 |
Case Report
Palatoglossal arch injury caused by denture clasps in an older adult with dementia
1 Assistant Professor, Department of Oral and Maxillofacial Surgery, Graduate School of Medicine, Kyoto University, Kyoto, Japan
2 Professor, Department of Oral and Maxillofacial Surgery, Graduate School of Medicine, Kyoto University, Kyoto, Japan
Address correspondence to:
Takuma Watanabe
54 Kawahara-cho, Shogoin, Sakyo-ku, Kyoto 606-8507,
Japan
Message to Corresponding Author
Article ID: 101503Z01TW2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Watanabe T, Mishima S, Hirota M. Palatoglossal arch injury caused by denture clasps in an older adult with dementia. Int J Case Rep Images 2025;16(1):80–84.ABSTRACT
Introduction: Older adults frequently use dentures, and patients with dementia can have difficulty manipulating dentures. Removable partial dentures frequently have sharp clasps which can cause severe complications.
Case Report: A woman in her 80s with Alzheimer’s disease was referred to our department with the chief complaint of inability to remove a maxillary partial denture. Intraoral examination revealed that the denture clasps had penetrated the right palatoglossal arch mucosa and were tightly fixed. By gently detaching the piercing clasps from the mucosa, the partial denture was retrieved.
Conclusion: Older adults with dementia and their caregivers should be regularly educated about denture accidents. If a denture causes oral mucosa injury, an oral surgeon may treat it in the Emergency Room. Knowledge of oral anatomy is essential for safe denture removal.
Keywords: Dementia, Denture clasp, Palatoglossal arch
Introduction
Recently, with the rapid aging of the population, the number of older adults with dementia has increased in Japan [1]. In several older adults, dentures are indispensable for the maintenance of mastication [1],[2]. Older adults with mild to moderate dementia are able to insert and remove dentures without assistance; however, patients with severe dementia have difficulty recognizing the orientation of the dentures or manipulating them [1],[3], leading to complications such as trauma [3].
Removable partial dentures are a simple, cost-effective treatment option for tooth replacement in partially edentulous patients [3],[4]. However, removable partial dentures frequently have clasps for retention [3]. Sharp clasps can cause mucosal erosion, perforation, or severe complications [5],[6]. The treatment for denture clasp injury includes manual removal alone or in combination with hemostasis using sutures or topical hemostatic agents, or extraction of the abutment tooth [3].
Here, we report a unique case in which denture clasps penetrating the palatoglossal arch mucosa in an older adult with dementia were successfully removed.
Case Report
A woman in her 80s was unable to remove her partial denture after eating in the evening, and her family called emergency medical services. The paramedics who arrived at the scene had noted that she was conscious and tachycardic with a heart rate of 82 beats/min and a blood pressure of 172/81 mmHg. Respiratory rate was 18/min, and oxygen saturation was 98% on room air. The patient was transported to our hospital, and referred to our department.
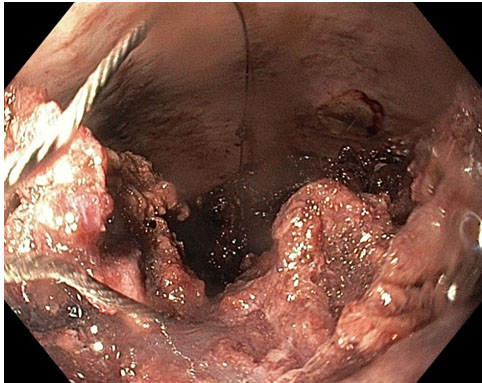
Based on the findings on brain magnetic resonance imaging and 123I-N-isopropyl-p-iodoamphetamine single-photon emission computed tomography, the patient had been diagnosed with Alzheimer’s disease approximately six months prior to presentation and was taking donepezil. The Mini Mental State Examination, Clock Drawing Test, and Frontal Assessment Battery scores were 18/30, 1/9, and 5/18 points, respectively. The patient also had been receiving denosumab for osteoporosis. Clinical examination revealed np cyanosis or dyspnoea. The heart rate, blood pressure, respiratory rate, and oxygen saturation on room air were 80 beats/min, 121/70 mmHg, 20/min, and 98%, respectively. Intraoral examination revealed that the maxillary partial denture clasps had penetrated the right palatoglossal arch mucosa, resulting in inability to remove the denture (Figure 1). No active bleeding was observed. The patient’s family reported that she had been using an upper partial denture for several years, wearing it during the day and while eating.
