 |
Case Report
Non-hemorrhagic unilateral adrenal infarct in pregnancy
1 The Ohio State University Wexner Medical Center, USA
Address correspondence to:
Yueyang F. Fei
The Ohio State University Wexner Medical Center, Department of Obstetrics and Gynecology, 395 W. 12th Ave, Columbus, OH 43210,
USA
Message to Corresponding Author
Article ID: 100044Z08YF2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Fei YF, Gonzalez-Brown V, Rood K, Buschur E. Non-hemorrhagic unilateral adrenal infarct in pregnancy. J Case Rep Images Obstet Gynecol 2019;5:100044Z08YF2019.ABSTRACT
Introduction: Adrenal infarct is a rare cause of abdominal pain, which is especially true in pregnancy. The symptoms and signs of insufficiency will depend on the amount of adrenal function lost. The adrenal gland has a unique vasculature that may facilitate infarction in a hypercoagulable state. Currently only limited case reports and small series describing evaluation and management of adrenal infarct are found in the literature. Unilateral adrenal infarct is a rare finding in pregnancy but an important diagnosis to consider to prevent incorrect management and worsening bilateral infarction.
Case Report: A 21-year-old G2P0010 presented at 29 4/7 weeks with sudden onset right upper quadrant and flank pain, fever, nausea, and vomiting. The patient was initially empirically treated for complicated urinary tract infection/pyelonephritis despite no clear laboratory evidence of infection. There was no evidence of adrenal insufficiency with the exception of fasting ketosis. The remainder of evaluation was unremarkable including ultrasounds and X-rays. Unilateral adrenal infarct was diagnosed on contrast-enhanced computed tomography with no associated hemorrhage. Thrombophilia assessment was notable for methylenetetrahydrofolate reductase (MTHFR) gene heterozygous and prothrombin G20210A gene heterozygous. She was treated with subcutaneous low molecular weight heparin (LMWH) through delivery and six weeks post-partum.
Conclusion: Unilateral non-hemorrhagic adrenal infarction may be an underdiagnosed cause of acute abdominal pain during pregnancy.
Keywords: Adrenal infarct, Pregnancy, Thrombophilia
Introduction
Bilateral adrenal infarction in pregnancy often presents with primary adrenal insufficiency, resulting in acute hypotension and shock. Unilateral adrenal infarction, however, may only present with vague abdominal pain, which may be similar to pain associated with preterm labor, placental abruption, or appendicitis [1]. This makes it challenging to confirm the diagnosis. Unilateral adrenal infarct is rare, though the pregnant state itself may constitute a thrombogenic state [2]. We present a case of a 29-week pregnant woman, with no significant past medical history and no history of previous thrombotic events, presenting with new onset right upper quadrant abdominal and flank pain, who was subsequently diagnosed with unilateral adrenal infarction. This case highlights the importance of suspicion of adrenal infarction in pregnant women with severe abdominal pain after ruling out other etiologies.
Case Report
A 21-year old G2P0010 presented at 29w4d with acute onset right-sided abdominal pain to her local Emergency Department. She described the pain as wrapping around her back and radiating to her right upper quadrant, associated with nausea and vomiting. The pain was initially constant but then became intermittent. There was no history of fever, chills, constipation, or urinary symptoms. Past medical and surgical histories were unremarkable. She denied family history of blood clots or clotting disorders. Her obstetrical history included a first trimester loss.
On presentation, she was clinically well-appearing; afebrile with blood pressure 134/77 mmHg, mild tachycardia with heart rate 112 beats per minute and respiratory rate 18 breaths per minute. Abdominal examination revealed moderate tenderness over the right upper quadrant with no rebound or guarding. Chest and cardiovascular examination were unremarkable. Cervical examination was unremarkable and fetal status was reassuring.
Laboratory evaluation included complete blood count with normal hemoglobin and platelets at 10.4 g/dL and 398x109/L, respectively. White blood cell count was initially noted at 14,500 cells/micrL (74.5% neutrophils, 15.5% lymphocytes, 8.0% monocytes, 0.3% eosinophils, 0.3% basophils), but on further evaluation notable for leukocytosis to 23,100 cells/micrL with left shift (81.0% neutrophils, 8.0% lymphocytes, 11.0% monocytes, 0% eosinophils, 0% basophils) within the first 24 hours. Liver function tests, amylase, and lipase were all within normal limits. Urine alysis showed no signs of infection. The patient developed a fever to 100.7°F (38.17°C) within the first day of her clinical presentation and was started empirically on IV Cefazolin 1g/8h for presumed pyelonephritis.
