|
Case Report
Pregnancy outcome after ultrasound guided drainage and sclerosis of cystic adenomyoma
1 Pennsylvania Hospital, Department of Obstetrics and Gynecology, Philadelphia, PA, USA
2 Hospital of the University of Pennsylvania, Division of Maternal Fetal Medicine, Philadelphia, PA, USA
3 Professor of Radiology, Division of Interventional Radiology, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, USA
4 Attending Physician, Division of Maternal Fetal Medicine, Hospital of the University of Pennsylvania, Philadelphia, PA, USA
5 Attending Physician, Department of Obstetrics and Gynecology, Pennsylvania Hospital, Philadelphia, PA, USA
Address correspondence to:
Jordann-Mishael Duncan
MD, Pennsylvania Hospital, 800 Spruce Street, Philadelphia, PA,
USA
Message to Corresponding Author
Article ID: 100097Z08JD2021
Access full text article on other devices

Access PDF of article on other devices

How to cite this article
Duncan J-M, Janssen M, Shlansky-Goldberg R, Hirshberg A, Neff P. Pregnancy outcome after ultrasound guided drainage and sclerosis of cystic adenomyoma. J Case Rep Images Obstet Gynecol 2021;7:100097Z08JD2021.ABSTRACT
Introduction: Cystic adenomyomas occur when the endometrial glands insert into the myometrium and can occur throughout a women’s reproductive life. Symptoms include uterine enlargement, menorrhagia, dysmenorrhea, and pelvic pain. Medical management of cystic adenomyomas includes oral contraceptives, the etonogestrel implant and gonadotropin releasing hormone (GnRH) agonists. Surgical management includes resection via hysteroscopy, laparoscopy or laparotomy, or interventional radiologic (IR) drainage and sclerosis of the mass. We report the first case of pregnancy after sclerotherapy for cystic adenomyoma.
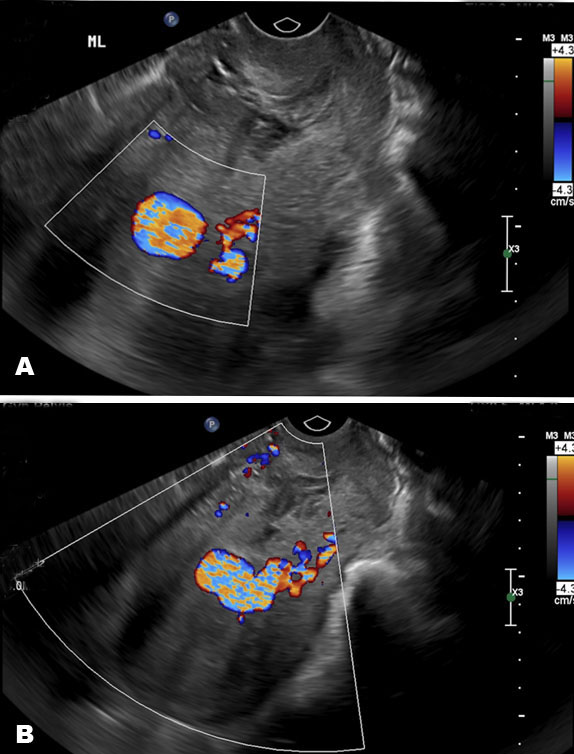
Case Report: This case describes a 22-year-old primiparous female with a history of repaired Tetralogy of Fallot, asthma, bronchiectasis, and previously described cystic adenomyomas. In summary, this patient was found to have a large septate myometrial cyst about 13.3 × 9.5 × 10.4 cm after a work up for abdominal bloating and constipation. She underwent several IR-guided procedures for drainage and sclerosis of these cysts. Three years after her last procedure the patient presented for prenatal care at 11 weeks gestation. Findings during her pregnancy included an anatomy ultrasound with a placental lake measuring approximately 4 cm, and numerous other smaller cysts without signs of a placenta accreta, and fetal growth restriction (FGR) at the 5th percentile diagnosed at 32 weeks gestation. She later underwent an uncomplicated induction of labor and vaginal delivery of a healthy 3110 g baby boy.
Conclusion: This is the first report of pregnancy after complex treatment for a cystic adenomyoma, which was complicated by FGR but had an overall good obstetric and neonatal outcome.
Keywords: Cystic adenomyoma, Fetal growth restriction, IR drainage and sclerosis, Placental cysts
SUPPORTING INFORMATION
Acknowledgments
Thank you to residents and staff of Hospital of University of Pennsylvania for taking excellent care of this patient.
Author ContributionsJordann-Mishael Duncan - Substantial contributions to conception and design, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Matthew Janssen - Substantial contributions to conception and design, Drafting the article, Final approval of the version to be published
Richard Shlansky-Goldberg - Substantial contributions to conception and design, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Adi Hirshberg - Substantial contributions to conception and design, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Pamela Neff - Substantial contributions to conception and design, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Jordann-Mishael Duncan et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.