 |
Case Report
Severe affection of the obturator nerve in a young patient after tension free vaginal sling placement: Case report of a rare complication and review of the literature
1 Consultant, Department of Ob/Gyn, APK Clinics, Wiesbaden, Germany
2 Head of Department, Department of Ob/Gyn, St. Josefs-Hospital, Wiesbaden, Germany
Address correspondence to:
Vera Joser
Asklepios Paulinen Klinik, Geisenheimer Straße 10, 65197 Wiesbaden,
Germany
Message to Corresponding Author
Article ID: 100146Z08VJ2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Joser V, Gabriel B. Severe affection of the obturator nerve in a young patient after tension free vaginal sling placement: Case report of a rare complication and review of the literature. J Case Rep Images Obstet Gynecol 2023;9(1):53–58.ABSTRACT
Introduction: Stress urinary incontinence affects up to 50% of women at some point in their lives. Tension-free vaginal mid-urethral sling procedure should be offered as a primary surgical treatment option to women with stress urinary incontinence.
Case Report: We report on the case of a 47-year-old patient presenting with heavy buttock and thigh pain, a severe walking disability necessitating the use of a walker after implantation of a retropubic sub-urethral sling (TVT-SERASIS) for the treatment of stress urinary incontinence in an external hospital. During the surgery in our hospital, it was revealed that the sling was placed incorrectly, charging the bladder wall as well as the left obturator nerve. We describe the diagnosis and operative management of this rare, but serious complication.
Conclusion: Our case provides supporting evidence for the limited value of imaging tools and the need of a surgical exploration under certain circumstances. In addition, we emphasize that removal of a sub-urethral sling should be performed under laparoscopic visualization when serious adverse events occur. Sub-urethral sling placement should be executed by experienced, dedicated pelvic floor surgeons.
Keywords: Complications, Mid-urethral sling (MUS), Obturator nerve injury, Stress urinary incontinence
Introduction
Stress urinary incontinence is the “complaint of involuntary urine leakage on effort or exertion, or on sneezing or coughing” [1], affects up to 50% of women at some point in their lives [2]. The quality of life of those affected is considerably reduced. Pelvic floor muscle exercise is the main conservative treatment for urinary incontinence. Tension-free vaginal mid-urethral sling procedure should be offered as a primary surgical treatment option to women with stress urinary incontinence according to the German Guidelines [3]. They have been rapidly adopted in the primary treatment of urinary stress incontinence because of their effectiveness, low invasiveness, and rapid postoperative recovery of the patient. Nevertheless, the surgery carries risks and dangers, so that this treatment should be well considered.
Case Report
A 47-year-old patient was referred to our pelvic floor center for further diagnosis and treatment. A retropubic sub-urethral sling (TVT-SERASIS) was placed in an external hospital 14 days ago for the treatment of stress urinary incontinence. The patient presented herself with a heavy walking disability using a walker. Since surgery, the patient complained of severe groin, buttock, and thigh pain on the left side with the inability of external hip rotation. In addition, the patient could neither adequately stand up nor urinate in a sitting position after pelvic tilt. The patient’s medical history was completely uneventful. She gave birth to two children spontaneously.
It was not possible to assess whether the sling was effective because the patient was unable to comment on her postoperative urinary function due to the severe pain and embarrassment. There were no sensory deficits according to the neurological examination. A residual urine-free micturition (while standing) was possible. There were neither increased inflammation values nor fever. A computer tomography (CT) scan performed in the external hospital as well as an ultrasound examination were inconclusive. Infiltration of local anesthetics and cortisone did not provide any significant pain relief. The patient was offered subsequently a physiotherapy and pain medication was prescribed.
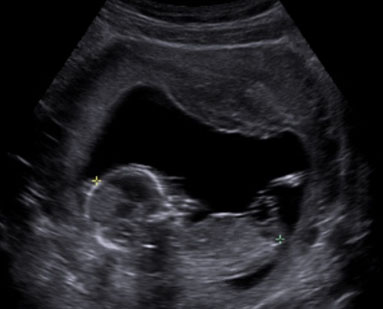
On physical examination in our hospital, the abdomen was soft. Speculum examination revealed no evidence of vaginal erosion, and the vaginal as well as the skin incisions healed without abnormality. Bimanual examination revealed an induration at the left edge of the symphysis. The groins were unsuspicious, but there was a significant hardening in the left groin with pain radiance into the left thigh. In addition, a superficial hematoma could be seen on the left side, due to local infiltration of Hydrocortisone and Mepivacaine a few days ago. Importantly, the exit points on the skin of the sub-urethral sling appeared to be located too far from each other and too close to the left groin indicating a potential incorrect placement of the sling. Introital ultrasound examination showed the sling lying symmetrically with a 4 mm distance from the urethra (Figure 1). In addition, a 12×8 mm highly echogenic area supported our assumption of a potential torsion of the sling course on the left side. There was no evidence of hematoma in the Retzius space. Bladder and both kidneys were unremarkable. For further diagnosis, a magnet resonance imaging (MRI) of the pelvis was performed without indicative findings. An orthopedic colleague was consulted and ruled out a bone or muscular lesion. In addition, a neurological colleague was consulted and confirmed the suspected obturator nerve injury on the left side.
