 |
Case Report
Case of retained fetal femur acting as inert intrauterine device
1 Medical Student, School of Medicine, University of Washington, Seattle, WA, USA
2 MD, PhD, Physician, Seattle Reproductive Medicine, Spokane, WA, USA
3 MD, MS, Physician, Seattle Reproductive Medicine, Seattle, WA, USA
Address correspondence to:
Brooke Barton
4311 S Pinegrove Ln, Spokane, WA,
USA
Message to Corresponding Author
Article ID: 100147Z08BB2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Barton B, Every E, Houmard B, Davis L. Case of retained fetal femur acting as inert intrauterine device. J Case Rep Images Obstet Gynecol 2023;9(1):59–62.ABSTRACT
Introduction: Retention of fetal bones is a rare but documented complication after dilation and curettage (D&C). Previous case reports have described instances of retention of multiple fetal bones or bony fragments.
Case Report: We are presenting a case of a female with 1.5 years of secondary infertility due to retention of a single, intact, fetal femur bone following a therapeutic abortion 13 years prior. The bone was incidentally identified on follicle check ultrasound and was removed via hysteroscopy. The patient conceived one year later, which progressed to a full-term pregnancy.
Conclusion: Retained bony fragments or intact bones should be considered as a possible cause of secondary infertility following therapeutic abortions, emphasizing the importance of ultrasound imaging in preliminary secondary infertility workup.
Keywords: Abortion, Hysteroscopy, Infertility, Retained bone, Ultrasound
Introduction
Retained fetal bone fragments are a rare but known complication of abortion. The incidence remains unclear in the general population, though a study by Makris et al. noted the incidence of retained fetal bone in those undergoing hysteroscopy for abnormal vaginal bleeding to be 0.15% [1]. Common side effects of retained bony fragments include vaginitis, cervicitis, menorrhagia, and infertility [1],[2].
Numerous case reports have documented infertility secondary to retained fetal bones following abortion [2],[3],[4],[5],[6],[7] [8]. Common findings from these cases include mid-trimester abortions, piecemeal removal of conceptus, and identification of fetal bone on transvaginal ultrasound and hysteroscopy. Another common finding is multiple bony fragments, rather than a single intact fetal bone. Furthermore, many of these cases report successful conception and return to regular menstruation following removal. The duration of bone retention has been reported anywhere from 8 weeks to 15 years [8].
Case Report
The patient is a 38-year-old G4P2022 female who presented to clinic for fertility evaluation. She had been off hormonal contraception and trying to conceive for 1.5 years. The patient had two previous full-term deliveries, one at 18 years old and one at 21 years old. At 25 years old, she reported a spontaneous, missed abortion at “2 months” gestation and a therapeutic abortion one year later at “3 months” gestation. Both abortions required D&C. With 1.5 years of infertility following 4 previous pregnancies, she was identified as having secondary infertility.
For the past 12 years, the patient noted occasional long (35 day) menstrual cycles with prominent mid-cycle pain. Physical and vaginal examination was unremarkable. She had a distant history of treated gonorrhea and no history of abnormal Pap smears.
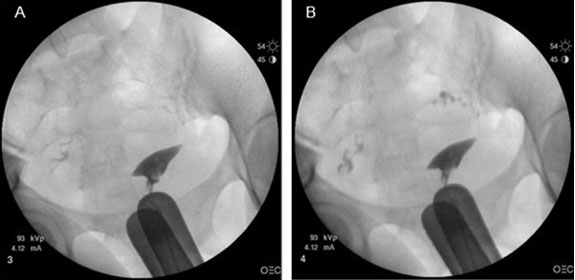
Initial workup for secondary infertility included a hysterosalpingogram, which revealed no tubal occlusion and no indication of foreign body in the uterine cavity (Figure 1).
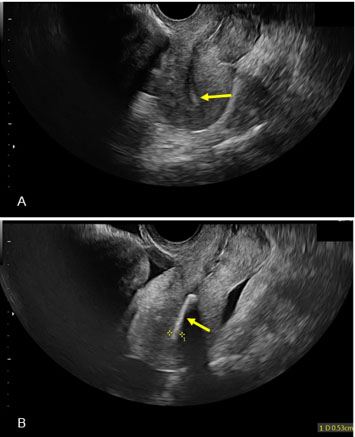
Due to age, lack of vaginal exam findings, and previous known fertility, the patient was trialed on an initial treatment plan of ovarian stimulation with letrozole followed by intrauterine insemination (IUI). At a follow-up follicle check ultrasound, the ultrasonographer noted a retroverted uterus with a pronounced linear echogenic area with distinct shadowing within the canal, measuring 5.3 mm with a solid lining (Figure 2). One ultrasound view obscured this area, and the uterus appeared empty, but another showed a clear view of echogenicity in the uterine cavity. Incidentally, the ultrasonographer also identified a 61×56 mm fibroid in the myometrium. The patient denied any history of intrauterine device (IUD) and given her history of two previous D&Cs, the ultrasonographer notified the physician of possible retained bone.