Based on the clinical diagnosis of partial denture stagnation due to clasp penetration into the palatoglossal arch, we tried to remove the partial denture with penetrating clasps under anterior direct vision of the palatoglossal arch alone. However, the denture clasps were tightly fixed to the mucosal wall of palatoglossal arch and could not be easily removed. Therefore, we assumed that the palatoglossal arch was pinched between the anterior and posterior clasps, and carefully rotated the partial denture while removing the clasps that were piercing the swollen palatoglossal arch anteriorly and posteriorly. Eventually, by gently detaching the piercing clasps from the mucosa, the partial denture with clasps was retrieved from the oral cavity without local anesthesia. During the procedure, vital signs were stable, and refusal behavior was not observed. After removal, no active bleeding or remaining foreign body was observed at the penetration site (Figure 2). Furthermore, the clasps of the retrieved partial denture did not appear to be fractured (Figure 3). The maxillary alveolar ridge was relatively flat with residual root pieces (Figure 4), whereas the mandibular arch had few natural teeth (Figure 5). Amoxicillin hydrate was administered orally at 750 mg daily for five days to prevent wound infection.
At the follow-up visit approximately one week later, uneventful recovery without intraoral wound infection was observed, and the patient reported no problems such as dysarthria or dysphagia (Figure 6). The offending partial denture was extremely loose; hence, we recommended replacement with new denture at a private dental clinic.






Discussion
The findings in this patient provided important clinical learnings. Regarding denture trauma, although several cases of clasp injury to the tongue have been reported [3], clasp penetration into the palatoglossal arch can also occur, particularly in older adults with dementia. Because release of clasps with specific structure which penetrate the palatoglossal arch are challenging in the confined environment of the oral cavity, careful maneuvers are required to avoid further trauma.
Older adults sometimes experience difficulty inserting and removing dentures [3],[7]. The ability of dependent older adults to use dentures is associated with their physical and mental capacities [8],[9],[10],[11], and dementia is associated with denture handling difficulties [1],[3]. Previous studies have reported that denture adaptability and inability to use dentures were associated with dementia or a lower level of activities of daily living [8],[9],[10],[11]. Dentures may become loose after prolonged use [12],[13] or when the abutment teeth anchoring the clasp become loose or are extracted [6],[13]. In addition, in older adults, the oral mucosal sensation can be reduced and motor control of the laryngopharynx can be poor [14],[15]. Loose dentures are relatively easy to dislodge and accidentally swallow [12],[13],[16]. Moreover, older adults may find using removable partial dentures difficult, especially the handling of the clasps [7], and partial denture clasps may traumatize the oral mucosa. Specifically, sharp and curved clasps can easily penetrate and embed into the soft tissue [17]. Clasp-penetration injuries are reported to occur frequently in the evening, potentially due to a greater number of opportunities for removing dentures at night after eating and before going to bed [3]. However, clasp-penetration injuries of the oral mucosa are significantly more common in the tongue, and mandibular free-end saddle dentures with premolar or canine clasps are the most frequently involved [3]. Our patient had dementia and continued to use an old and ill-fitting partial denture after loss of the right maxillary molar crowns. Consequently, when the denture was removed after eating in the evening, the denture clasps penetrated the right palatoglossal arch. Although small dentures without clasps usually travel through the alimentary tract after accidental ingestion [14], in our patient, a large partial denture with clasps was stuck in front of the pharynx due to clasp penetration. Palatoglossal arch injury caused by the molar clasps of the maxillary partial denture is rare. However, the situation can be considered fortunate because the denture was not accidentally swallowed.
A previous study evaluated the utility of newly developed denture placement and removal devices and revealed that the device was effective in the elderly [7]. On the other hand, nonmetal clasp dentures offer better aesthetics since their clasps are made of the same material as the prosthetic base, which helps increase patient’s acceptance [18]. To prevent clasp injury during denture placement and removal, the use of these devices or application of nonmetal clasp dentures, which do not require the use of sharp metal clasps, may be an option.