Based on our clinical findings an incorrect sling course with obturator nerve affection was suspected and a laparoscopic surgical exploration of the Retzius space with tape removal was planned.
We started with a diagnostic cystoscopy to exclude an arosion of the sling into the urinary bladder or urethra. The left bladder wall appeared warped without any sling arosion and unsuspicious mucosa. Subsequently, a laparoscopy was performed to evaluate the intra-abdominal situation which was normal. Then, the Retzius space was entered laparoscopically after transecting the Urachus and the pre-vesical space was visualized to explore the position of the sling.
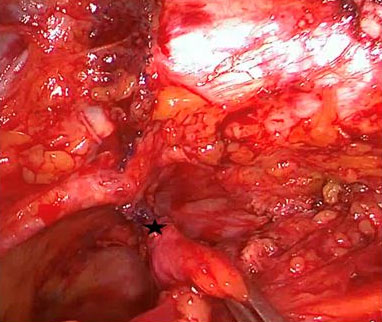
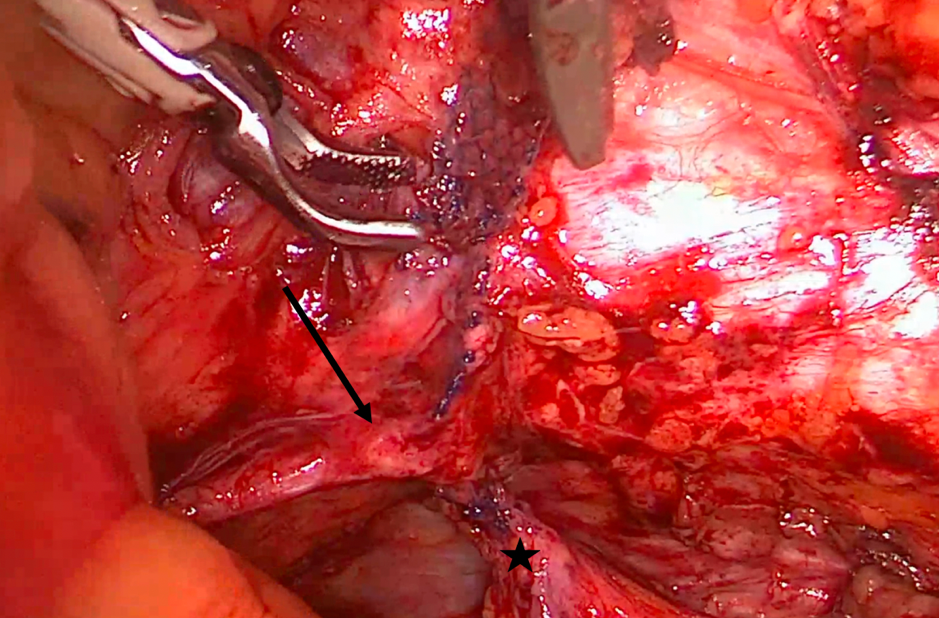
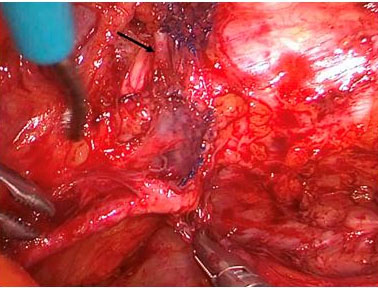
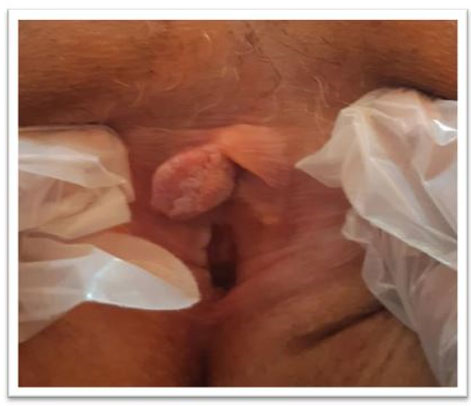
On the right side, the sling appeared to be located too laterally without any affection of neighboring structures or organs. On the left side, the bladder wall was pulled upward toward the obturator foramen and the internal border of the pubic ramus by the sling being placed incorrectly (Figure 2). The obturator nerve was loaded by the sling, just before entering the obturator foramen and pulled upward (Figure 3). More cranially, the sling was found to be virtually directly adjacent to the external iliac vein, which was visualized posteriorly, dissected, and freed. During this dissection procedure it became evident that the corona mortis vessel branch was situated as well directly posterior to the sling (Figure 4). Fortunately, no blood vessels were injured during the insertion of the sling.
