 |
Case Report
Infiltrating tubular-papillary carcinoma of supernumerary left breast: A case report
1 Department of Obstetrics and Gynecology, Thiès Regional Hospital, The University of Thiès, Faculty of Health Sciences, Ex l0ème RIAOM, IBP: 9, Senegal
2 Department of Obstetrics and Gynecology, The University of Ziguinchor, Senegal
3 Anesthesial and Resuscitation, Thiès Barthimé hospital, Senegal
Address correspondence to:
Mariétou Thiam
Department of Obstetrics and Gynecology, Thiès Regional Hospital, The University of Thiès, Faculty of Health Sciences, Ex l0ème RIAOM, IBP: 967 Thiès,
Senegal
Message to Corresponding Author
Article ID: 100047Z08LG2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Gueye L, Thiam M, Gueye SM, Phiri A, Ndiaye MM, Mahamat S, Diop AP, Cisse ML. Infiltrating tubular-papillary carcinoma of supernumerary left breast: A case report. J Case Rep Images Obstet Gynecol 2019;5:100047Z08LG2019.ABSTRACT
Introduction: Supernumerary breast cancer is a rare phenomenon and diagnosis is delayed due to late consultation.
Case Report: A 58-year-old diabetic patient, agrand multiparas with history of exclusive breastfeeding. Examination on first consultation showed an ulcero-necrotic mass of the left axillar fistulized to the skin. Mammography concluded that the axillary polylobed, hypo-echogenic tissue formation was quite limited at 9 cm in the long axis containing cystic and necrotic sections. Otherwise, the breasts were normal-looking. Biopsy of the mass was in favor of tubulopapillary adenocarcinoma. The thoracic-abdominal computed tomography showed left tissue involvement, with most likely homolateral axillary ganglionic invasion. We administered six Adriamycin cyclophosphamide type neo-adjuvant chemotherapy treatment followed mastectomy of the supernumerary breast associated with a left lymph node curage. Histology of the operative piece conclusion was infiltrating tubulo-papillary adenocarcinoma Scarff-Bloom and Richardson II (SBR II) with the presence of tumor emboli. Resection margins were not invaded. 1/8 of the lymph nodes were invaded by malignant proliferation.
Conclusion: This case describes a rare diagnosis of tubularpapillary carcinoma on an ectopic breast of the axillary extension treated with neoadjuvant chemotherapy and a mastectomy of the supernumerary breast. As with breast cancers in our context, diagnosis is often made when the tumor is at an advanced stage making treatment more cumbersome and mutilating with lower chances of recovery.
Keywords: Cancer, Ectopic breast, Treatment
Introduction
Carcinomas of accessory breast tissue account for about 0.3% of all breast cancers [1]. In the majority of cases, the diagnosis is made at a late stage because of the delay in consultation [2]. Evans et al.[3] reported that 71% of ectopic breast cancers were located in the axilla. Breast tissues develop from the ectodermal ridges, also known as the milk lines, on the ventral surface of the body, which extend from the axillae to the inguinal regions and end on the medial aspect of the thighs on each side of the body [4]. Embryologically, ectopic breast tissue develops as a result of failed resolution of the mammary ridge, an ectodermal thickening that extends from the axilla to the groin [5]. Ectopic breast tissue may appear at any site along the milk line, but it occurs most commonly in the axilla; less commonly, it may appear in locations outside of the mammary ridge, including the face, middle back, buttock, posterior neck, chest, vulva, hip, posterior, flank and/or lateral thigh, shoulder and upper extremities [4],[6]. The diagnostic procedures and therapeutic management of accessory breast carcinoma are not definitively established. The present study aimed to perform an analysis in a case of infiltrating tubularpapillary carcinoma on a supernumerary breast of the left axiltreated with combination chemotherapy and surgery as well as to review the medical literature with regard to the clinical features, treatment methods and prognosis of this disease.
