 |
Clinical Image
Cervical lymphadenopathy in pregnancy: Need for early biopsy
1 Senior resident, Department of Obstetrics and Gynecology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India
2 Junior resident, Department of Obstetrics and Gynecology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India
3 Head and Professor, Department of Obstetrics and Gynecology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India
4 Assistant Professor, Department of Obstetrics and Gynecology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India
Address correspondence to:
Kanagavarshani Murali
Senior resident, Department of Obstetrics and Gynecology, Women and Child Hospital, JIPMER, Puducherry 605006,
India
Message to Corresponding Author
Article ID: 101502Z01KM2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Murali K, Mittapally A, Dorairajan G, Sivaranjani P. Cervical lymphadenopathy in pregnancy: Need for early biopsy. Int J Case Rep Images 2025;16(1):76–79.ABSTRACT
No Abstract
Keywords: Cervical lymphadenopathy, Hodgkin lymphoma, Pregnancy, Tuberculosis
Case Report
A 27-year-old multigravida at 26 plus 5 weeks period of gestation (POG) with a previous cesarean section was referred to our outpatient department (OPD). She had swelling in the neck region for the past one and a half years. The swelling was noticed after her first childbirth in 2022. She had been empirically treated with anti-tubercular therapy (ATT) for nine months. However, her symptoms had not subsided. She had no complaints of fever, malaise, or night sweats during the presentation. There was no contact with tuberculosis.
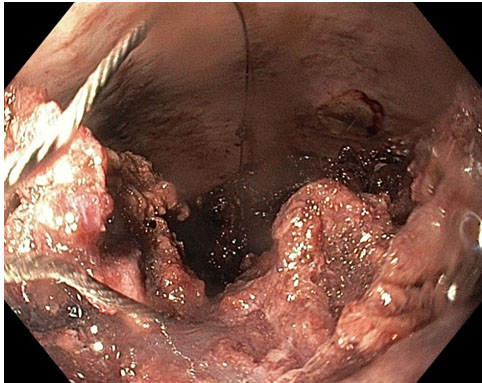
On examination, her vitals were stable. She had bilateral supraclavicular, cervical, and left axillary lymphadenopathy (Figure 1). The lymph nodes were matted, firm, non-mobile, non-tender, and not associated with skin changes or discharging sinuses. There was no organomegaly on abdominal examination, the uterus was 24 weeks, and the fetal heart rate was present.
The biopsy of the lymph node came out to be Hodgkin lymphoma—classical type. Magnetic resonance imaging of the chest, abdomen, and pelvis was done due to the potential radiation effects of computed tomography (CT) on the fetus. It revealed multiple enlarged cervical, supraclavicular, para-aortic, para-caval, and retroperitoneal lymph nodes with the left common iliac and axillary node enlargement. A diagnosis of stage 3 Hodgkin’s lymphoma was made. After a discussion with a multidisciplinary team Involving obstetricians and medical oncologists, the decision was taken for conservative management and to start chemotherapy after delivery. A summary of the patient’s obstetric follow-up is given below (Table 1).
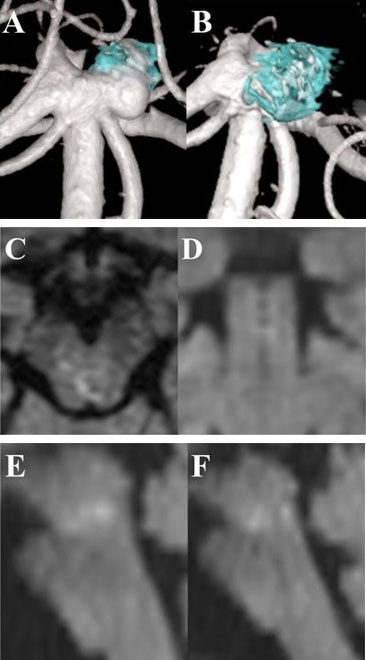
The patient was on regular follow-up in medical oncology and obstetric departments. At 36 +5 weeks of gestation, the patient was admitted for elective cesarean section because of a previous section with fetal growth restriction with oligohydramnios, and a cesarean section was done at 37 weeks. An alive female baby weighing 2.1 kilograms with APGAR 8 and 10 was delivered. The intraoperative period was uneventful, and the patient recovered completely. Positron emission tomography-computed tomography (PET-CT) done in the postpartum period revealed no progression in lesions compared to the previous magnetic resonance imaging (MRI). One-week post-surgery chemotherapy was started (ABVD—Adriamycin, Bleomycin, Vinblastine, Dacarbazine), and the patient was discharged on postoperative day 8 with allopurinol and low molecular weight heparin for postpartum thromboprophylaxis. Currently, she has received five cycles of chemotherapy, and the recent PET-CT showed 80% resolution of the lesion compared to pre-chemotherapy (Figure 2). She is planning for further cycles of chemotherapy. The baby is 5 months old and weighs 5 kilograms, with normal milestone development.