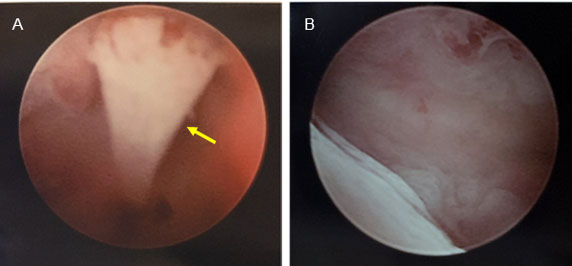
The echogenic substance was removed via operative hysteroscopy by transabdominal ultrasound guidance two months after its identification on ultrasound. The size, shape, color, consistency, and overall appearance of the foreign body was consistent with fetal bone. The foreign body was approximately 22 mm in length, which correlates with an estimated gestational age of 15 weeks and the timing of the patient’s most recent abortion. It was determined clinically that the echogenic substance was fetal bone (Figure 3). The bone was positioned linearly between the fundus and the anterior aspect of the lower uterine segment. The bone was grasped at the distal end and removed intact. The fundal aspect of the bone left a small indentation in the endometrium without extension into the myometrium. This was the only bony piece identified and removed. Complete removal was confirmed with ultrasound and hysteroscopy.
The patient spontaneously conceived 10 months after removal of the fetal femur, confirmed via 7-week ultrasound. At 37 weeks gestation, she had an induction of labor for preeclampsia followed by delivery via cesarean section for failure to progress. Both the patient and infant continue to be healthy six months after delivery.
Discussion
This case represents one of the longest documented instances of retained fetal bone, 13 years. It also is unique in revealing the possibility of secondary fertility with only a single, intact, fetal bone as previous accounts primarily describe retention of several bony fragments. Similar to previous documented cases, fertility was restored following removal [2],[3],[4],[5],[6],[7],[8],[9].
This case helps investigate potential mechanisms for secondary infertility following retention of fetal bone. For example, one theory suggests that retained fetal bones block blastocyst implantation in the uterine lining via uterine inflammation and embryo toxicity [10]. One case study documented increased prostaglandin levels in retention of fetal bone of similar levels as IUD users, lending credence to the uterine inflammation theory [10]. Due to the retention of a singular bone, and her ability to conceive directly after removal of said bone, it can be projected that the placement of the bone was the cause of her secondary infertility. This bone, in essence, was acting as an inert IUD, likely abiding to the uterine inflammation theory as above as well as mechanically blocking implantation. While it is likely that the retained bone is the primary cause of her secondary infertility, the incidental finding of a large fibroid could have additionally contributed to her mid-cycle pain.
Most notably, this case represents the importance of thorough ultrasound imaging in workups for secondary infertility. Had this patient received an ultrasound as part of their initial screening, this fetal bone may have been identified earlier. Given the return-to-fertility nature of retained bones as historically described, this patient potentially could have avoided further hormonal stimulation or reproductive endocrinology testing with early identification of the bone. This case also emphasizes the importance of astute and thorough ultrasonography, as the image of the bone was obscured in one ultrasonic view and unidentifiable in other modalities of imaging, such as hysterosalpingogram, that were previously performed.
Conclusion
In conclusion, as endochondral ossification occurs in week 12, any abortion at this gestational age or later could be associated with risk of retained long bones, adding to our understanding of secondary infertility. Additionally, this case emphasizes the importance of thorough ultrasound imaging in preliminary fertility workup, as early identification of fetal bone has the potential to prevent undue medical workup, expenses, and time.
REFERENCES
1.
Makris N, Stefanidis K, Loutradis D, Anastasiadou K, Hatjipappas G, Antsaklis A. The incidence of retained fetal bone revealed in 2000 diagnostic hysteroscopies. JSLS 2006;10(1):76–7.
[Pubmed]

2.
Bakhshi PS, Allahbadia G, Kauer K, Virk SPS. Hysteroscopic removal of intrauterine retained fetal bones. Gynecol Surg 2004;1:159–66. [CrossRef]
3.
Singla A, Gupta B, Guleria K. First trimester abortion: A rare cause of intrauterine bony spicules. Case Rep Obstet Gynecol 2012;2012:701021. [CrossRef]
[Pubmed]
4.
Moon HS, Park YH, Kwon HY, Hong SH, Kim SK. Iatrogenic secondary infertility caused by residual intrauterine fetal bone after midtrimester abortion. Am J Obstet Gynecol 1997;176(2):369–70. [CrossRef]
[Pubmed]
5.
Panama S, Triolo O, Arezio P. Prolonged retention of fetal bones: Intrauterine device and extrauterine disease. Clin Exp Obstet Gynecol 1990;17(1):47–9.
[Pubmed]
6.
Dawood MY, Jarret JC 2nd. Prolonged intrauterine retention of fetal bones after abortion causing infertility. Am J Obstet Gynecol 1982;143(6):715–7. [CrossRef]
[Pubmed]
7.
Shukr G, Webber V, Vilkins A. 108 Infertility from retained fetal bone after termination: Case report and literature review. Am J Obstet Gynecol 2021;224(6):S807–8. [CrossRef]
8.
Basu M, Mammen C, Owen E. Bony fragments in the uterus: An association with secondary subfertility. Ultrasound Obstet Gynecol 2003;22(4):402–6. [CrossRef]
[Pubmed]
9.
Onderoglu LS, Yarali H, Gultekin M, Katlan D. Endometrial osseous metaplasia: An evolving cause of secondary infertility. Fertil Steril 2008;90(5):2013.e9–11. [CrossRef]
[Pubmed]
10.
Lewis V, Khan-Dawood F, King M, Beckmann C, Dawood MY. Retention of intrauterine fetal bone increases menstrual prostaglandins. Obstet Gynecol 1990;75(3 Pt 2):561–3.
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
All individuals who contributed to the work qualified for authorship.
Author ContributionsBrooke Barton - Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Emma Every - Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Brenda Houmard - Conception of the work, Design of the work, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Lynn Davis - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Brooke Barton et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}