Case Report
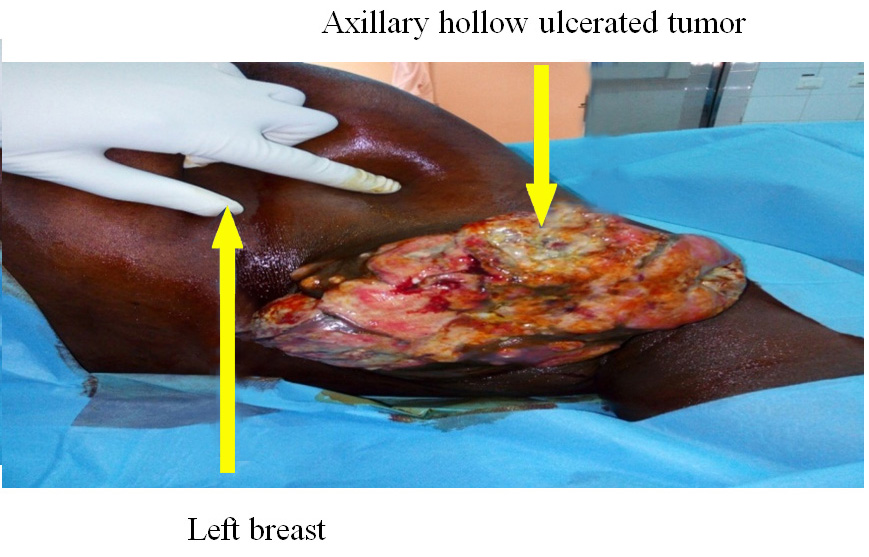
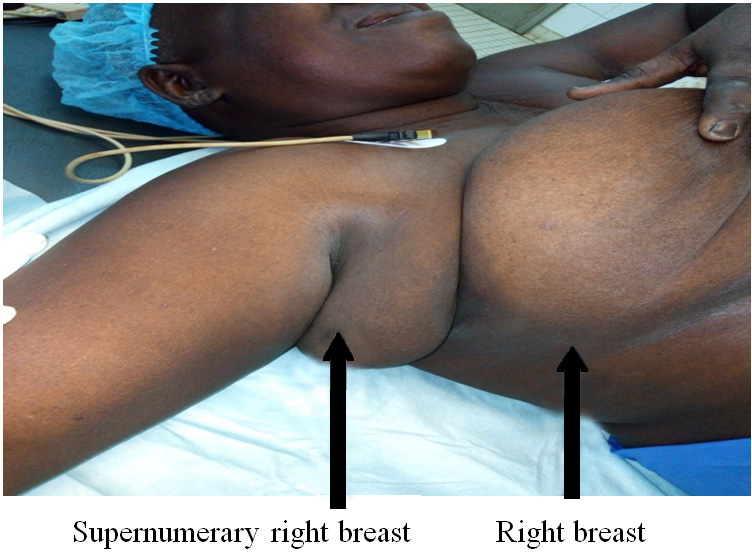
A 58-year-old diabetic patient on diet treatment only, gravida 10 para 9 with a history of exclusive breast feeding for 20 months of all her children. She was referred for an ulcerous-necrotic tumor of the left axillary extension. Examination at admission showed an ulcerous-necrotic mass of the left axillary extension fistulized at the skin (Figure 1). Comparative examination of the right axillary fossa found a supernumerary breast (Figure 2). Bilateral and comparative examination of the breasts was unremarkable.
On mammography, the axillary tissue like mass, was multi-lobbed, hypo-echoic and well outlined, at 9 cm long axis containing cysts and necrotic zones. Otherwise, the breasts appeared normal. A tubular-papillary adenocarcinoma was reported as final diagnosis.
In the complimentary tests reports, the CT scan showed a left tissue like mass with probable homo-lateral axillary lymph node involvement, as well as presence of a nonspecific 29 mm hypodense nodule of the spleen. Cardiac ultrasound and the biological assessment was normal. Breast MRI was not performed due to lack of means.
