 |
Case Report
MRI and placenta accreta: Keys for its interpretation in images, regarding a case
1 Radiology Resident, Facultad de Medicina Clínica Alemana de Santiago, Universidad del Desarrollo, Vitacura, Santiago, Chile
2 Radiologist, Fellowship in Abdominal Imaging, Departamento de imágenes abdominales, Clínica Alemana de Santiago, Vitacura, Santiago, Chile
3 Radiologist, Departamento de imágenes abdominales, Clínica Alemana de Santiago, Vitacura, Santiago, Chile
4 Gynecologist, Clínica Alemana de Santiago, Vitacura, Santiago, Chile
5 Pathologist, Clínica Alemana de Santiago, Vitacura, Santiago, Chile
Address correspondence to:
Francisca Aliaga
Avenida Vitacura 5951, Vitacura, Santiago,
Chile
Message to Corresponding Author
Article ID: 100186Z08FA2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Aliaga F, del Campo F, Cocio R, Schiappacasse G, Blanco S, Pires Y. MRI and placenta accreta: Keys for its interpretation in images, regarding a case. J Case Rep Images Obstet Gynecol 2024;10(2):50–53.ABSTRACT
Introduction: Placenta accreta spectrum (PAS) refers to the abnormal adherence of the placental trophoblast to the uterine myometrium. Several conditions are associated with its development. Ultrasound is the imaging modality of choice for antenatal diagnosis. In cases of doubt, magnetic resonance (MR) plays a leading role, due to its high performance, and contributes to surgical planning. The final diagnosis is made in the surgery, with subsequent confirmation by pathology. The objective of this article is to present a case of placenta increta, focused on the imaging findings in magnetic resonance imaging (MRI).
Case Report: We present a case of a 35-year-old woman with a history of 2 previous cesarean sections and chronic hypertension, who presented a 23-week pregnancy with obstetric ultrasound showing placenta accreta. An MRI was performed, and it showed signs of placenta accreta, with no evidence of transmural extension to adjacent organs. At 34 weeks, a cesarean section and hysterectomy were performed, with no evidence of bladder invasion.
Conclusion: The diagnosis of PAS is made antenatal with ultrasound, but MRI has been used in some cases, with some characteristic features that every radiologist should know.
Keywords: Hysterectomy, Magnetic resonance, Placenta accreta, Ultrasound
Introduction
Placenta accreta spectrum (PAS) disorders represent abnormal implantation of placental components into the uterine myometrium and remain the leading cause of peripartum hysterectomy in Western countries. The main risk factors of PAS correspond to conditions that are associated with scars or lesions of the uterine wall [1].
Ultrasound is the method of choice for antenatal diagnosis, due to its wide availability; however, it is affected by amniotic fluid, intestinal gas, and the position of the placenta. In cases of diagnostic doubt or characterization of the involvement, magnetic resonance (MR) plays a leading role, due to its high resolution and little involvement of the aforementioned factors. Magnetic resonance makes it possible to define more precisely the involvement of adjacent organs in case of suspected placenta percreta, and thus contributes to surgical planning [1],[2],[3],[4],[5].
The precise diagnosis is made in the surgical act due to the impossibility of separating the placenta from the uterus, with subsequent pathological confirmation.
The objective of this article is to present a case of placenta increta, focused on the imaging findings in MRI.
