 |
Case Report
Pregnancy outcome after ultrasound guided drainage and sclerosis of cystic adenomyoma
1 Pennsylvania Hospital, Department of Obstetrics and Gynecology, Philadelphia, PA, USA
2 Hospital of the University of Pennsylvania, Division of Maternal Fetal Medicine, Philadelphia, PA, USA
3 Professor of Radiology, Division of Interventional Radiology, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, USA
4 Attending Physician, Division of Maternal Fetal Medicine, Hospital of the University of Pennsylvania, Philadelphia, PA, USA
5 Attending Physician, Department of Obstetrics and Gynecology, Pennsylvania Hospital, Philadelphia, PA, USA
Address correspondence to:
Jordann-Mishael Duncan
MD, Pennsylvania Hospital, 800 Spruce Street, Philadelphia, PA,
USA
Message to Corresponding Author
Article ID: 100097Z08JD2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Duncan J-M, Janssen M, Shlansky-Goldberg R, Hirshberg A, Neff P. Pregnancy outcome after ultrasound guided drainage and sclerosis of cystic adenomyoma. J Case Rep Images Obstet Gynecol 2021;7:100097Z08JD2021.ABSTRACT
Introduction: Cystic adenomyomas occur when the endometrial glands insert into the myometrium and can occur throughout a women’s reproductive life. Symptoms include uterine enlargement, menorrhagia, dysmenorrhea, and pelvic pain. Medical management of cystic adenomyomas includes oral contraceptives, the etonogestrel implant and gonadotropin releasing hormone (GnRH) agonists. Surgical management includes resection via hysteroscopy, laparoscopy or laparotomy, or interventional radiologic (IR) drainage and sclerosis of the mass. We report the first case of pregnancy after sclerotherapy for cystic adenomyoma.
Case Report: This case describes a 22-year-old primiparous female with a history of repaired Tetralogy of Fallot, asthma, bronchiectasis, and previously described cystic adenomyomas. In summary, this patient was found to have a large septate myometrial cyst about 13.3 × 9.5 × 10.4 cm after a work up for abdominal bloating and constipation. She underwent several IR-guided procedures for drainage and sclerosis of these cysts. Three years after her last procedure the patient presented for prenatal care at 11 weeks gestation. Findings during her pregnancy included an anatomy ultrasound with a placental lake measuring approximately 4 cm, and numerous other smaller cysts without signs of a placenta accreta, and fetal growth restriction (FGR) at the 5th percentile diagnosed at 32 weeks gestation. She later underwent an uncomplicated induction of labor and vaginal delivery of a healthy 3110 g baby boy.
Conclusion: This is the first report of pregnancy after complex treatment for a cystic adenomyoma, which was complicated by FGR but had an overall good obstetric and neonatal outcome.
Keywords: Cystic adenomyoma, Fetal growth restriction, IR drainage and sclerosis, Placental cysts
Introduction
Adenomyosis is a benign condition characterized by the presence of ectopic endometrial glands and stroma within the myometrium [1]. An adenomyoma can occur in either a nodular form appearing as a solid mass, or a cystic form. The incidence of cystic adenomyomas is not well described due to its rarity. Cystic adenomyomas can occur throughout a women’s reproductive life from adolescence through menopause. They occur when endometrial glands insert into the myometrium and in most cases contain hemorrhagic material [2].
Cystic adenomyomas are diagnosed with characteristic imaging. A case report of cystic adenomyoma in an adolescent describes that on T1-weighted magnetic resonance imaging (MRI) they appear as a hyperintense lesion. Additionally, on T2-weighted imaging cystic adenomyomas have a hypointense signal which reflects cyst wall thickening, myometrial hypertrophy, as well as an indeterminate intensity compatible with hemorrhagic or proteinaceous fluid [3].
There are other case reports that discuss management of cystic adenomyomas such as medical management which includes hormonal suppression of endometrial tissue with oral contraceptives, the etonogestrel implant and gonadotropin releasing hormone (GnRH) agonists [4],[5]. Refractory or severe cases may require surgical management which includes hysteroscopic ablation/resection, laparoscopic resection/enucleation, or laparotomy with resection. In the literature, there is one case that describes interventional radiologic (IR) drainage and sclerosis of myometrial masses [5].
To our knowledge, there are currently no cases in the literature with reports of pregnancy, or successful pregnancy outcomes, after treatment of these cystic adenomyomas. We report a case of pregnancy with a good outcome in a patient who previously received sclerosis therapy for large cystic adenomyomas.
