 |
Case Report
A large cervical fibroid polyp: Case report and management challenges in a low resource setting
1 Department of Obstetrics/Gynecology, University of UYO, Uyo, Nigeria
2 Department of Obstetrics/Gynecology, University of UYO Teaching Hospital, Uyo, Nigeria
3 Department of Anaesthesia, University of UYO Teaching Hospital, Uyo, Nigeria
4 Department of Pathology, University of UYO, Uyo, Nigeria
Address correspondence to:
Aniekan Monday Abasiattai
Department of Obstetrics/Gynecology, University of UYO, Uyo, Nigeria,
Nigeria
Message to Corresponding Author
Article ID: 100231Z08AA2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Abasiattai A, Atat B, Ebu A, Abudu K. A large cervical fibroid polyp: Case report and management challenges in a low resource setting. J Case Rep Images Obstet Gynecol 2026;12(1):49–53.ABSTRACT
Introduction: Cervical fibroid polyps (CFPs) are reported to be very rare. When large, they may result in varying clinical presentations, diagnostic difficulties, management challenges and significant morbidity and mortality.
Case Report: We hereby report the case of a 33-year-old primiparous lady who presented with abnormal vaginal bleeding and was found to be severely anemic (PCV 20%) with a firm, non-tender, smooth-surfaced mass that protruded through the cervical rim. The large 6 cm CFP was successfully removed and the patient had a good outcome.
Conclusion: This case report underscores the necessity of a thorough clinical examination including a vaginal examination in all patients who have similar presentations, to enable prompt and timely diagnosis and appropriate management.
Keywords: Cervical fibroids, Cervical fibroid polyps, Cervical myoma, Fibroids
Introduction
Uterine fibroids, also known as uterine leiomyomas, are benign monoclonal tumors of the myometrium [1]. They are the most common neoplasms in reproductive-age women and are particularly predominant in those who are black, in whom they develop earlier, grow much larger, and cause more severe symptoms [2]. It is estimated that the uteri of 70–80% of black women will harbor fibroids during their lifetime, and fibroids tend to cause significant morbidity in this group of women [3].
Fibroids are located in different parts of the uterus in relation to the serosa or endometrium [4]. Those in the uterine corpus are initially interstitial or intramural and, depending on their subsequent development, can either become subserous or submucous or remain intramural. Rarely, fibroids could develop between the layers of the broad ligament (Intraligamentary fibroids) and the stroma of the cervix (cervical fibroids) [4].
Cervical fibroids are reported to be exceedingly rare, occurring in 0.6% to 2% of fibroids [5] with some recent reports stating prevalence rates of 1–2% [6] and 2–2.5% [7]. Their rarity has been attributed to the sparseness of smooth muscles in the cervical stroma (<10%) [8]. They are usually solitary, arising either from the supravaginal or the vaginal portion of the cervix, and may coexist with other fibroid nodules in the body of the uterus. They may be interstitial, subserous, or very rarely submucous [8]. Submucous cervical fibroids may develop a stalk or pedicle, become polypoidal, and protrude through the cervical canal or even the vagina, i.e., a cervical fibroid polyp (CFP) [5],[8].
Due to its unique location and peculiar characteristics, the clinical presentations of CFPs may vary, leading to delay in the presentation of patients and in the receipt of appropriate treatment, diagnostic difficulties, and resultant significant morbidity and mortality [9].
We hereby report the case of a 33-year-old primiparous lady who presented with a large cervical fibroid polyp and also discuss our experience in its management. The rarity of this disorder, the diagnostic difficulty associated with it, and challenges with its management stimulated this report.
Case Report
A 33-year-old Para 1+0 lady presented with complaints of abnormal vaginal bleeding for nine months. Initially, she noticed her periods had increasingly become heavy and were associated with the passage of clots. She then also developed intermenstrual bleeding two months later, which increased in severity becoming worse two days prior to presentation, prompting her to present in our facility. There was associated dizziness, but no postcoital bleeding, dyspareunia, dysmenorrhea, or urinary symptoms.