After thorough inspection, the left obturator nerve was found to be affected and displaced cranially by the sling, but it did not appear to have been torn off and subsequently pulled back into the obturator foramen. The external iliac vessel, the corona mortis, as well as the nerve were thoroughly freed from the sling which was subsequently carefully mobilized. The obturator nerve was completely dissected and exposed. The sling was completely sticked on these structures, especially on the nerve and all procedures had to be performed very gently, without too much tension.
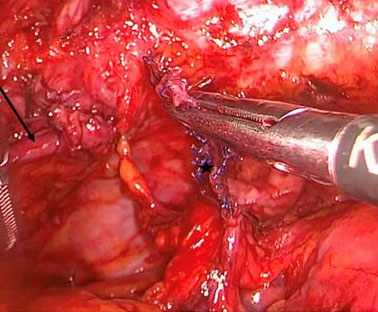
Thus, further dissection and exposure had to be performed here so that the sling could be cut and the cranial portion extracted separately. The nerve and artery were freed and moved freely into the foramen. The nerve, which had been displaced cranially, immediately slipped back into its original position. Finally, the caudal portion of the sling was removed vaginally after using the old vaginal incision and using controlled pulling forces and under laparoscopic view (Figure 5). After surgery the patient immediately reported of full pain relief. The patient could be mobilized in a timely manner and, under physiotherapeutic guidance, stepping and external rotation of the hip were possible again without restrictions.
Four days after surgery, the patient could be discharged from inpatient treatment. Physiotherapeutic care continued on an outpatient basis. Unfortunately, however, the previously known stress incontinence recurred. The patient currently refuses a new sub-urethral sling implantation to treat her urinary leakage again.

Discussion
The NICE (National Institute for Health and Clinical Excellence) Clinical Guideline 2019 recommends the use of Synthetic Macroporous Type I Slings for the treatment of female stress incontinence [4]. Two main approaches of sling placement have been developed: the retropubic and the transobturator, which are comparable regarding subjective and objective success rates. However, the longest data history is only available for the retropubic approach (17 years), and the long-term success rates (8 years and more) seem to be in favor of this approach. Moreover, in patients with risk factors such as intrinsic urethral sphincter deficiency, mixed incontinence, or obesity, the retropubic approach is more successful compared to the transobturator one. In addition, the probability of re-surgery after primary sling placement is higher after a transobturator approach. The perioperative risks of both approaches are low; however, the transobturator approach was found to bear a higher risk of vaginal perforations and sling palpability. Based on these data, urogynecologists prefer to use the retropubic approach to treat younger patients.
Mid-urethral retropubic sling approaches have higher perioperative morbidity compared with the transobturator ones, though the overall rate of adverse events remained low [2].
The retropubic sling insertion is more frequently associated with bladder injury, retropubic hematoma, bladder voiding dysfunction, and lower urinary tract symptoms than the transobturator insertion [5],[6]. However, inner thigh and groin pain and vaginal sulci injuries are more common after transobturator implantation insertion [7],[8],[9],[10].
Injuries to the iliac, obturator, or epigastric vessels associated with retropubic sling implantation have been reported [11],[12]. Although rare, they are more common compared to the transobturator approach [2]. In the German-Austrian-Swiss guideline, the risk of a severe vascular complication is reported to be “very low” [3].
In our case, the sling was placed directly adjacent to the main blood vessels, i.e., the external iliac vein and the corona mortis, being an anastomosis between the obturator and the external iliac veins. It was located behind the superior pubic ramus at a variable distance from the symphysis. Fortunately, these vessels were not injured during primary surgery requiring emergency laparotomy. The big advantage of laparoscopic assisted surgery is the visualization of every important structure before vaginal removal of the dystopic sling. If we would have not performed a laparoscopy in our case, the patient would have been exposed to a non-negligible risk of injury the aforementioned vessels as well as tearing of the obturator nerve close to the obturator foramen, which would have made repair impossible or at least very difficult.
Neurologic complications due to obturator nerve injury after retropubic sling insertion are very rare. The less experienced surgeon may be tempted to use a more lateral way being afraid to injure the bladder. In our case we suspected that this may have been the case because the skin incisions, especially on the left side, as described before, were placed too far laterally towards the groin.
It is recommended that the tip of the surgical instrument—while passing the Retzius space—has always to be in close contact with the backside of the symphysis to avoid serious complication such as intra-abdominal entry (with potential bowel perforation) or lateral damage of big vessels or, as in our case, the obturator nerve.