Discussion
Cervical lymphadenopathy refers to abnormal enlargement of lymph nodes in the neck. The causes can vary according to the age of the patient and geographical area from infection to malignancy. Considering the chronic symptoms and high prevalence in India tuberculosis is one of the primary differential diagnoses. However, our patient had already taken ATT and the symptoms have not improved. Studies have shown about 50% of lymphadenopathy is due to non-tuberculosis causes and human immunodeficiency virus (HIV) and lymphoma should always be considered in inconclusive cases [1],[2],[3]. Lymphomas are the fourth most common malignancy presenting in pregnancy with Hodgkin’s being the most common [4]. However, lymphomas presenting as cervical lymphadenopathy in pregnancy have not been reported. In a study conducted in India of all the cases presenting with cervical lymphadenopathy, only 8% had Hodgkin lymphoma [5].
In such cases, an excisional biopsy with histopathology is recommended for definitive diagnosis [6]. Due to the high proportion of cases of tuberculosis and poor patient follow-up many cases have been started on empirical therapy on initial presentation. Hence even in resource-poor settings like India, a fine needle aspiration cytology (FNAC) or biopsy is necessary before empirical therapy. This patient had no constitutional symptoms like fever or weight loss. A biopsy should have been considered in the initial presentation itself. Thus, this case report tells the importance of biopsy in all cases of cervical lymphadenopathy. Another possible cause to be ruled out is the co-existence of lymphoma and tuberculosis due to the immune-compromised state [7],[8], which is unlikely in our patient as the lymph nodes did not resolve after starting treatment.
Conclusion
Non-tuberculosis causes of cervical lymphadenopathy should always be considered, even in high-prevalence areas. An excisional biopsy of the nodes should be done in all cases without starting empirical ATT. The probable clues to non-TB etiology are supraclavicular lymphadenopathy, no contact with tuberculosis, lack of constitutional symptoms, and lack of response after eight weeks of ATT treatment.
REFERENCES
1.
Biswas G, Das A, Haldar D, Mukherjee A, Dutta S, Sinha R. Clinico-pathological correlates of cervical lymphadenopathy: A hospital based study. Indian J Otolaryngol Head Neck Surg 2013;65(Suppl 1):42–7. [CrossRef]
[Pubmed]

2.
Pandit S, Choudhury S, Das A, Das SK, Bhattacharya S. Cervical lymphadenopathy—pitfalls of blind antitubercular treatment. J Health Popul Nutr 2014;32(1):155–9.
[Pubmed]
3.
Bazemore AW, Smucker DR. Lymphadenopathy and malignancy. Am Fam Physician 2002;66(11):2103–10.
[Pubmed]
4.
Brenner H, Gondos A, Pulte D. Ongoing improvement in long-term survival of patients with Hodgkin disease at all ages and recent catch-up of older patients. Blood 2008;111(6):2977–83. [CrossRef]
[Pubmed]
5.
Waseem M, Abdul S, Gul Muhammad S. Hodgkin’s lymphoma in cervical lymphadenopathy. Pak J Med Sci 2008;24(1):118–21.
6.
Tuberculosis 13 January 2016 NICE no: 33 (Last updated: 16 February 2024). [Available at: https://www.nice.org.uk/guidance/ng33/resources/tuberculosis-pdf-1837390683589]
7.
Ouedraogo M, Ouedraogo SM, Cisse R, et al. Active tuberculosis in a patient with Hodgkin’s disease. A case report. [Article in French]. Rev Pneumol Clin 2000;56(1):33–5.
[Pubmed]
8.
Audebert F, Schneidewind A, Hartmann P, Kullmann F, Schölmerich J. Lymph node tuberculosis as primary manifestation of Hodgkin’s disease. [Article in German]. Med Klin (Munich) 2006;101(6):500–4. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
We thank the patient for agreeing to publish this article and images.
Author ContributionsKanagavarshani Murali - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Alekya Mittapally - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Gowri Dorairajan - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sivaranjani P - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Kanagavarshani Murali et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
/2025/images/figure1.1745483390.jpg){kind=link}
/2025/images/figure1.1745483390.jpg){kind=link}
/2025/images/figure1.1745483390.jpg){kind=link}
/2025/images/figure1.1745483390.jpg){kind=link}
/2025/images/figure1.1745483390.jpg){kind=link}
/2025/images/figure1.1745483390.jpg&title=Article%20Image){kind=link}
/2025/images/figure1.1745483390.jpg){kind=link}
/2025/images/figure2.1745483390.jpg){kind=link}
/2025/images/figure2.1745483390.jpg){kind=link}
/2025/images/figure2.1745483390.jpg){kind=link}
/2025/images/figure2.1745483390.jpg){kind=link}
/2025/images/figure2.1745483390.jpg){kind=link}
/2025/images/figure2.1745483390.jpg&title=Article%20Image){kind=link}
/2025/images/figure2.1745483390.jpg){kind=link}