 |
Case Series
Tubal abortion case series: Important clinical findings found on diagnostic laparoscopy may preserve tubal function and future fertility
1 Ob/Gyn Faculty, Honor Health System, 19829 N 27th Ave, Phoenix, AZ 85027, USA
2 Ob/Gyn Faculty, Lincoln Hospital and Mental Health Center, 249 E 149th St., Bronx, NY 10451, USA
Address correspondence to:
Alexander Sabre
M.D., Honor Health System, 19829 N 27th Ave, Phoenix, AZ 85027,
USA
Message to Corresponding Author
Article ID: 100110Z08AS2022
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Sabre A, Arul M. Tubal abortion case series: Important clinical findings found on diagnostic laparoscopy may preserve tubal function and future fertility. J Case Rep Images Obstet Gynecol 2022;8:100110Z08AS2022.ABSTRACT
Introduction: Tubal abortion is characterized by the extrusion of an ectopic pregnancy initially implanted in the fallopian tube through the fimbriated ostium into the peritoneal cavity. It may present as either complete or incomplete expulsion, may lead to severe bleeding, or present with less acute findings which nevertheless requires surgical evaluation. Recognition of a complete tubal abortion through surgical evaluation may be challenging but is essential because it allows conservative management which allow preservation of tubal function and fertility without disrupting tubal anatomy or function.
Case Series: We present a case series of surgical evaluation and management of tubal abortion, with the first case which demonstrated complete tubal abortion and subsequent implantation into the omentum which required surgical dissection. The second case demonstrates acute complete tubal abortion in an asymptomatic patient, who underwent diagnostic laparoscopy revealing the subsequent pathology.
Conclusion: This case series highlights other findings in literature, that conservative surgical management entailing evacuation of products of conception and blood clots to prevent chronic pain and further adhesion formation is sufficient management of complete tubal abortion. This approach ensures preservation of tubal anatomy and allows patients an opportunity for future fertility.
Keywords: Case series, Ectopic pregnancy, Tubal abortion
Introduction
The incidence of ectopic pregnancy is approximately 20 in 1000 pregnancies [1]. The most common location for an ectopic pregnancy is in the fallopian tubes (95%) specifically in the ampullary portion, but other less common areas are ovarian, abdominal, cervical, and cesarean scar locations [2].
Tubal abortion is important to recognize because it may be appropriately managed with conservative intraoperative techniques. Surgical interventions for tubal gestations consist of either salpingectomy or salpingostomy, these techniques either disrupt the structure and function of the fallopian tube, or form adhesions further disrupting the architecture of the pelvic organs. Because of the concern about future fertility, in the appropriate patient with tubal abortion and intact adnexal structures, conservative management is the mainstay of treatment [3].
We present a case series of two encounters of complete tubal abortion diagnosed by laparoscopic findings, histological evidence, and that both were managed in conservative surgical manner that preserved tubal anatomy.
Case Series
Case 1
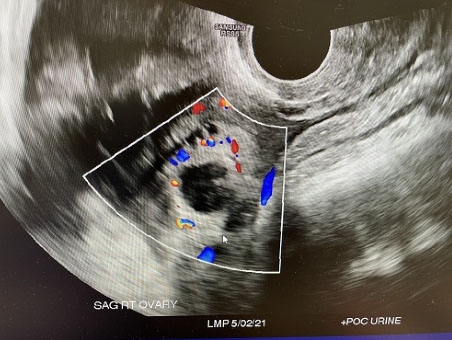
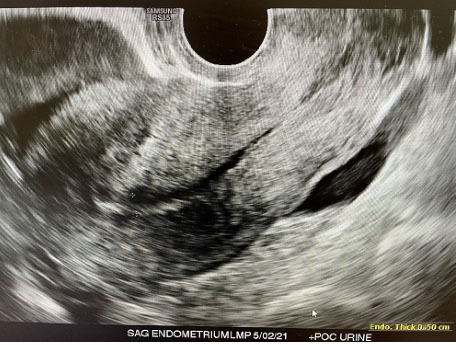
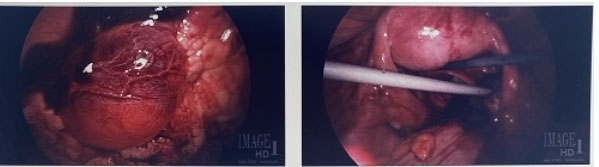
A 25-year-old gravida 1, para 0 at 5 weeks+0 day by last menstrual period (LMP) initially presented to emergency room with worsening lower abdominal pain for two days. No significant past medical history. Physical exam revealed guarding and generalized abdominal pain and rebound. At that time, patient vitals were unremarkable, Temperature: 98°F, blood pressure (BP): 106/67 mmHg, pulse rate: 88 bpm, respiratory rate (RR): 18 breaths per minute, SpO2: 100% on room air (RA). Laboratory evaluation revealed the patient had a positive β-hCG 1444 mIU/mL and hemoglobin/hematocrit of 12.0 g/dL/38.0%. Pelvic ultrasound (US) revealed no intrauterine pregnancy and thick walled right adnexal ring measuring 2.6 cm with low level internal echos, and moderate amount of complex pelvic fluid (Figure 1 and Figure 2). The patient was taken to operating room which revealed extensive hemoperitoneum of 800 mL of blood and clots, normal uterus and intact bilateral fallopian tubes, and a 2 cm vascular cystic gestational sac-like structure which was attached to omentum and to fimbria of right fallopian tube, that was mixed with clots (Figure 3). Intraoperative general surgery consult was called due to proximity to bowel, it was noted that the gestational sac and omentum were free of bowel, a transection and wedge resection was performed on the affected area. The specimen was sent for pathological evaluation revealing the presence of focal trophoblasts and chorionic villi (Figure 4). The patient serum hCG was followed outpatient till negative.
Case 2
A 19-year-old gravida 1, para 0 at 4 weeks 0 days by LMP (although exact dating was difficult to ascertain due to recent use of oral contraceptive pills and spotting episodes), presented to emergency department with vaginal bleeding and severe abdominal pain which occurred less than twelve hours prior. The pain has been constant but less severe upon presentation in ER. Past GYN history was significant for three sexual partners, one which was sexual assault three months prior which the patient did not seek medical evaluation for, and was also significant for tobacco smoking. Patient vital signs were within normal range: Temp: 98°F, BP 138/82 mmHg, pulse rate: 86 bpm, RR: 18 breaths per minute, SpO2: 100% on RA. Abdominal exam was essentially benign, pain was only elicited on pelvic exam on palpation of pouch of Douglas.
Labs revealed hCG of: 436 mIU/mL, hemoglobin/hematocrit of 13.0 g/dL/39.3% and US revealed no gestational sac, moderate free fluid in pelvis, and a nonvascular 4.7×0.9×3.2 cm structure in left adnexa (Figure 5). Concern was for ruptured ectopic pregnancy and patient brought to OR underwent diagnostic laparoscopy with findings of extensive adhesions consistent with Fitz-Hugh-Curtis syndrome, normal uterus bilateral ovaries and right fallopian tube, extensive hemoperitoneum of 350 mL, mildly dilated but intact left fallopian tube, and behind the left ovary adhered to the fimbria and the pelvic side wall in the pouch of Douglas was a blood clot and what appeared to be products of conception (Figure 6 and Figure 7). This was evacuated and sent for pathological evaluation, which revealed chorionic villi confirming ectopic pregnancy from the specimen obtained. Patient was followed up in clinic 10 days later with serum hCG negative.




Discussion
The classical symptom associated with tubal pregnancy is lower abdominal pain due to tubal distention, associated with tubal contractions and thus colicky pain. If the process continues the gestational products may be expressed into the peritoneal cavity, resulting in tubal abortion. Sherman et al. have noted that patients typically present with severe pain and acute signs of peritoneal irritation being noted on physical examination [3].
The progression of tubal ectopic pregnancy may include rupture of the fallopian tube causing massive hemoperitoneum, or may result in tubal contractions resulting in spontaneous expulsion from the abdominal ostium, embryonic demise and involution of the conceptus [4]. Rarely, the expulsion of the embryo may secondarily implant within the peritoneal cavity. This is different from primary abdominal pregnancy, which do not demonstrate Studdiford’s criteria of normal ovaries and fallopian tubes, no evidence of uteroperitoneal fistula, pregnancy primary location in the serosal peritoneal surface, and no evidence of secondary implantation following initial primary tubal expulsion [5]. In case #1, because of the presence of fibrin and blood clots from the right fallopian tube surrounding the gestational sac imbedded in omentum, this confirms a complete tubal abortion with subsequent peritoneal implantation.