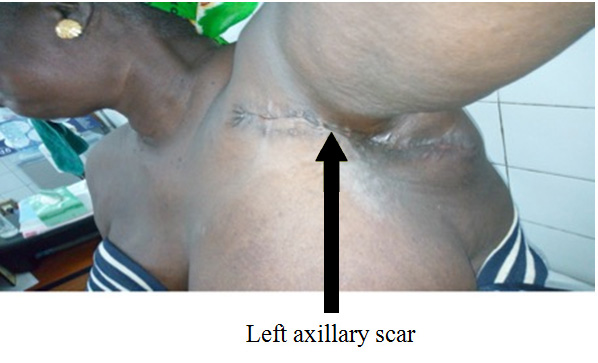
She benefited from neo adjuvant chemotherapy of adriamycin and cyclophosphamide AC type, six sessions with a partial response. Then a mastectomy associated with lymph node resection. A fusiform incision carrying all the supernumerary breast directed towards arm pit was realized dissecting up to the muscle. Then an opening of the clavi-pecto-axillary aponeurosis and curage of the two floors of BERG.Hemostasis was satisfactory and a Redon drain was placed in the mastectomy bed and closure achieved with separate stiches, and the specimen was sent to the histology laboratory (Figure 3).
Based on the histological findings an infiltrating tubular-papillary adenocarcinoma SBR II (3 + 3 + 1) with tumor emboli was diagnosed. The resection margins were not invaded. One-eighth of the lymph nodes were however, invaded by malignant proliferation. Postoperatively, a correct healing was obtained (Figure 4) and there was no recurrence even after 20 months of follow-up.

Discussion
Primary ectopic breast cancer occurs from aberrant or supernumerary breasts. It is rare and estimated at 0.3% of all breast cancer. 95% of ectopic breast cancer arise from aberrant mammary tissue (islets of non-organized secretory systems unconnected to the overlying skin), compared to 5% only in a supernumerary breast (an organized ductal system connected to the overlying skin via a nipple-areola complex) [1],[7]. It can present itself anywhere along the primitive milk line (galactic), most often the arm pit (60-70%) as described in our case and rarely on the thorax. (5-10%) [1], [8]. The diagnosis of supernumerary breast cancer follows the same diagnostic strategy as a regular breast cancer, namely: clinical examination, breast ultrasound, mammography and histological confirmation by Tru-Cut biopsy. Sometimes standard mammography may present technical difficulties depending on the location of the ectopic breast tissue due to its rare occurrence. In most cases, the diagnosis is delayed by an average of 40.5 months [8]. In our context, the diagnosis was made at a stage of neglected cancer [9] with loss of subcutaneous tissue and necrotic ulceration. MRI, which would have made it possible to better assess adjacent ipsilateral breast before surgery, was not performed due to lack of financial means, it is recommended to facilitate diagnosis and treatment in patients with masses in the galactic line [10]. The evaluation of the ipsilateral breast and the negative complimentary assessment allowed us to propose a conservative treatment with a possible radiotherapy. Radiotherapy is still difficult to access in our countries; in the GUEYE series (78.1%), patients treated for neglected breast cancer had not benefited [9]. Soufiane [11] and Aouad [12] reported 72.7% and 77.1% respectively of absence of radiotherapy.
According to literature, papillary carcinoma of the breast is a very rare entity and accounts for 0.5 to 1% of all breast carcinomas [13]. It is generally characterized by slow growth with a good prognosis. Invasive ductal carcinoma was the most common histological type, 50-79%, in these ectopic forms followed by medullary and lobular carcinomas 9.5% [8]. Therapeutic recommendations in literature follow standardized guidelines for breast cancer [1],[2],[7]. In view of tumor size, adjuvant chemotherapy type AC was proposed followed by supernumerary breast mastectomy; ipsilateral adjacent breast mastectomy provides no additional benefit and is no longer recommended [8].