Regarding the treatment for the clasp-penetration injuries, the injuries are typically minor, with manual removal alone being the most common intervention [3]. Regarding denture impaction in the esophagus, in the absence of sharp clasps, endoscopic removal can be attempted; however, for dentures with sharp clasps, surgical removal is the first-line treatment to prevent esophageal injury by the clasps during the procedures [14]. Impacted dentures should be removed as soon as the diagnosis is made, because edema from local trauma tends to fix the denture more firmly making later manipulation increasingly difficult [13]. Moreover, since the clasps tend to pierce and embed into the surrounding tissues, forceful attempts at removal may exacerbate tissue injury and bleeding [3]. Regarding the pharyngeal anatomy, the soft palate is composed of several muscles: palatopharyngeus, palatoglossus, levator veli palatini, tensor veli palatini, and musculus uvulae [19]. The palatoglossus is an extremely thin muscle that makes up the palatoglossal arch [19]. The glossopharyngeal nerve travels anteriorly along the lateral surface of the pharynx in the palatoglossal arch [20]. Several approaches to block the glossopharyngeal nerve are used to adequately anesthetize the pharynx [20]. The least invasive approach involves placing cotton pledgets soaked with local anesthetic solution in the inferior-most portion of the soft-tissue fold that makes up the palatoglossal arch [20]. In addition, local anesthetic paste placed on a tongue depressor or solution provided as a gargle may be used for topical anesthesia [20]. In our patient, the sharp clasps for maxillary right first and second molars penetrated the anterior and posterior surfaces of the palatoglossal arch, respectively; thus, the arch was pinched anteroposteriorly and inflammatory edema occurred. Considering the orientation of the two sharp clasps relative to each other, we believed that the clasp was trapped in the palatoglossal arch and was difficult to release. Performing local infiltration anesthesia would have caused further edema, making clasp removal even more difficult and causing further tissue damage. Although the patient had dementia, she cooperated with our procedure; therefore, local or topical anesthesia was unnecessary. Eventually, based on the knowledge of the pharyngeal anatomy and denture structure, we could successfully remove the partial denture by safely detaching the penetrated clasps from the mucosa without local anesthesia.
Conclusion
Older adults with dementia who use dentures and their caregivers must be regularly educated about denture accidents. Caregivers should always consider the possibility of denture accidents and accurately evaluate the patient’s condition. Clinicians should carefully explain to patients how to remove dentures without pinching the soft tissue. Additionally, regular oral examinations, including denture adjustments, would likely prove helpful. Patients with clasp-penetration injury to the oral mucosa involving removable partial dentures may be treated by oral surgeons in the Emergency Room. Knowledge of the oral anatomy and denture structure is required for the safe release of clasps and denture removal.
REFERENCES
1.
Kubo KY, Iinuma M, Shibutani T, Ito M, Iwaku F. Denture-handling ability of elderly persons with dementia: Examination of time spent inserting and removing dentures. Spec Care Dentist 2007;27(4):149–53. [CrossRef]
[Pubmed]

2.
Shimazaki Y, Soh I, Saito T, Yamashita Y, Koga T, Miyazaki H, Takehara T. Influence of dentition status on physical disability, mental impairment, and mortality in institutionalized elderly people. J Dent Res 2001;80(1):340–5. [CrossRef]
[Pubmed]
3.
Iijima Y, Yamada M, Nakamura S, Hino S, Horie N, Kaneko T. Denture clasp injury of the oral mucosa. Gerontol Geriatr Med 2023;9:23337214231162750. [CrossRef]
[Pubmed]
4.
Campbell SD, Cooper L, Craddock H, et al. Removable partial dentures: The clinical need for innovation. J Prosthet Dent 2017;118(3):273–80. [CrossRef]
[Pubmed]
5.
Nwaorgu OG, Onakoya PA, Sogebi OA, Kokong DD, Dosumu OO. Esophageal impacted dentures. J Natl Med Assoc 2004;96(10):1350–3.
[Pubmed]
6.
Kim JH. Swallowed partial denture in severe intellectual disability patient. BMJ Case Rep 2021;14(1):e239945. [CrossRef]
[Pubmed]
7.
Kawasaki M, Nomura S, Okada N, Nomura A, Uoshima K. Evaluation of newly developed devices for denture placement and removal in the dependent elderly. Gerodontology 2012;29(2):e703–9. [CrossRef]
[Pubmed]
8.
Pregliasco F, Ottolina P, Mensi C, et al. Oral health profile in an institutionalized population of Italian adults with mental retardation. Spec Care Dentist 2001;21(6):227–31. [CrossRef]
[Pubmed]
9.
Chalmers JM, Carter KD, Spencer AJ. Oral diseases and conditions in community-living older adults with and without dementia. Spec Care Dentist 2003;23(1):7–17. [CrossRef]
[Pubmed]
10.
Taji T, Yoshida M, Hiasa K, Abe Y, Tsuga K, Akagawa Y. Influence of mental status on removable prosthesis compliance in institutionalized elderly persons. Int J Prosthodont 2005;18(2):146–9.
[Pubmed]
11.
Minakuchi S, Takaoka S, Ito J, Shimoyama K, Uematsu H. Factors affecting denture use in some institutionalized elderly people. Spec Care Dentist 2006;26(3):101–5. [CrossRef]
[Pubmed]
12.
Arora A, Arora M, Roffe C. Mystery of the missing denture: An unusual cause of respiratory arrest in a nonagenarian. Age Ageing 2005;34(5):519–20. [CrossRef]
[Pubmed]
13.
Bandyopadhyay SN, Das S, Das SK, Mandal A. Impacted dentures in the oesophagus. J Laryngol Otol 2014;128(5):468–74. [CrossRef]
[Pubmed]
14.