Case Report
We present the case of a 22-year-old primiparous female with a past medical history significant for repaired Tetralogy of Fallot, asthma, bronchiectasis, and previously described cystic adenomyomas by Fuseini et al. To summarize the prior case report, the patient initially presented in 2014 for bloating and constipation, and was found to have an abdominal mass on pelvic exam. Ultrasound imaging at that time was consistent with a large simple ovarian cyst. She underwent a diagnostic laparoscopy with planned laparoscopic ovarian cystectomy, however laparoscopic findings showed a mass originating from the uterus and the procedure was then aborted.
After the procedure, the patient underwent an MRI which showed a large myometrial cyst about 13.3 × 9.5 × 10.4 cm with an inferior locule approximately 8.8 × 10.1 × 10.4 cm with simple appearing fluid and a superior locule approximately 3.5 × 6.6 × 7.7 with hemorrhagic material separated by a thick septation. On imaging there was no evidence of congenital uterine anomaly, with a single endometrial cavity, and normal ovaries with small ovarian lesions suggestive of endometriomas. She then underwent IR aspiration of the cyst with repeat imaging showing a decrease in size to 9.4 × 9.1 × 9.4 cm that correlated with symptomatic relief.
Over the next three years her symptoms intermittently recurred and imaging also demonstrated recurrence of myometrial cystic adenomas about 3–4 times in different locations of the uterus. During one recurrence, severe hydronephrosis from cyst compression of the ureter was noted, which resolved after drainage with no long-term renal damage. She underwent five additional IR aspirations over the course of three years. During three of the aspirations, ethanol sclerotic agents were used ranging from 10 to 200 mL. One the aspirations, 500 mg in 20 mL of doxycycline sclerosis was used. All of these procedures were all uncomplicated. She ultimately underwent medical management with GnRH agonist therapy for three months and transitioned to extended cycle oral contraceptives, and subsequently to an etonogestrel implant. Additionally, she was offered surgical management with myometrial cystectomy or hysterectomy, however, desired continued hormonal suppression with intermittent attempts at IR drainage as she desired fertility preservation.
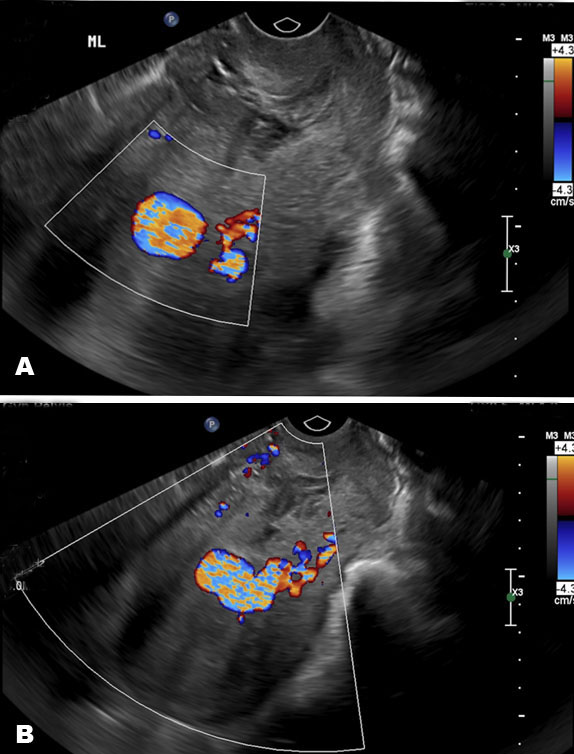
This case report is a follow-up of this patient during her pregnancy three years after treatment of myometrial cysts. She presented at 11 weeks 1 day for a new prenatal visit. In the first and second trimester of her pregnancy she did not report any symptoms to suggest growth of her myometrial cyst. Her first trimester ultrasound did not show any myometrial cysts. Her anatomy scan at 20 weeks was remarkable for a placental lake, the largest measuring 2.26 × 4.55 × 4.02 cm with multiple other smaller 1 × 1 × 1 cm chorionic cysts which were visualized on the fetal aspect of the placenta as shown in Figure 1. The placenta had no signs of a placenta accreta. Due to her complex history, she received a growth ultrasound at 32 weeks which revealed fetal growth restriction (FGR) with an estimated fetal weight (EFW) of 1590g (8th percentile) with normal umbilical artery dopplers. She subsequently started appropriate antenatal testing which continued to be reassuring until term. A growth scan was repeated at 36 weeks with an EFW of 2204 g (5th percentile) and umbilical artery dopplers were again normal. At 38 weeks she underwent scheduled induction of labor for FGR. Her labor course was overall uncomplicated and had an uneventful vaginal delivery of a 6 bs 13.7 oz (3.11 kg) baby boy with Apgars of 5, 9.

