were seen around the gestational sac on ultrasound.
Surgical management
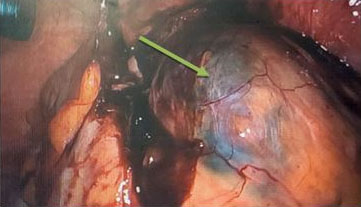
Diagnostic laparoscopy showed the ectopic pregnancy to be arising from the left lateral angle of the uterus and 200–300 mL of the hemoperitoneum. Significant viscera of the omentum and bowel were adherent to the gestational sac (Figure 4). The omentum was released from the pregnancy sac laparoscopically. The sigmoid colon and sigmoid mesentery were seen to be densely adhered to the gestational sac thereby significantly distorting the pelvic anatomy, so the approach was converted to laparotomy through a Pfannenstiel incision. A harmonic scalpel was used to release the dense bowel adhesions from the surface of the pregnancy sac. Adhesiolysis was carried out carefully by the general surgeon. The gestational sac was then clamped and separated from the superior surface of the uterus (Figure 5). No injury to the bowel or other organs was noted intraoperatively. The estimated blood loss was 350 mL. The operation was carried out by experienced consultant general surgeon and consultant gynecologists. The patient received tranexamic acid and intravenous Augmentin 1.2 g intraoperatively. The post-operative plan for the patient included intravenous fluids for the next 48 hours, regular analgesia, low molecular weight heparin for 10 days and repeat ß-hCG monitoring weekly until it became negative. The post-operative inpatient admission lasted five days and the patient was clinically stable on discharge.
The patient re-presented on day 12 post-operation with worsening abdominal pain, fever, and bleeding. Computed tomography-abdomen and pelvis suggested urinoma secondary to left mid to distal ureteric injury. She was treated for intra-abdominal sepsis with antibiotics and fluids. Cystoscopy was carried out and JJ stents of the left ureter were inserted. Ultrasound-guided drainage of the urinoma was also done. The ureteric injury fortunately healed with conservative management, and she was followed up by the urology team.


Discussion
Abdominal pregnancy is undoubtedly rare—with a reported incidence of 10.9 in 100,000 deliveries and 9.2 in 1000 ectopic pregnancies [2]. Early abdominal pregnancy poses challenges in diagnosis, carries a significant risk of complications and mortality therefore requiring timely treatment. The etiology of these uncommon events may be explained; in this case that we present, histology proved this to be a secondary abdominal pregnancy which originated as a tubal ectopic pregnancy. Following rupture and re-implantation, secondary abdominal pregnancies may adhere to any organ or structure in the abdominal cavity including bowel, omentum, uterus, and pelvic wall [5],[6]. This case saw the pregnancy sac was indeed attached to such structures. The implantation site of the EAP onto a highly vascularized surface in the abdominal viscera increases the possibility of separation of the gestational sac from these structures during pregnancy and subsequently causing a major hemorrhage. The case required prompt management following diagnosis, and treatment was carefully planned with measures taken to prepare for the possibility of extensive hemorrhage. Judicious pre-operative diagnosis is therefore paramount to optimize management of abdominal pregnancy and minimize complications. This will allow medical teams to plan and coordinate the necessary personnel, equipment, and resources to improve patient outcomes.
Diagnosis of abdominal pregnancy is invariably difficult and oftentimes missed—as outlined by a recent study looking at 163 extrauterine abdominal pregnancies, only 45% of cases were correctly diagnosed during the antenatal period [7]. Diagnosis should be based on history, physical examination, and imaging. A case report in Italy by Gerli et al. highlights challenges clinicians face in diagnosis of EAP and has put forward echographic diagnostic criteria: (1) Absence of intrauterine gestational sac, (2) absence of both an evident dilated fallopian tube and a complex adenexal mass, (3) a gestational cavity surrounded by loops of bowel and separated by peritoneum, and (4) a wide mobility similar to fluctuation of the sac, particularly evidence with a gentle pressure of the transvaginal probe toward the posterior cul-de-sac [4]. Using this they were successfully able to diagnose EAP in an 8 weeks’ pregnant and asymptomatic patient, distinguishing EAP from a tubal ectopic pregnancy which was initially suspected. The patient was managed using laparoscopy, remained well post-operation and discharged the day after surgery. Similarly in our case, ultrasound diagnosis was through the identification of an empty uterus (Figure 2 and Figure 3) next to a gestational sac surrounded by loops of bowel and confirmed by a senior gynecology consultant.