Toshima T, Morita M, Sadanaga N, et al. Surgical removal of a denture with sharp clasps impacted in the cervicothoracic esophagus: Report of three cases. Surg Today 2011;41(9):1275–9. [CrossRef]
[Pubmed]
15.
Gachabayov M, Isaev M, Orujova L, Isaev E, Yaskin E, Neronov D. Swallowed dentures: Two cases and a review. Ann Med Surg (Lond) 2015;4(4):407–13. [CrossRef]
[Pubmed]
16.
Hidaka H, Suzuki T, Toyama H, Kurosawa S, Nomura K, Katori Y. Dislocated dental bridge covering the larynx: Usefulness of tracheal tube guides under video-assisted laryngoscopy for induction of general anesthesia, thus avoiding tracheostomy. Head Face Med 2014;10:23. [CrossRef]
[Pubmed]
17.
Rajamani SK, Sahu P, Dandekar S. Prolonged impacted partial denture in the oropharynx during pregnancy and insights into its management – A case report. Walawalkar Int Med J 2018;5:45–50.
18.
Mendoza-Carrasco I, Hotta J, Sugio CYC, et al. Nonmetal clasp dentures: What is the evidence about their use? J Indian Prosthodont Soc 2020;20(3):278–84. [CrossRef]
[Pubmed]
19.
Cho JH, Kim JK, Lee HY, Yoon JH. Surgical anatomy of human soft palate. Laryngoscope 2013;123(11):2900–4. [CrossRef]
[Pubmed]
20.
Bhatnagar N, Lin CJ, Orebaugh SL, Vallejo MC. Regional anesthesia considerations for awake endotracheal intubation and prevention and management of dental injuries. Int Anesthesiol Clin 2012;50(1):1–12. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Takuma Watanabe - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sayaka Mishima - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Makoto Hirota - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Takuma Watanabe et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


/2025/images/figure1.1746270696.jpg){kind=link}
/2025/images/figure1.1746270696.jpg){kind=link}
/2025/images/figure1.1746270696.jpg){kind=link}
/2025/images/figure1.1746270696.jpg){kind=link}
/2025/images/figure1.1746270696.jpg){kind=link}
/2025/images/figure1.1746270696.jpg&title=Article%20Image){kind=link}
/2025/images/figure1.1746270696.jpg){kind=link}
/2025/images/figure2.1746270696.jpg){kind=link}
/2025/images/figure2.1746270696.jpg){kind=link}
/2025/images/figure2.1746270696.jpg){kind=link}
/2025/images/figure2.1746270696.jpg){kind=link}
/2025/images/figure2.1746270696.jpg){kind=link}
/2025/images/figure2.1746270696.jpg&title=Article%20Image){kind=link}
/2025/images/figure2.1746270696.jpg){kind=link}
/2025/images/figure3.1746270696.jpg){kind=link}
/2025/images/figure3.1746270696.jpg){kind=link}
/2025/images/figure3.1746270696.jpg){kind=link}
/2025/images/figure3.1746270696.jpg){kind=link}
/2025/images/figure3.1746270696.jpg){kind=link}
/2025/images/figure3.1746270696.jpg&title=Article%20Image){kind=link}
/2025/images/figure3.1746270696.jpg){kind=link}
/2025/images/figure4.1746270696.jpg){kind=link}
/2025/images/figure4.1746270696.jpg){kind=link}
/2025/images/figure4.1746270696.jpg){kind=link}
/2025/images/figure4.1746270696.jpg){kind=link}
/2025/images/figure4.1746270696.jpg){kind=link}
/2025/images/figure4.1746270696.jpg&title=Article%20Image){kind=link}
/2025/images/figure4.1746270696.jpg){kind=link}
/2025/images/figure5.1746270696.jpg){kind=link}
/2025/images/figure5.1746270696.jpg){kind=link}
/2025/images/figure5.1746270696.jpg){kind=link}
/2025/images/figure5.1746270696.jpg){kind=link}
/2025/images/figure5.1746270696.jpg){kind=link}
/2025/images/figure5.1746270696.jpg&title=Article%20Image){kind=link}
/2025/images/figure5.1746270696.jpg){kind=link}
/2025/images/figure6.1746270696.jpg){kind=link}
/2025/images/figure6.1746270696.jpg){kind=link}
/2025/images/figure6.1746270696.jpg){kind=link}
/2025/images/figure6.1746270696.jpg){kind=link}
/2025/images/figure6.1746270696.jpg){kind=link}
/2025/images/figure6.1746270696.jpg&title=Article%20Image){kind=link}
/2025/images/figure6.1746270696.jpg){kind=link}