It must be emphasized that concerns regarding bladder injury are justified but this should not lead to lateral deviation and surgeons should always be aware of the rare, but serious complications that may occur when leaving the “safe region” of the symphysis back wall. In addition, there are some precautions to prevent bladder injury, while placing the sling such as bladder emptying and deviation to the contralateral side. In our case, the bladder was affected together with the obturator nerve on the left side, which reflects an incorrect insertion. Also, we would like to emphasize that such complications are never due to the alloplastic material itself.
Conclusion
Obturator nerve injuries and other serious complications are rare, but more probable after transobturator placement of sub-urethral slings. Our patient was unable to stand up after the sling insertion which is not “normal” for a patient after such a “small surgery.” The pure clinical view as well as ultrasound can be helpful in the diagnosis and a prompt surgical exploration is necessary in such cases as MRI and CT scans are of limited value. A prompt clinical diagnosis and early loosening and removal of the sling would certainly have been easier—two weeks after implantation the sling was already well integrated into the surrounding tissue—however, much more damage could have been caused by a “blind” vaginal traction, so that a stepwise surgical procedure under laparoscopic control, as described above, appears to be of great benefit and protects the patients from secondary harms. The procedure of mid-urethral sling placement should be executed by experienced and specialized pelvic floor surgeons or at least be performed under supervision of experienced ones. Differentiated information of the patient, also about alternative treatments and their risks, is required.
REFERENCES
1.
Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology in lower urinary tract function: Report from the standardisation sub-committee of the International Continence Society. Urology 2003;61(1):37–49. [CrossRef]
[Pubmed]

2.
Ford AA, Rogerson L, Cody JD, Aluko P, Ogah JA. Mid-urethral sling operations for stress urinary incontinence in women. Cochrane Database Syst Rev 2017;7(7):CD006375. [CrossRef]
[Pubmed]
3.
AWMF: Leitlinien. In: Harninkontinenz der Frau. [Available at: https://register.awmf.org/assets/guidelines/015-091l_S2k_Harninkontinenz-der-Frau_2022-03.pdf]
4.
Urinary incontinence and pelvic organ proplapse in women: Management. NICE (National Institute for Health and Clinical Excellence) guideline. 2 April 2019. [Availabe at: https://www.nice.org.uk/guidance/ng123/resources/urinary-incontinence-and-pelvic-organ-prolapse-in-women-management-pdf-66141657205189]
5.
Novara G, Galfano A, Boscolo-Berto R, et al. Complication rates of tension-free midurethral slings in the treatment of female stress urinary incontinence: A systematic review and meta-analysis of randomized controlled trials comparing tension-free midurethral tapes to other surgical procedures and different devices. Eur Urol 2008;53(2):288–308. [CrossRef]
[Pubmed]
6.
Tommaselli GA, Di Carlo C, Formisano C, Fabozzi A, Nappi C. Medium-term and long-term outcomes following placement of midurethral slings for stress urinary incontinence: A systematic review and metaanalysis. Int Urogynecol J 2015;26(9):1253–68. [CrossRef]
[Pubmed]
7.
Latthe PM, Singh P, Foon R, Toozs-Hobson P. Two routes of transobturator tape procedures in stress urinary incontinence: A meta-analysis with direct and indirect comparison of randomized trials. BJU Int 2010;106(1):68–76. [CrossRef]
[Pubmed]
8.
Petri E, Ashok K. Comparison of late complications of retropubic and transobturator slings in stress urinary incontinence. Int Urogynecol J 2012;23(3):321–5. [CrossRef]
[Pubmed]
9.
Thomas TN, Siff LN, Jelovsek JE, Barber M. Surgical pain after transobturator and retropubic midurethral sling placement. Obstet Gynecol 2017;130(1):118–25.
[Pubmed]
10.
Elers J, Hornum Bing M, Birkefoss K, Rohde JF, Ussing A, Glavind K. TVT or TVT-O? – A systematic review and meta-analysis comparing efficacy, complications and re-operations. Eur J Obstet Gynecol Reprod Biol 2021;258:146–51. [CrossRef]
[Pubmed]
11.
Sivanesan K, Abdel-Fattah M, Ghani R. External iliac artery injury during insertion of tension-free vaginal tape: A case report and literature review. Int Urogynecol J Pelvic Floor Dysfunct 2007;18(9):1105–8. [CrossRef]
[Pubmed]
12.
Parikh NN, Spinner RJ, Tollefson MK, Linder BJ. An unusual complication of retropubic midurethral sling placement: Obturator neuralgia. Urology 2021;156:e96–8. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Vera Joser - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Boris Gabriel - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Vera Joser et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}