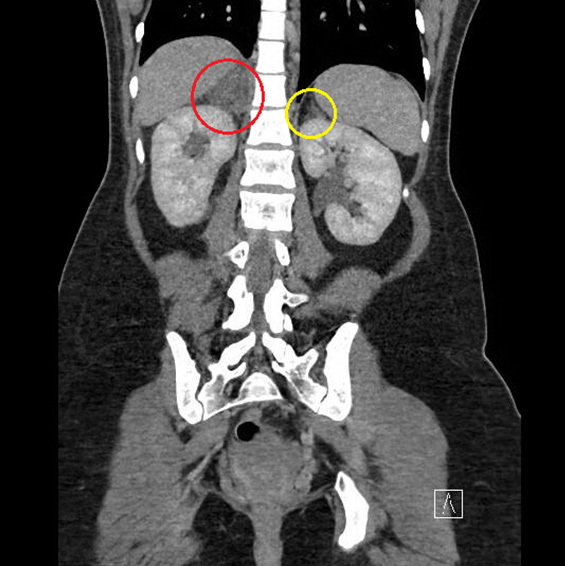
Initial imaging included a right upper quadrant ultrasound, renal ultrasound, and chest X-ray which were unremarkable. She was then transferred to our institution where antibiotics were discontinued due to no other signs of infection and negative urine culture. Due to the persistence of her abdominal pain, a computed tomography scan (CT A/P) was performed. As seen in Figure 1 and Figure 2, CT A/P showed normal appendix, but was concerning for right adrenal infarct with diffuse enlargement and hypoattenuation of the right adrenal gland with surrounding fat stranding. In light of this radiological finding, which was consistent with site of pain and acute clinical presentation, a diagnosis of right adrenal infarction was made. The patient was started on therapeutic subcutaneous low molecular weight heparin (LMWH) 70mg (1mg/kg) twice daily to prevent promulgation of adrenal infarction and prevent a similar event to contralateral adrenal gland.
Now, with an established diagnosis of adrenal infarction, additional labs were drawn. Adrenocorticotropic hormone (ACTH) was 14.0 pg/mL (9.0-50.0 pg/mL) and cortisol was 17.36 mcg/dL (3.09-22.40 mcg/dL), both within normal limits. This was followed by an appropriate response to high-dose ACTH stimulation test (cortisol rose to 45.05 mcg/ dL), confirming adequate adrenal function. Renin and aldosterone were found to be elevated as expected in pregnancy, at 66.7 pg/mL (4.2–52.5 pg/mL) and 81.0 ng/dL (<35.4 ng/dL), respectively. Chemistry was now noted to have bicarbonate 10 mmol/L (22–30 mmol/L), anion gap 16 mmol/L (3–13 mmol/L), elevated lipase 277 U/L (11–82 U/L), otherwise unremarkable. Arterial blood gas showed metabolic acidosis with pH 7.316 (7.35–7.45), pCO2 16.5 mmHg (32–48 mmHg), HCO3 8.2 mmol/L (22–26 mmol/L). Given the patient’s history of nausea and vomiting and poor oral intake, this was consistent with starvation ketosis. The patient’s electrolytes improved with bicarbonate replacement in maintenance IV fluids and improvement in her dietary intake. She showed no signs or symptoms of adrenal insufficiency, and never required steroid replacement.
A thrombophilia assessment showed negative antiphospholipid antibodies, as well as normal antithrombin III and protein C activity. She tested negative for factor V Leiden mutation. She was found to be positive for methylenetetrahydrofolate reductase (MTHFR) gene and prothrombin G20210A mutation heterozygous.
By the third day of admission, the patient’s symptoms improved, and she was discharged home on LMWH. The remainder of her pregnancy was uneventful. At full term, she had an uneventful vacuum assisted vaginal delivery. LMWH was continued for six weeks postpartum. The plan was to repeat thrombophilia panel six weeks after discontinuation of anticoagulation. However, patient recently presented to her obstetrician with a new pregnancy at 11 weeks. She has been restarted on anticoagulation for this current pregnancy.

Discussion
Adrenal infarction in pregnancy is a rare event with only case reports and case series reported in the literature. Bilateral adrenal infarction usually presents with adrenal insufficiency, which can lead to shock, sepsis, and death. Unilateral adrenal infarction can present with acute abdominal pain, nausea, vomiting, and mimic a wide range of other diagnoses. One review of MRIs performed over a ten year period at one institution for abdominal pain in pregnancy revealed a 1.3% incidence rate of infarcted adrenal gland [1].
Adrenal hemorrhage and infarction can be due to a variety of factors, including iatrogenic anticoagulation, thromboembolic disease, hypercoagulable state, sepsis, recent surgery, and trauma. Through extensive review of the literature, fifteen cases of adrenal infarction in pregnancy were identified, including one case of bilateral infarct. Many of the cases were reported in radiology literature to describe diagnosis of this rare finding, without further elaboration on details of the pregnancy [1]. Other reports have reported anti-phosopholipid antibody syndrome and other thrombophilia factors which may contribute to additional hypercoagulability. Our patient was found to have MTHFR gene and prothrombin G20210A mutation heterozygosity. Prothrombin G20210A mutations without a personal history of previous venous thromboembolism, carry a less than 1% risk of venous thromboembolism during pregnancy [3]. Our case is the first reported case in which two thrombophilia mutations have been identified. Although, pregnancy itself poses a thrombogenic risk, a patient that presents with clinical signs and symptoms for adrenal infarct should undergo a thrombophilia evaluation. Even in the setting of antiphospholipid syndrome, bilateral adrenal infarction is very uncommon, but important to diagnose to prevent further morbidity and mortality [4].