Case Report
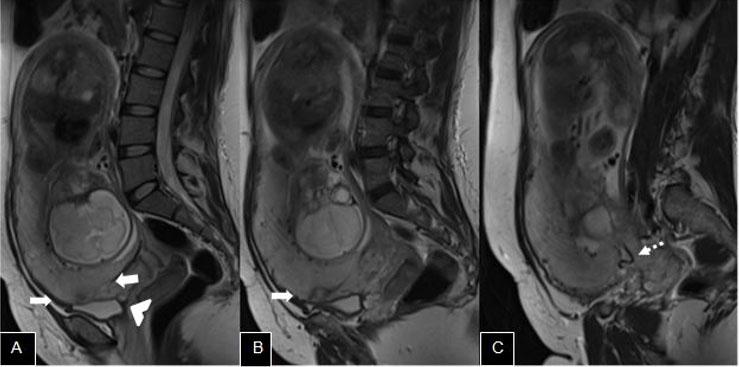
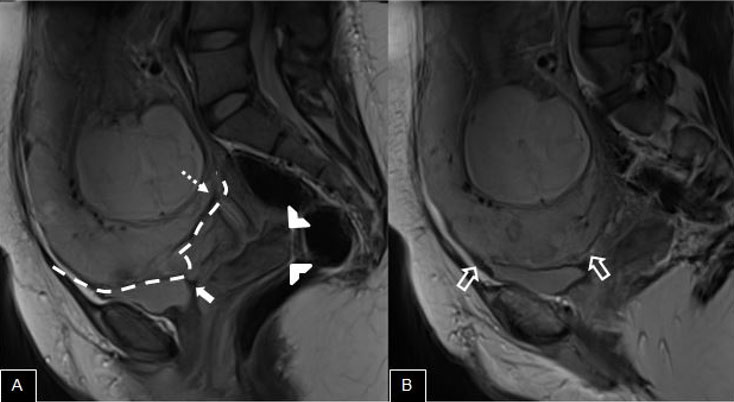
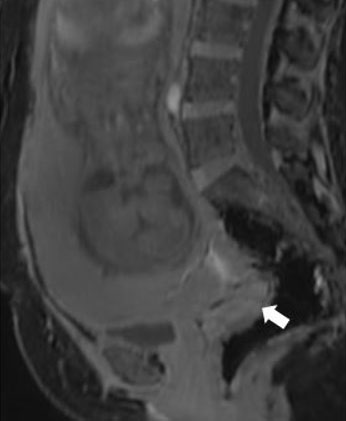
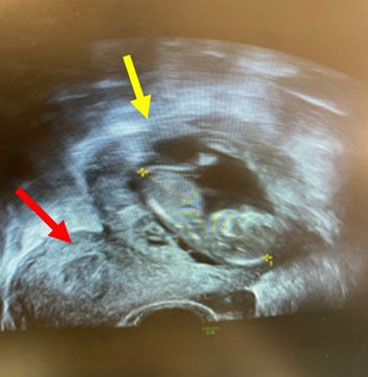
We report a case of a 35-year-old female patient with a history of 2 previous cesarean sections and chronic hypertension, who presented a 23-week pregnancy with obstetric ultrasound showing a totally occlusive anterior placenta, with some placental lacunae, thinning of the perivesical myometrium, and loss of a clear zone, consistent with placenta accreta (Figure 1). At 27 weeks of pregnancy, she consulted for heavy metrorrhagia, without pain. She was hospitalized for observation and fetal maturation. It was decided to complete the study with MRI to evaluate possible interconsultation with urology. Magnetic resonance imaging showed uterine bulge, with an hourglass shape, anterior and low insertion placenta, determining occlusion of the internal cervical os, as well as low-signal bands on T2WI and some aberrant vascular structures especially at its anterior–inferior edge, as well as some lobulation, findings that suggest accreta, with no signs of transmural extension to adjacent organs (Figure 2, Figure 3, Figure 4, Figure 5).
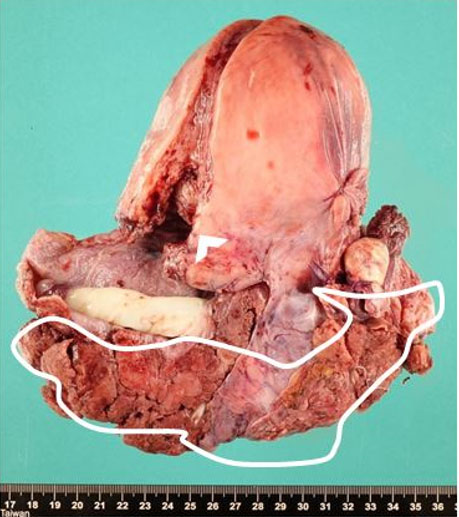
At 34 weeks, the fetal heart rate dropped, with sustained bradycardia, so she was transferred to the ward. A cesarean section and hysterectomy were performed, where uterine rupture was evidenced with 700 cc of hemoperitoneum. There was no evidence of bladder invasion. The surgical specimen was sent for pathological examination. The uterus, partially opened at the anterior wall, showed a placental disc firmly attached to the lower uterine segment that was thinned and deeply occupied by placental tissue (Figure 6).