Comparably, a case in Hong Kong demonstrated EAP at a later gestation of 16 weeks, diagnosed using ultrasound scan (USS) on routine antenatal check. Abdominal and vaginal ultrasound scans revealed an empty uterus and ectopic gestational sac at the right adenexal area with placenta posteriorly in the pouch of Douglas [8]. The patient opted for surgical management but in this case, they performed a laparotomy. The patient remained well post-procedure and was discharged on day 7 post-operation. These cases underpin the importance of ultrasound diagnostic criteria of EAP, especially in the face of clinical uncertainty; for example, where a pregnant patient is asymptomatic. Conversely, the case we present showed the patient complained of non-specific abdominal pain. This reinforces that a diagnosis of EAP requires the whole clinical picture to be considered and warrants clinicians to investigate and assess patients thoroughly when presenting in pregnancy with various symptoms, especially: recurrent abdominal pain, fetal malpresentation, and unusual ultrasound findings [6]. Teaching antenatal USS operators to purposefully inspect the uterus on USS, using carefully outlined diagnostic criteria and a high clinical suspicion of EAP will incite greater confidence in identifying abdominal pregnancy on USS. Magnetic resonance imaging can aid the diagnosis. In our case, as the patient’s presentation was acute pain, we did not have time to perform MRI prior to surgery and ultrasound criteria was sufficient for diagnosis and surgical planning.
Reports of abdominal pregnancies across geographical locations show varying outcomes which are largely dependent on access to antenatal scanning services and medical care [6],[7],[8]. Remote and rural areas continue to have limited access to USS and therefore abdominal pregnancies are more likely to progress into later gestation, as demonstrated by a case report in Cameroon where advanced abdominal pregnancy was diagnosed at term [7]. Yet again, the mother was asymptomatic throughout pregnancy and attended routine antenatal visits at a health center, each appointment deeming the pregnancy normal. Only, the health center had no access to USS. The first ultrasound scan in this pregnancy was at term when she presented with absent fetal movements to a hospital. USS showed a non-gravid uterus and a partially decomposed fetus at full term lying obliquely with the head in mother’s right upper quadrant. Management entailed exploratory laparotomy and delivery of fetus, estimated blood loss was 500 mL and antibiotics given. She was fortunately clinically well on discharge at day 8 post-procedure.
Even with access to antenatal USS in more developed parts of the world, abdominal pregnancies have been misdiagnosed and inadvertently managed conservatively. One such report in the United Kingdom illustrates a case where a woman presented on multiple occasions with non-specific abdominal pain and a palpable abdominal mass. Serial fetal monitoring and USS were misinterpreted as a viable singleton gestation with a large anterior cervical fibroid. At 35 weeks when she underwent Caesarean section, it was discovered that the uterus was separate from the pregnancy sac—which was exclusively encircled and attached to omentum. Abdominal pregnancy therefore was diagnosed at the laparotomy and delivery of the fetus [6].
Another report from Saudi Arabia exemplified a case of abdominal pregnancy which was missed antenatally despite multiple ultrasound scans which were misinterpreted as an intrauterine pregnancy in a bicornate uterus [5]. This abdominal pregnancy was similarly discovered during Caesarean section at term. On removal of the placenta, a massive bleed occurred from the placental bed, requiring intensive fluid resuscitation, transfusion of multiple blood products and intensive care admission. However, on day 10 post-Caesarean section, she was discharged with her newborn. Though positive outcomes were described for mother and baby in these cases, they are infrequent and are a result of misdiagnosis. Across the 163 cases of abdominal pregnancy studied by Nunyalulendho et al., poor outcomes were frequently observed. For instance, fetal or perinatal mortality secondary to prematurity or prolonged gestation in a compromised environment was 72%, along with pressure deformities in surviving babies. Maternal mortality was 12% and post-operative complications were hemorrhage and infection, affecting more than 50% of all patients, and 75% required blood transfusion [7].
The cases of missed and/or late abdominal pregnancy depict marked differences in the stage at which diagnosis was made and the attachment site of the pregnancy sac. Considering the above cases and their differences, it emphasizes the rarity of positive outcomes of continuing a pregnancy, as well as the importance of a preoperative diagnosis to optimize outcomes. Ultrasound scanning services available in an EPU, such as in our case, portrays the role that it plays in the successful non-invasive diagnosis and management of EAP. For this reason, accessibility to these services and trained personnel reduces the duration of time it takes to reach diagnosis and supports timely intervention, thereby reducing the chance of misdiagnosis and/or complications associated with a greater gestational age.