Previous observations have noted that the “stressed” adrenal gland has an increased susceptibility to acute hemorrhage and infarction. There are increased cortisol and ACTH levels in pregnancy, likely multifactorial in etiology, due to placental synthesis of ACTH and corticotropin releasing hormone (CRH), increased cortisol binding globulin during pregnancy, increased pituitary sensitivity to CRH, and cortisol feedback inhibition, which increases stimulation of the adrenal glands. The renin-angiotensin-aldosterone system is stimulated with increasing levels of aldosterone and renin throughout pregnancy to maintain sodium balance and volume status [2]. In addition, the adrenal glands are well-vascularized with arterial supply from the superior, middle, and inferior adrenal arteries. However, the adrenal vein is the sole source of venous drainage. The increased activity and blood flow, in combination with impaired blood return, could explain the increased risk of thrombosis in pregnancy.
Of the eight cases that specified laterality, seven of those cases identified right-sided adrenal infarct. This discrepancy could also be related to the anatomy of the adrenal gland and impaired venous drainage. The right adrenal vein drains to the inferior vena cava (IVC) directly whereas the left drains to the left renal vein, which then connects to the IVC. Compression of the IVC in pregnancy could cause venous stasis and clot formation, which has a greater impact on the right side due to the shorter right adrenal vein.
The use of anticoagulation in these instances must also be carefully considered as anticoagulation can worsen adrenal hemorrhage. In most case reports we were able to find, patients were started on anticoagulation, which was continued for a brief period postpartum. The majority of cases reported unilateral adrenal infarct with no evidence of adrenal insufficiency [5],[6]. Unilateral adrenal infarct is a rare finding in pregnancy, but an important diagnosis to consider to prevent incorrect management and worsening bilateral infarction. Our literature search also revealed four cases of adrenal hemorrhage which was identified on imaging. Half the cases presented with acute adrenal insufficiency requiring stress dose steroids and the other half presented with acute hemorrhage requiring immediate surgery. None of these cases were treated with anticoagulation prior to diagnosis. As far as it was observed, outcomes were generally positive for mother and fetus [7].
Our case highlights that adrenal infarction may complicate a normal pregnancy without any other recognized thrombophilic factors and should be included in the differential diagnosis of the acute abdomen in pregnancy. In these cases it is also important to monitor for signs or symptoms of adrenal insufficiency and treat with steroid replacement when applicable, as this can be a life-threatening complication.
Teaching points
- Patients who are found to have adrenal infarction should undergo thrombophilia work up to evaluate for underlying coagulopathies.
- Risks and benefits of anticoagulation should be considered in cases of adrenal infarction to prevent worsening clot burden and acute hemorrhage.
- Patients who present with adrenal infarction should be evaluated and monitored for signs of adrenal insufficiency and steroid replacement initiated if needed.
Conclusion
Pregnancy increases the risk of infarction of the adrenal glands through increased stimulation and venous stasis. This case emphasizes the importance of screening for adrenal insufficiency in patients with known hypercoagulable states presenting with abdominal pain, vomiting, and hemodynamic instability.
REFERENCES
1.
Glomski SA, Guenette JP, Landman W, Tatli S. Acute nonhemorrhagic adrenal infarction in pregnancy: 10-year MRI incidence and patient outcomes at a single institution. AJR Am J Roentgenol 2018;210(4):785–91.
[Pubmed]

2.
Carr BR, Parker CR Jr, Madden JD, MacDonald PC, Porter JC. Maternal plasma adrenocorticotrophin and cortisol relationships throughout human pregnancy. Am J Obstet Gynecol 1981;139(4):416–22. [CrossRef]
[Pubmed]
3.
ACOG Practice Bulletin No. 197: Inherited thrombophilias in pregnancy. Obstet Gynecol 2018;132(1):e18–34. [CrossRef]
[Pubmed]
4.
Espinosa G, Santos E, Cervera R, et al. Adrenal involvement in the antiphospholipid syndrome: Clinical and immunologic characteristics of 86 patients. Medicine (Baltimore) 2003;82(2):106–18.
[Pubmed]
5.
Aljenaee KY, Ali SA, Cheah SK, Alroomi MJ. Unilateral adrenal infarction in pregnancy secondary to elevated factor VIII. Saudi Med J 2017;38(6):654–6. [CrossRef]
[Pubmed]
6.
Green PA, Ngai IM, Lee TT, Garry DJ. Unilateral adrenal infarction in pregnancy. BMJ Case Rep 2013;2013. [CrossRef]
[Pubmed]
7.
Jonnalagadda K, Bhavani N, Pavithran PV, Kumar H, Menon UV, Chithra R. Spontaneous bilateral adrenal hemorrhage of pregnancy. Int J Reprod Contracept Obstet Gynecol 2017;6(2):772–5. [CrossRef]
SUPPORTING INFORMATION
Author Contributions
Yueyang F. Fei - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Veronica Gonzalez-Brown - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kara Rood - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Elizabeth Buschur - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Yueyang F. Fei et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}