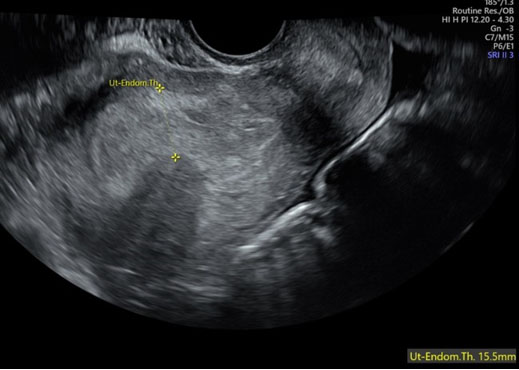
She had received several medications and blood transfusions and had undergone a series of ultrasound scans in the course of her previous hospital consultations and treatments. The first scan done in a diagnostic laboratory six months prior to presentation, showed myomas in the myometrium, free adnexa, and normal endometrium. The second scan, conducted in a health facility a month later, revealed an empty, slightly bulky, anteverted uterus with a 5 mm thick endometrial stripe, normal ovaries, and normal abdominal organs. The third and final scan, which was done a week before she presented in our facility, revealed mild dilatation of the secondary calyces and renal pelvis of both kidneys, an anteverted uterus measuring 120.1 mm × 58.2 mm × 56.4 mm with a clear endometrium (9.98 mm thick) and a large cervix (48.1 mm in transverse diameter) which was heterogeneous in echogenicity, suggesting cancer of the cervix. She had a full-term supervised pregnancy and an uncomplicated vaginal delivery of a live male baby three years before presentation.
On examination, she was moderately pale. Abdominal examination did not reveal any abnormality. Vaginal examination revealed an enlarged barrel-shaped cervix with a firm, non-tender, reddish-brown smooth-surfaced mass protruding through it, surrounded by the cervical rim (Figure 1). It was difficult to delineate the upper aspect of the mass. The uterus was 12 weeks in size, firm, and nodular. The adnexa were normal and rectal examination did not reveal any abnormality. A tentative diagnosis of a cervical fibroid was made to exclude a submucous fibroid polyp.
The packed cell volume (PCV) was 20% (Hb 6.7 g/dL), urea, creatine, electrolytes, and urinalysis did not reveal any abnormality. She was given oral norethisterone acetate and transfused with three units of whole blood. The PCV rose to 32%, and she was scheduled for examination under anesthesia and possibly laparotomy.
Under anesthesia, in theatre, re-examination revealed the mass to be protruding through the cervix, surrounded by its rim. It was attached to a stalk that extended into the cervical canal; the upper aspect of the stalk could not be ascertained. The abdomen was then entered through a Pfannenstiel incision; the uterus, which was equivalent to a 12-week gestation, was exteriorized, and was found to contain a solitary small subserous fibroid and tiny intramural fibroid seedlings, which were removed. There was no submucous fibroid, and no stalk or pedicle in the uterine cavity. A transverse incision was then made on the enlarged barrel-shaped cervix, and the large cervical myoma was identified, attached by a stalk approximately 6 cm long to the anterior aspect of the upper part of the cervical canal. The stalk was then ligated above the myoma, near its origin, and divided below the ligature. The fibroid polyp, which measured 6.0 × 4.5 × 4.5 cm (Figure 2), was subsequently removed through the vagina by a third assistant. The stump was doubly ligated and the cervix repaired. The uterus was reconstituted, and the abdomen was closed. Her postoperative period was uneventful, and she was discharged on the fourth postoperative day.
At the follow-up visit, she was devoid of symptoms, and her general condition was satisfactory. The abdominal wound had healed well, the uterus was normal-sized, the cervix was normal, and a repeat ultrasound revealed normal pelvic organs and normal kidneys, with no calyceal dilatation.
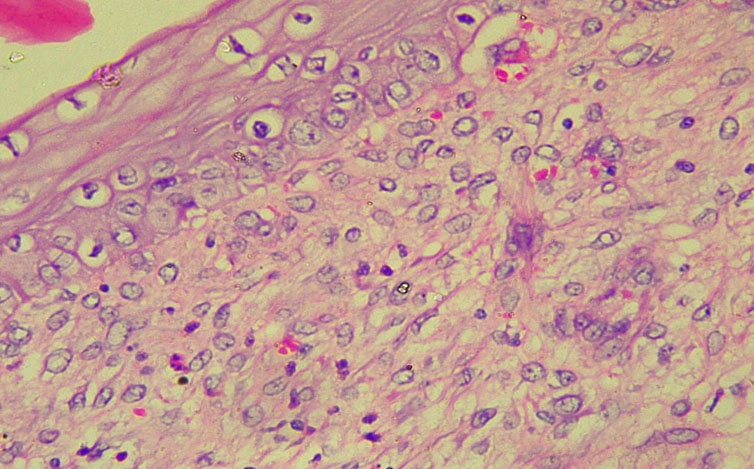
Histological examination of the polyp revealed an overlying stratified squamous epithelium with atrophy and sub-epithelium containing a similar, benign mesenchymal neoplasm composed of proliferating mature smooth muscle cells, disposed in a crisscross pattern, admixed with extensive areas of hyaline degenerative changes. The tumor cells possessed plump, spindle, bland nuclei and abundant cytoplasm, thus confirming CFP (Figure 3).