Adjuvant radiotherapy should be considered to optimize loco regional control. A review of literature provides no formal guidance on the dose, fractionation and radiotherapy fields in this context. The treatment domains range from inclusion of the tumor bed alone, to the ipsilateral axillary and supraclavicular fossa, even in the absence of lymph node metastasis [7],[8]. In our case, a second line chemotherapy and a radiotherapy are considered.
Conclusion
This case describes a rare diagnosis of tubular- papillary carcinoma on an ectopic breast of axillary extension treated with neoadjuvant chemotherapy, supernumerary breast mastectomy and possible radiotherapy. As with breast cancer, in our setting, the diagnosis is often made at a locally advanced stage making the treatment heavier and more mutilating with less chance of healing.
REFERENCES
1.
Marshall MB, Moynihan JJ, Frost A, Evans SR. Ectopic breast cancer: Case report and literature review. Surg Oncol 1994;3(5):295–304. [CrossRef]
[Pubmed]

2.
Livesey JR, Price BA. Metastatic accessory breast carcinoma in a subcutaneous thoracic nodule. JR Soc Med 1990;83(12):799–800.
[Pubmed]
3.
Evans DM, Guyton DP. Carcinoma of the axillary breast. J Surg Oncol 1995;59(3):190–5.
[Pubmed]
4.
Hao JY, Yang CC, Liu FF, et al. Accessory breast cancer occurring concurrently with bilateral primary invasive breast carcinomas: A report of two cases and literature review. Cancer Biol Med 2012;9(3):197–201. [CrossRef]
[Pubmed]
5.
Howard BA, Gusterson BA. Human breast development. J Mammary Gland Biol Neoplasia 2000;5:119–37.
[Pubmed]
6.
Pathak S, Preston J. A rare case of multiple accessorybreast tissue in the axillae, lower abdomen and vulval areas. J Obstet Gynaecol 2007;27(5):531–3. [CrossRef]
[Pubmed]
7.
Madej B, Balak B, Winkler I, Burdan F. Breast Cancer Accessory: A Case Report. Adv Med Sci 2009;54(2):308–10. [CrossRef]
[Pubmed]
8.
Viscont G, Eltahir Y, Van Ginkel RJ, Bart J, Werker PM. Approach and management of primary ectopic breast carcinoma in the axilla: Where are we? A comprehensive historical literature review. J Plast Reconstr Aesthet Surg 2011;64(1):e1–11 [CrossRef]
[Pubmed]
9.
Gueye SMK, Gueye M, Moreau JC, et al. "Neglected" breast cancers: Experience of the Senology Unit of the Aristide University Hospital The Dantec of Dakar (Senegal). Journal of SAGO 2015;16(2):21–6.
10.
da Silva BB, dos Santos AR, Pires CG, Rosal MA, dos Santos LG, Lopes-Costa PV. Ectopic breast cancer in the anterior chest wall: A case report and literature review. Eur J Gynaecol Oncol 2008;29(6):653–5.
[Pubmed]
11.
Soufiane D. Management of advanced breast cancer in 402 cases at the Joliot Curie Institute in Dakar. Thesis Med Dakar 2015;25:185.
12.
Aouad L. Metastases of breast cancer in 96 cases collected at the Joliot Curie Institute in Dakar. Thesis Med Dakar 2004;40:125.
13.
El Mazghi A, Bouhafa T, Loukili K, El Kacemi H, Lalya I, Kebdani T, Hassouni K. Intracystic papillary carcinoma of the breast: Report of three cases. [Article in French]. Pan Afr Med J 2014;18:207. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Lamine Gueye - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mariétou Thiam - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Serigne Modoukane Gueye - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Adamson Phiri - Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mor Malick Ndiaye - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Souleymane Mahamat - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Alioune PierreDiop - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mamadou Lamine Cisse - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Lamine Gueye et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}