There is no characteristic pain in ectopic pregnancy, but certain features such as peritoneal irritation and guarding are indicative of intraperitoneal process. On physical exam, cervical motion tenderness and palpable adnexal mass are frequently present [6]. This was present in case #2, as the patient did not present with peritoneal signs elicited on abdominal examination, but on bimanual examination of posterior cul de sac, pain was elicited. Because of the nature of peritoneal irritation, tubal abortion can mimic other causes of abdominal pain. Aryal et al. presented a case of suspected acute appendicitis, with initial negative urine pregnancy test, that upon laparoscopic intervention reveal a tubal abortion located in right iliac fossa [7].
Diagnosis is critical for both management and patient counseling. Ectopic pregnancy is also an important cause of morbidity and a high percentage of the affected patients may become infertile [8]. A complete tubal abortion is an important diagnostic consideration, allowing for conservative management performed during laparoscopy. This may preserve tubal function and future fertility, while also avoiding the use of the chemotherapy agent, methotrexate.
Suspected cases of ectopic pregnancies that do not meet criteria for medical management with methotrexate require surgical exploration [9]. Tubal abortion can only be confirmed with direct visualization of products of conception outside of the fallopian tube, allow for conservative manipulation of the pelvic organs to decreased disruption of structure and function, and thus remains an important differential diagnosis made by gynecologists in the surgical approach to ectopic pregnancy.
Conclusion
This case series highlights other findings in literature, that conservative surgical management entailing evacuation of products of conception and blood clots to prevent chronic pain and further adhesion formation is sufficient management of complete tubal abortion. This approach ensures preservation of tubal anatomy and allows patients an opportunity for future fertility.
REFERENCES
1.
Sebire NJ, Lindsay I, Fisher RA, Savage P, Seckl MJ. Overdiagnosis of complete and partial hydatidiform mole in tubal ectopic pregnancies. Int J Gynecol Pathol 2005;24(3):260–4. [CrossRef]
[Pubmed]

2.
Hoffman BL, Schorge JO, Schaffer JI, Halvorson LM, Bradshaw KD, Cunningham GF. Ectopic Pregnancy. Williams Gynecology. 2ed. New York: McGraw Hill; 2008. p. 198–215.
3.
Caspi E, Sherman D. Tubal abortion and infundibular ectopic pregnancy. Clin Obstet Gynecol 1987;30(1):155–63. [CrossRef]
[Pubmed]
4.
Chirculescu B, Chirculescu R, Ionescu M, Peltecu G, Panaitescu A. Complete tubal abortion: A rare form of ectopic pregnancy. Chirurgia (Bucur) 2017;112(1):68–71. [CrossRef]
[Pubmed]
5.
Poole A, Haas D, Magann EF. Early abdominal ectopic pregnancies: A systematic review of the literature. Gynecol Obstet Invest 2012;74(4):249–60. [CrossRef]
[Pubmed]
6.
Alkatout I, Honemeyer U, Strauss A, et al. Clinical diagnosis and treatment of ectopic pregnancy. Obstet Gynecol Surv 2013;68(8):571–81. [CrossRef]
[Pubmed]
7.
Aryal S, Shrestha BM, Lamsal S, Regmi M, Karki A, Katuwal N. Tubal abortion masquerading as an acute appendicitis with a negative urine pregnancy test: A case report. Int J Surg Case Rep 2021;87:106438. [CrossRef]
[Pubmed]
8.
Elito JJ. Clinical treatment of unruptured ectopic pregnancy. Ectopic Pregnancy – Modern Diagnosis and Management. London: IntechOpen Limited; 2011. p. 177–201. [CrossRef]
9.
American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Gynecology. ACOG practice bulletin No. 193: Tubal ectopic pregnancy. Obstet Gynecol 2018;131(3):e91–103. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
We wish to thank all the first line responders and healthcare workers who tirelessly fight for patients in the COVID-19 pandemic.
Author ContributionsAlexander Sabre - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Manonmani Arul - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2022 Alexander Sabre et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}