Discussion
The imaging study of PAS is essential for proper diagnosis and management, with ultrasound being the modality of choice due to its wide availability. In a systematic review that included 54 studies, the sensitivity of 2D ultrasound of the third trimester was 87% and the specificity 86%, demonstrating its high value. It can show numerous placental lacunae, loss of the retroplacental clear zone, thinning of the myometrium, and extraplacental extension [5].
However, in certain cases, it is necessary to complement the study with an MRI, especially when there are diagnostic doubts or for surgical planning, like in this case. In this context, the optimal evaluation is at 28–32 weeks of pregnancy, after this period it is difficult to evaluate the placenta due to prominence of cotyledons and myometrial thinning [2],[4]. Several recent meta-analyses show an overall MRI sensitivity of 86.5–94.4% and a specificity of 96–98.8% in predicting the depth of placental invasion [2].
Recently, the Society for Abdominal Radiology (SAR) and the European Society for Urogenital Radiology (ESUR) issued a joint consensus statement for MRI of placenta accreta spectrum disorders, calling for recommendations to establish a uniform technique, a lexicon to describe the findings, and a structured report [3]. They described seven MRI features of PAS disorders that include intraplacental T2-dark bands, which is the more sensitive feature for the diagnosis of PAS disorders [3], placental or uterine bulge, myometrial thinning, bladder wall interruption, focal exophytic mass, loss of T2-hypointense retroplacental line, and abnormal vascularization of the placental bed.
These predictive signs of PAS disorders must be interpreted appropriately because some of them can be observed in patients with advanced pregnancies, such as myometrial thinning. This is why, as previously mentioned, it is important to perform the MRI at the appropriate stage of pregnancy, to avoid misinterpretations.
Accurate evaluation of MRI allows to reduce the morbidity and mortality of patients, helping clinicians to decide the best surgical management, be it performing a hysterectomy or a more conservative surgical management.
Conclusion
The diagnosis of PAS has increased in recent times, mainly in the West, due in part to the increase in the number of cesarean sections and older maternal age, which has led to an increase in the number of peripartum hysterectomies. Ultrasound is the first imaging modality to be performed due to its high availability, low cost, and good performance in antenatal diagnosis; however, MRI is the choice in selected cases of patients in whom ultrasound evaluation is limited or for surgical planning, having high sensitivity and specificity in the diagnosis of placenta accreta, mainly in the evaluation of extramural involvement, with some characteristic features that we should be capable to recognize.
REFERENCES
1.
Lin H, Li L, Lin Y, Wang W. Accuracy of magnetic resonance imaging in diagnosing placenta accreta: A systematic review and meta-analysis. Comput Math Methods Med 2022;2022:2751559. [CrossRef]
[Pubmed]

2.
Patel-Lippmann KK, Planz VB, Phillips CH, Ohlendorf JM, Zuckerwise LC, Moshiri M. Placenta accreta spectrum disorders: Update and pictorial review of the SAR-ESUR joint consensus statement for MRI. Radiographics 2023;43(5):e220090. [CrossRef]
[Pubmed]
3.
Jha P, P?der L, Bourgioti C, et al. Society of Abdominal Radiology (SAR) and European Society of Urogenital Radiology (ESUR) joint consensus statement for MR imaging of placenta accreta spectrum disorders. Eur Radiol 2020;30(5):2604–15. [CrossRef]
[Pubmed]
4.
Kapoor H, Hanaoka M, Dawkins A, Khurana A. Review of MRI imaging for placenta accreta spectrum: Pathophysiologic insights, imaging signs, and recent developments. Placenta 2021;104:31–9. [CrossRef]
[Pubmed]
5.
Maged AM, El-Mazny A, Kamal N, et al. Diagnostic accuracy of ultrasound in the diagnosis of Placenta accreta spectrum: Systematic review and meta-analysis. BMC Pregnancy Childbirth 2023;23(1):354. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
Departments of Radiology, Anatomical Pathology, Gynecology and Obstetrics, Facultad de Medicina Clínica Alemana, Universidad del Desarrollo, Santiago de Chile.
Author ContributionsFrancisca Aliaga - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Fernanda del Campo - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Rolando Cocio - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Giancarlo Schiappacasse - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sebastián Blanco - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yumay Pires - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Francisca Aliaga et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}