 |
Case Report
Dilation and evacuation with intrauterine device placement in a patient with acute promyelocytic leukemia: A case report
1 Department of Obstetrics and Gynecology, Hackensack University Medical Center, Hackensack, NJ, USA
2 Hackensack Meridian School of Medicine, Hackensack Meridian Health Network, Nutley, NJ, USA
Address correspondence to:
Kelsey McClure
DO, Department of Ob/Gyn, Hackensack University Medical Center, 20 Prospect Avenue, Suite #805, Hackensack, NJ 07601,
USA
Message to Corresponding Author
Article ID: 100143Z08KM2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
McClure K, Benerofe S, Budge KL, Francis AP, Figueroa M. Dilation and evacuation with intrauterine device placement in a patient with acute promyelocytic leukemia: A case report. J Case Rep Images Obstet Gynecol 2023;9(1):40–43.ABSTRACT
Introduction: Pregnant leukemia patients should be offered continuation or termination of pregnancy. Treatment of leukemia in reproductive-age patients includes consideration of contraception. Hormonal intrauterine devices (IUDs) prevent pregnancy and decrease menstrual bleeding. Despite safety data for IUDs in immunocompromised patients, infection and vaginal bleeding concerns may inhibit their placement.
Case Report: We report a case of a 28-year-old female at 13 weeks 4 days gestation with acute promyelocytic leukemia (APL) who presented with coagulopathy. When stabilized, dilation and evacuation (D&E) with levonorgestrel IUD placement was performed. The postoperative course was uncomplicated. Despite chemotherapy and neutropenia, this APL patient tolerated D&E with levonorgestrel IUD placement well with only routine preoperative antibiotics.
Conclusion: Comprehensive options counseling for pregnant patients with new APL diagnoses are imperative, and interdisciplinary consideration of risks for individual patient concerns of pregnancy prevention during treatment with teratogenic potential, avoidance of combined hormonal contraception (CHC) coagulopathy risk, and menstrual bleeding reduction in the setting of pancytopenia with levonorgestrel IUD contraception management in immunocompromised patients may be considered.
Keywords: Acute promyelocytic leukemia, Case report, Contraception, Immunocompromised, Levonorgestrel IUD
Introduction
Acute promyelocytic leukemia is a subtype of acute myeloid leukemia characterized by a balanced translocation generating the fusion gene promyelocytic leukemia/retinoic acid receptor alpha (PML-RARA). Promyelocytic leukemia/retinoic acid receptor alpha has sensitivity to all-trans-retinoic acid (ATRA) and arsenic trioxide (ATO) with cure rates around 90% [1]. Acute promyelocytic leukemia therapy may have teratogenic effects, but delay of therapy can worsen a patient’s prognosis. Increased risk of abortion and preterm delivery are noted [2], and APL therapy in pregnancy is associated with a high risk of medical and obstetrical complications [3]. Treatment can cause pancytopenia, creating susceptibility to bleeding and infection [2]. Dilation and evacuation has low complication rates; however, limited data exist to guide the treatment of APL patients desiring interruption of pregnancy. Levonorgestrel IUDs (LNG-IUD) are highly effective contraceptives that can decrease menstrual blood loss without increasing thrombotic risk. Studies exploring hormonal IUD use in other immunocompromised populations such as human immunodeficiency virus (HIV) [4] and lupus [5] patients have supported their safety. We reviewed a patient with APL on ATRA-ATO and hydroxyurea who underwent D&E with LNG-IUD placement. Further studies are needed to explore the safety of D&E with IUD placement for APL patients.
Case Report
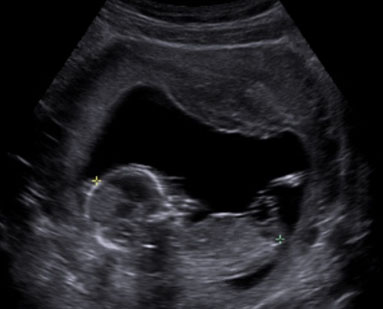
A 28-year-old gravida 1 at 13 weeks 4 days gestation (Figure 1) presented for treatment of newly diagnosed APL. The patient had one normal prenatal visit in the first trimester. A few weeks later, the patient noted new-onset headache, gingival bleeding, bruising, vomiting, and epistaxis, prompting presentation to an emre3gency room (ER) where the patient’s white blood cell count (WBC) was 140 × 103 and fibrinogen nadir was 63 mg/dL. The patient was transferred to our institution for presumed disseminated intravascular coagulopathy (DIC) and was then diagnosed with APL on peripheral blood smear. Hematology/oncology recommended treatment with ATRA-ATO and hydroxyurea. Coagulopathy was monitored closely and managed with fresh frozen plasma and platelet transfusions with goal fibrinogen greater than 150 mg/dL and platelet count greater than 50 per µL. After maternal fetal medicine (MFM) consultation, the patient decided to proceed with chemotherapy and termination of pregnancy once coagulopathy improved. Family planning consultation was performed on HD2 with recommendation for surgical termination with cervical preparation to reduce the risk of bleeding and infection. Recommendation against restarting the patient’s previous combined hormonal contraception post-abortion was made. The patient strongly desired fertility post-treatment, progesterone-only, and non-hormonal contraceptives were reviewed, and the patient opted for postabortal LNG-IUD placement.