Discussion
Cervical fibroid polyps arise mainly from the supravaginal portion of the cervix and often present as symptomless small masses, particularly in their early stages of development [5],[8]. Large CFPs (>4 cm in size) as occurred in our patient, are reported to be very rare and due to their presenting symptoms, peculiar nature, and unique anatomic location, may pose diagnostic difficulties and management challenges leading to life-threatening complications [8],[9],[10],[11].
The most common symptom associated with a CFP is documented to be abnormal vaginal bleeding (heavy menstrual bleeding, intermenstrual bleeding or postcoital bleeding), as seen in our patient [12]. Other presenting symptoms include dysmenorrhea, dyspareunia, chronic pelvic or back pain, infertility, abnormal vaginal discharge, and the feeling of a lump in the vagina [5]. Due to their proximity to the pelvic organs, CFPs may also cause pressure symptoms such as constipation, urinary frequency, urgency, and urinary retention [10]. Pressure on the ureters or their distortion by the enlarged fibroid polyp could lead to hydronephrosis and destruction of the renal parenchyma with resultant chronic renal failure [12]. Our patient developed mild hydronephrosis, likely due to the attendant pressure, which resolved following removal of the fibroid polyp, as has been previously reported [12].
As typified by our patient, cervical fibroid polyps, particularly when large, can present as a mass protruding through the cervical canal or even the introitus [9]. Hence, to the detriment of affected patients, they have often been misdiagnosed as cervical cancer, incarcerated procidentia, chronic uterine inversion, or submucosal fibroid polyps [5],[9]. Our patient had received several forms of treatment before her presentation in our facility without any relief of her symptoms, probably because the precise diagnosis of her condition could not be made by the health providers who initially attended to her.
Following presentation in our facility, a thorough evaluation, including a careful vaginal examination, identified the fibroid mass protruding through the cervical os. An examination under anesthesia confirmed its origin and nature and revealed its attachment to a stalk. However, since the upper limit of the stalk could not be determined, a decision to proceed to a laparotomy was made, during which the stalk was discovered to originate from the anterior wall of the cervix, rather than the inner aspect of the myometrium, which is the site of origin of pedicles attached to submucous fibroid polyps. Pedunculated submucous fibroids may also develop a stalk, and depending on their length, prolapse through the cervix and/or vaginal canal, making them almost indistinguishable from CFPs [13].
Ultrasonography and magnetic resonance imaging (MRI) are reported to be crucial for identifying CFPs. However, MRI with a sensitivity of 100% has diagnostic superiority and is reportedly the most effective method for identifying these lesions. It provides detailed multiplanar imaging that allows for accurate assessment of the polyp’s location, number and characteristics [13]. Our patient had undergone several ultrasound scans, with only one revealing a possible cervical pathology. The scans were inconclusive and unhelpful in the diagnosis, and an MRI could not be carried out because it was unavailable when the patient was managed. This highlights the drawbacks of ultrasonography in our environment regarding the accuracy of reports, which could be misleading if entirely relied on.
Though the importance of ultrasonography and its role in medical diagnostics is clearly established, in Nigeria, recent reports reveal serious growing concern over its misuse leading to diagnostic inaccuracies and misinterpretations. This has been attributed to the proliferation of unqualified practitioners and untrained individuals performing ultrasound scans, deficiencies in training and expertise, and the absence of a robust regulatory framework for ultrasonographic practice in the country [14]. As shown in our case, this underscores the importance and need for the routine conduct of a thorough clinical examination, including a vaginal examination, whenever similar clinical scenarios are encountered.
Surgery which remains the primary treatment of choice particularly for large CFPs can be particularly challenging because of the risk of intraoperative hemorrhage and injury to adjacent structures like the bladder, ureters, and bowel [10]. Our patient did not have any of these complications, probably because the myoma was centrally located. The type of surgical procedure performed depends on the age, and reproductive wishes of the patient as well as the experience and personal preference of the surgeon [15] with vaginal myomectomy being recommended by most authors when conservation of the uterus is desired for future childbearing [5],[9]. This approach is reported to be safe and quick, especially when the mass is mobile and the pedicle can be easily avulsed, and also when there is adequate vaginal access [5],[9].
In our patient, however, it was virtually impossible to access the pedicle of the mass through the vagina, which led to our resorting to removing the mass abdominally. This also permitted the enucleation of the coexisting fibroid nodules in the body of the uterus which would have been impossible through the vagina. Early surgical treatment is imperative once the diagnosis of large CFPs is made, in order to prevent permanent damage to the renal parenchyma due to pressure from the mass, as was done in our case. After the mass was removed from our patient, the ultrasonographic features of hydronephrosis resolved.