Discussion
Overall, this patient had an uncomplicated pregnancy and delivery after repeated IR drainage and sclerosis of large recurrent cystic adenomyomas. This is the first documented case following a patient with history of cystic adenomyomas throughout her pregnancy. The major theorized concerns from the cystic adenomyoma sclerotherapy were that it may result in poor placental perfusion and ultimately in FGR. Another possible concern is that this prior sclerotherapy could result in abnormal placental implantation and vascularization leading to placenta accreta spectrum. Indeed, during her pregnancy, she developed FGR, although fortunately she did not have evidence of placenta accreta. Although this patient had other risks factors for FGR, such as maternal cardiovascular disease and pulmonary disease, there have not been any documented pregnancies after management of cystic adenomyomas so this finding could still play a role in FGR.
Interestingly, there were a number of placental cysts of the fetal surface of the placenta, as shown in Figure 1, which we cannot completely explain solely by the patient’s history and may ultimately be unrelated to her prior cystic adenomas. Subchorionic cysts are associated with FGR via a proposed mechanism that they can cause umbilical cord constriction and compromise fetal blood flow [6],[7]. A case series found that simple cysts <2 cm are not likely of any clinical significance but cyst size>4.5 cm and multiple cysts >3 were associated with growth restriction [8]. Our patient had a large placental lake measuring approximately 4.5 cm which given its size may have contributed to fetal growth restriction and is difficult to tell if this is coincidental or resultant from the cystic adenomyomas. Future case series should be performed to expand the literature for outcomes of pregnancies management of large cystic adenomyomas.
Conclusion
Cystic adenomyomas can cause significant symptoms such as menorrhagia, dysmenorrhea, and pelvic pain. They can be treated with medical management and surgical management such as IR drainage with sclerosis similar to our patient. There are no prior reports of pregnancy after treatment for cystic adenomas, and in our case the pregnancy was complicated by FGR and placental cysts, however the maternal and fetal outcomes were good.
REFERENCES
1.
Brosens I, Gordts S, Habiba M, Benagiano G. Uterine cystic adenomyosis: A disease of younger women. J Pediatr Adolesc Gynecol 2015;28(6):420–6. [CrossRef]
[Pubmed]

2.
Gordts S, Campo R, Brosens I. Hysteroscopic diagnosis and excision of myometrial cystic adenomyosis. Gynecol Surg 2014;11(4):273–8. [CrossRef]
[Pubmed]
3.
Branquinho MM, Marques AL, Leite HB, Silva IS. Juvenile cystic adenomyoma. BMJ Case Rep 2012;2012:bcr2012007006. [CrossRef]
[Pubmed]
4.
Ho ML, Ratts V, Merritt D. Adenomyotic cyst in an adolescent girl. J Pediatr Adolesc Gynecol 2009;22(3):e33–8. [CrossRef]
[Pubmed]
5.
Fuseini NM, Shlansky-Goldberg RD, Neff PM. Ultrasound-guided drainage and sclerosis of a cystic myometrial mass. J Obstet Gynaecol 2017;37(1):127–8. [CrossRef]
[Pubmed]
6.
Thakur S, Jhobta A, Thakur CS. Placental cyst. Applied Radiology 2015;44(9):44.
7.
Brown DL, DiSalvo DN, Frates MC, Davidson KM, Genest DR. Placental surface cysts detected on sonography: Histologic and clinical correlation. J Ultrasound Med 2002;21(6):641–6. [CrossRef]
[Pubmed]
8.
Witters I, Sieprath P, Van Holsbeke C, Theyskens C, Deraedt K. Prenatal diagnosis of multiple large subchorionic placental cysts with intracystic hemorraghe. Facts Views Vis Obgyn 2017;9(4):223–5.
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
Thank you to residents and staff of Hospital of University of Pennsylvania for taking excellent care of this patient.
Author ContributionsJordann-Mishael Duncan - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Matthew Janssen - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Richard Shlansky-Goldberg - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Adi Hirshberg - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Pamela Neff - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Jordann-Mishael Duncan et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}