Reviews of various abdominal pregnancy cases show that as pregnancy gestation increases so does the risk of massive hemorrhage, sepsis, intestinal obstruction, disseminated intravascular coagulopathy, perforation of adjacent organs (bowel, bladder, abdominal wall), and subsequently fetal and/or maternal mortality [9]. Due to the significance of these risks, urgent management with medical, surgical or a combination approach is recommended. Medical therapeutic options include preoperative arterial embolization, methotrexate for feticide or as an adjunct post-operatively [9],[10]. Laparoscopy is the treatment of choice for early abdominal pregnancy and has benefits when compared to laparotomy: reduced duration of operation, less intraoperative blood loss, less adhesion formation and shorter hospital admission [10]. However, laparotomy is the preferred approach in advanced pregnancy with extensive attachments, as well as in cases with an ectopic placenta [7]. In the case we present, the initial surgical approach utilized was indeed laparoscopic—this proved successful until it materialized the extent of adhesion of the pregnancy sac to the surface of the large bowel. The approach required to be converted to laparotomy and expertise was sought from a general surgical consultant to release the pregnancy sac. This captures the uncertainty of the management of EAP and how clinicians are required to be adaptable in their approach when facing difficulties in their initial management strategy.
The majority of literature quotes that ureteric injury rates at gynecological surgery might range from <1% to 2%. However, with significant distortion of pelvic anatomy due to adhesions and deep infiltrating endometriosis, rates of ureteric injury have been reported to be as high as 21% [11]. Electrocautery may be involved in up to one-quarter of ureteric injuries. However, only up to a third of ureteric injuries are recognized intraoperatively. A thermal injury to the ureter may result in delayed necrosis and/or fistula formation that will often present clinically between 10 and 14 days postoperatively [11]. In our case, due to dense bowel adhesions, anatomy was distorted. The ureteric injury is highly likely secondary to delayed injury from the use of diathermy. Insertion of ureteric stent and ureterolysis may potentially have avoided this injury. Fortunately, our patient healed with conservative management and stenting of ureter after urological input.
Conclusion
Abdominal pregnancies are unpredictable by nature, though overall, maternal mortality has been observed to decrease since accessibility to ultrasound scanning, use of laparoscopy and routine β-hCG monitoring has become more widely available in antenatal care. In this case, we demonstrated the importance of timely intervention through an EPU and efficient ultrasound diagnosis. In conclusion, abdominal pregnancy carries with it numerous complications that are difficult to predict and manage. Therefore, each case requires careful diagnosis to inform and optimize management, considering gestation and maternal factors.
REFERENCES
1.
Agarwal N, Odejinmi F. Early abdominal ectopic pregnancy: Challenges, update and review of current management. The Obstetrician & Gynaecologist 2014;16(3):193–8. [CrossRef]

2.
Atrash HK, Friede A, Hogue CJ. Abdominal pregnancy in the United States: Frequency and maternal mortality. Obstet Gynecol 1987;69(3 Pt 1):333–7.
[Pubmed]
3.
Scadron EN. Primary peritoneal pregnancy. Am J Obstet Gynecol 1957;73(3):686–9. [CrossRef]
[Pubmed]
4.
Gerli S, Rossetti D, Baiocchi G, Clerici G, Unfer V, Di Renzo GC. Early ultrasonographic diagnosis and laparoscopic treatment of abdominal pregnancy. Eur J Obstet Gynecol Reprod Biol 2004;113(1):103–5. [CrossRef]
[Pubmed]
5.
Dahab AA, Aburass R, Shawkat W, Babgi R, Essa O, Mujallid RH. Full-term extrauterine abdominal pregnancy: A case report. J Med Case Rep 2011;5:531. [CrossRef]
[Pubmed]
6.
Varma R, Mascarenhas L, James D. Successful outcome of advanced abdominal pregnancy with exclusive omental insertion. Ultrasound Obstet Gynecol 2003;21(2):192–4. [CrossRef]
[Pubmed]
7.
Nkusu Nunyalulendho D, Einterz EM. Advanced abdominal pregnancy: Case report and review of 163 cases reported since 1946. Rural Remote Health 2008;8(4):1087.
[Pubmed]
8.
Kun KY, Wong PY, Ho MW, Tai CM, Ng TK. Abdominal pregnancy presenting as a missed abortion at 16 weeks' gestation. Hong Kong Med J 2000;6(4):425–7.
[Pubmed]
9.
Rahaman J, Berkowitz R, Mitty H, Gaddipati S, Brown B, Nezhat F. Minimally invasive management of an advanced abdominal pregnancy. Obstet Gynecol 2004;103(5 Pt 2):1064–8. [CrossRef]
[Pubmed]
10.
Poole A, Haas D, Magann EF. Early abdominal ectopic pregnancies: A systematic review of the literature. Gynecol Obstet Invest 2012;74(4):249–60. [CrossRef]
[Pubmed]
11.
Minas V, Gul N, Aust T, Doyle M, Rowlands D. Urinary tract injuries in laparoscopic gynaecological surgery; prevention, recognition and management. The Obstetrician & Gynaecologist 2014;16(1):19–28. [CrossRef]
SUPPORTING INFORMATION
Acknowledgments
Thank you to Frimley Park Hospital EPU.
Author ContributionsMarta Mungai Ndungu - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Rakesh Thing - Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sridevi Sankaran - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementVerbal informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Marta Mungai Ndungu et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}