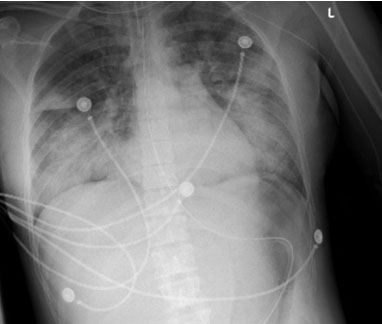
On HD3 chemotherapy was initiated and the patient developed acute respiratory distress (ARDS), requiring intubation and admission to the intensive care unit (ICU) (Figure 2). On HD5 she improved, was extubated, and discharged from the ICU. She continued routine APL treatment with antimicrobial prophylaxis. On HD13 her coagulopathy reversed and she was surgically cleared for termination of pregnancy with hemoglobin levels greater than 8 g/dL and platelets greater than 80,000 per µL. On HD14 the patient received mifepristone 200 mg orally once. On HD15 she received 600 mcg misoprostol buccal 2 hours prior to surgery. Dilation and evacuation was performed under ultrasound guidance. Paracervical injection of four units of vasopressin in 20 cc normal saline was performed at the start of the procedure. The estimated blood loss was 200 mL and no uterotonics were required. The patient received Doxycycline for preoperative prophylaxis and a gonorrhea/chlamydia swab was negative. Levonorgestrel IUD was placed under ultrasound guidance. Immediate and 2-week postoperative checks were unremarkable, and the patient continued with her APL treatment. The patient was contacted six months postoperatively and remained without complications.
Discussion
This case is an example of newly diagnosed APL on ATRA-ATO and hydroxyurea, complicated by coagulopathy, differentiation syndrome, and neutropenia, that underwent uncomplicated D&E with LNG-IUD placement. The dysfunctionality of the coagulation system is a common complication of APL that poses an increased risk of early mortality by hemorrhage or thrombosis. Coagulopathy for this patient was likely due to underlying leukemia, differentiation syndrome, and/or concomitant chemotherapy increasing the risk for the development of ARDS. The surgery took place after coagulopathy was reversed and differentiation syndrome had improved; however, the patient was still neutropenic at the time. During the postoperative course, the patient showed no signs of pelvic infection or heavy vaginal bleeding.
Dilation and evacuation procedures have low complication rates; however, rarity of APL in pregnancy limits guidance of treatment in patients choosing interruption of pregnancy. Counseling using shared decision-making models with patient, OB-GYN, and other involved subspecialists included recommendations for D&E versus medical termination to reduce the risk of retained products, bleeding, and infection. In this setting of high risk of bleeding, thrombosis, and unintended pregnancy, the benefits of levonorgestrel-IUD were determined by the patient and her providers to have benefits that outweighed risks of placement. Surgical termination was efficient and safe, allowing minimal interruption of APL treatment.
There has been hesitancy with the placement of IUDs in immunocompromised women due to fear of infection, but data suggest that the IUD is a practical option [6]. Levonorgestrel IUDs are highly effective contraception advisable in cases of treatment with teratogenic potential. Menstrual bleeding reduction can be beneficial in the setting of treatment-induced pancytopenia. Increased continuation of highly effective reversible contraceptive methods with postabortal placement [7] and avoidance of CHC coagulopathy risk is favorable in this high-risk population. Further studies are needed to support the safety of D&E with IUD placement in APL patients undergoing treatment.
Conclusion
Hemorrhagic and thrombotic complications are the most common cause of mortality in patients with APL due to distinct coagulopathy stemming from hyperfibrinolysis. Pancytopenia may exacerbate menstrual bleeding and abnormal uterine bleeding. These patients may benefit from LNG-IUD placement, which provides reduction of menstrual blood loss, highly effective contraception while receiving potentially teratogenic treatments, and unintended pregnancy-related thrombosis. Theoretical concerns for IUD placement in immunocompromised patients include an increased risk of infection and clotting. This case report presents D&E and LNG-IUD placement with routine infection screening and prophylaxis in a patient with newly diagnosed APL without complications after six months of follow-up. Counseling considerations for this patient included pregnancy prevention during treatment with teratogenic potential, avoidance of combined hormonal contraception (CHC) due to coagulopathy risk, and menstrual bleeding reduction in the setting of pancytopenia. We advocate for comprehensive contraception counseling including LNG-IUD placement and shared decision-making for patients at high risk for unintended pregnancy seeking highly effective contraception.
REFERENCES
1.
Sanz MA, Fenaux P, Tallman MS, et al. Management of acute promyelocytic leukemia: Updated recommendations from an expert panel of the European LeukemiaNet. Blood 2019;133(15):1630–43. [CrossRef]
[Pubmed]

2.
Santolaria A, Perales A, Montesinos P, Sanz MA. Acute promyelocytic leukemia during pregnancy: A systematic review of the literature. Cancers (Basel) 2020;12(4):968. [CrossRef]
[Pubmed]
3.
Verma V, Giri S, Manandhar S, Pathak R, Bhatt VR. Acute promyelocytic leukemia during pregnancy: A systematic analysis of outcome. Leuk Lymphoma 2016;57(3):616–22. [CrossRef]
[Pubmed]
4.
Morrison CS, Sekadde-Kigondu C, Sinei SK, Weiner DH, Kwok C, Kokonya D. Is the intrauterine device appropriate contraception for HIV-1-infected women? BJOG 2001;108(8):784–90. [CrossRef]
[Pubmed]
5.
Sánchez-Guerrero J, Uribe AG, Jiménez-Santana L, et al. A trial of contraceptive methods in women with systemic lupus erythematosus. N Engl J Med 2005;353(24):2539–49. [CrossRef]
[Pubmed]
6.
Browne H, Manipalviratn S, Armstrong A. Using an intrauterine device in immunocompromised women. Obstet Gynecol 2008;112(3):667–9. [CrossRef]
[Pubmed]
7.
Okusanya BO, Oduwole O, Effa EE. Immediate postabortal insertion of intrauterine devices. Cochrane Database Syst Rev 2014;2014(7):CD001777. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Kelsey McClure - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sara Benerofe - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kelly L Budge - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Antonia P Francis - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Melissa Figueroa - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Kelsey McClure et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}