Our case is unique and also interesting, not only because of the rarity of the disorder, but also because of the delay in establishing the definitive diagnosis, the difficulty in identifying the fibroid pedicle, the need for an EUA to determine the precise nature of the mass and the procedure performed to remove the mass.
Conclusion
Cervical fibroid polyps are very rare benign uterine tumors which can cause diagnostic difficulties and management challenges especially in low-resource settings such as ours. This case reports underscores the necessity of a thorough clinical examination including a vaginal examination in all patients with similar presentations, to enable prompt and timely diagnosis and appropriate management.
REFERENCES
1.
Senbango OC, Ottan TA, Akinlinsi FM, Oshodi YA, Rabiu KA, Adewunmi AA. Clinical presentation of uterine leiomyoma and the outcome of surgical management options in a Nigerian tertiary health facility. Annals of Health Research 2023;9(2):136–45. [CrossRef]

2.
Abasiattai AM, James R, Atat B, Edemekong V, Etuknwa U. Nonpuerperal uterine inversion complicating a huge prolapsed submucous myoma: A case report. Int J Gynaecol Obstet 2025;169(3):1240–2. [CrossRef]
[Pubmed]
3.
Igboeli P, Walker W, McHugh A, Sultan A, Al-Hendy A. Burden of uterine fibroids: An African Perspective, a call for action and opportunity for intervention. Curr Opin Gynecol Obstet 2019;2(1):287–94. [CrossRef]
[Pubmed]
4.
Van den Bosch T. Benign disease of the uterus. In: Edmonds DK, Less C, Bourne T, editors. Dewhurst’s textbook of obstetrics & gynaecology. 9th ed. Oxford: Blackwell; 2018. p. 823–34. [CrossRef]
5.
Gupta A, Gupta P, Manaktala U. Varied clinical presentations, the role of magnetic resonance imaging in the diagnosis, and successful management of cervical leiomyoma: A case series and review of literature. Cureus 2018;10(5):e2653. [CrossRef]
[Pubmed]
6.
Shiragur S, Patil BG, Talwade SA. A rare case report of giant degenerated cervical polyps. J Obstet Gynaecol Pract POGS 2025;3(1):52–54. [CrossRef]
7.
Bhardwaj B, Choudhary J, Kumar HS. Cervical fibroids: A surgical challenge. Medical Journal of Dr. D.Y. Patil Vidyapeeth 2024;17(2):417–22. [CrossRef]
8.
Agarwal M, Singh S, Agarwal R, Jaiswal S. Prolapsed giant cervical fibroid polyp. J South Asian Feder Obst Gynae 2016;8(1):77–78. [CrossRef]
9.
Odugu BU, Onyekpa IJ, Obi CK, Okafor I, Ugwu IA. Varied presentations of cervical fibroid polyps and the diagnostic role of early vaginal examination in a six case series study. Crit Care Obst Gynae 2021;7(7):46.
10.
Mahadrik K, Patidar R, Roy CPR. Infected prolapsed giant cervical fibroid polyp. Ann Case Report 2020;5:546. [CrossRef]
11.
Mujalda A, Kaur T, Jindal D, Sindhu V, Jindal P, Mujalda J. Giant cervical fibroid: A surgical challenge. Cureus 2023;15(5):e39602. [CrossRef]
[Pubmed]
12.
Yaliwal RG, Bidri SR, Polisetty LP. Acute prolapse of giant submucosal fibroid polyp mimicking uterine inversion – A rare case report. Indian J Obstet Gynecol Res 2022;9(1):121–3. [CrossRef]
13.
Uhasai K, Naik D, PR. Efficacy of MRI over ultrasound in evaluation of abnormal uterine bleeding with histopathological correlation. Cureus 2023;15(5):e38560. [CrossRef]
[Pubmed]
14.
Abayomi OA, Adeyemi AA, Awolowo TA, Olaogun DO, Oke OF, Akiinsipe CI, et al. The abuse of ultrasonography: A critical review of the Nigerian situation. Int J Radiol Sci 2024;6(1):04–07. [CrossRef]
15.
Hota BM, Geetha L, Prashanthi CG, Maeesha K. Lateral cervical fibroid: A case report with review of literature. Int J Reprod Contracept Obstet Gynecol 2025;14(11):4056–9. [CrossRef]
SUPPORTING INFORMATION
Author Contributions
Aniekan Monday Abasiattai - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Bless Atat - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Anietie Ebu - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kunle Abudu - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Aniekan Monday Abasiattai et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}