 |
Case Report
Mesh infection after umbilical hernia repair in a pregnant female
1 Department of Obstetrics and Gynecology, Summa Health, Akron, Ohio, USA
2 Northeast Ohio Medical University, Rootstown, Ohio, USA
Address correspondence to:
Renae Jackson
MD, Department of Obstetrics and Gynecology, Summa Health, 141 N Forge St, Akron OH 44304,
USA
Message to Corresponding Author
Article ID: 100148Z08RJ2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Jackson R, Rehman S, Hill K, Graham J. Mesh infection after umbilical hernia repair in a pregnant female. J Case Rep Images Obstet Gynecol 2023;9(1):63–66.ABSTRACT
Introduction: Acute abdominal findings occur in about 1 in 500 pregnancies. Diagnosis of acute abdominal findings in pregnancy can be difficult due to the physiologic and anatomic changes that are intrinsic to pregnancy. In pregnancy, the presence or recurrence of umbilical hernia is common and should be included in the differential diagnosis for acute abdominal findings. Few cases have been reported of complications post-hernia repair during subsequent pregnancies.
Case Report: We report the case of a 31-year-old female with a history of an umbilical hernia repair who presented with acute abdominal findings at 22 weeks gestation attributed to delayed infection of surgical mesh.
Conclusion: This patient’s presentation of acute abdominal findings during pregnancy with a history of umbilical hernia repair one year prior required exclusion of both obstetric and non-obstetric causes to determine diagnosis. There is little published evidence to guide Ob/Gyn physicians in counseling patients on the impact of pregnancy on prior umbilical hernia mesh repair. This case emphasizes the need for surveillance for mesh related complications during subsequent pregnancies in women with a history of mesh umbilical hernia repair.
Keywords: Infected mesh, Mesh repair, Pregnancy, Umbilical hernia
Introduction
Acute abdominal findings occur in approximately 1 in 500 pregnancies [1]. Diagnosis of acute abdomen can be difficult due to the physiological changes in a pregnant female. In particular, the expanding uterus can cause rearrangement of intra-abdominal organs and complicate physical exams. Furthermore, symptoms of nausea, vomiting, and abdominal pain are not uncommon in pregnancy and can overshadow prompt diagnosis of other acute abdominal processes. An acute abdomen can develop from a variety of non-obstetric causes such as gastrointestinal, urogenital, gynecological, and surgical complications. Obstetric causes of an acute abdomen can include ectopic pregnancy, placental abruption, abnormal placentation, and uterine rupture. Of the non-obstetric sources, the leading cause of acute abdomen is appendicitis, reportedly found in up to one in 500 pregnancies [1]. This is followed by acute cholecystitis and bowel obstruction [1],[2]. Complications from prior surgeries make up a small subset of acute abdominal concerns.
In pregnancy, the presence or recurrence of umbilical hernia is common and can be exacerbated by the increased intra-abdominal pressure [3]. In a national cohort study of 470,000 women, findings demonstrated that the cumulative incidence of ventral hernia repair was 14% over a 10 year period, with subsequent pregnancy after repair resulting in a 1.6-fold increase in recurrence and seven fold increase in repair in parous women compared to nulliparous women [3]. Repair is necessary to prevent incarceration or strangulation of abdominal contents; however, repair of these hernias in the nonpregnant population has been reported to be accompanied by postoperative infection, hernia recurrence, and chronic pain [4],[5],[6]. Despite the vast literature on routine umbilical hernia repair, there is little evidence on optimal repair methods, timeline of repair, or complications of umbilical hernia repair in females who subsequently become pregnant. Few cases have been documented of hernia repair complications on subsequent pregnancies. Complications from hernia repair on later pregnancies that have been documented include chronic pain and recurrence of hernia [7],[8]. However, there have been no cases reported of complications during pregnancy after umbilical hernia repairs with mesh. This case highlights a unique complication of umbilical hernia repair with mesh in a pregnant female one year post repair.
Case Report
A 31-year-old female with a history of two prior cesarean sections and no other relevant medical history was referred to general surgery for a reducible, symptomatic umbilical hernia. Six weeks after diagnosis, she underwent a mesh augmented laparoscopic repair of an incarcerated umbilical hernia. The patient’s postoperative visits indicated an uncomplicated postoperative course with only minimal chronic abdominal pain.
One year later, the patient presented to obstetric triage at 22 weeks gestation complaining of severe abdominal pain, constipation, nausea, and vomiting. She denied any fever, chills, chest pain, shortness of breath, vaginal discharge, dysuria, or hematuria at that time. On arrival, the patient’s vitals were within normal limits, and she was afebrile. Physical exam revealed a gravid uterus, moderately distended abdomen with generalized tenderness to palpation, rebound, and guarding. Speculum exam showed no pooling of fluid, with a visually closed cervix. Fetal heart rate was present and there were no contractions on the tocometer.
Further diagnostic workup included a complete blood count which was significant for mild leukocytosis at 11.8 K/uL and hemoglobin at 11.3 g/dL. Electrolytes, urinalysis, lipase, and lactate were within normal limits. Chlamydia, gonorrhea, and trichomonas testing were all negative. Computed tomography (CT) scan demonstrated soft tissue extending beyond the uterine wall on the anterior left aspect encompassing a portion of small bowel (Figure 1). Computed tomography read was concerning for a possible placenta percreta. There was also a small amount of free fluid in the pelvis with normal appearing appendix and no bowel obstruction noted. Abdominal ultrasound was performed due to concern for abnormal placentation. The ultrasound was reassuring for no placental abnormality; however, inflammation of the bowel and free fluid was noted in the umbilical region (Figure 2). General surgery was consulted to evaluate the patient, given suspicion for non-obstetrical acute abdomen.
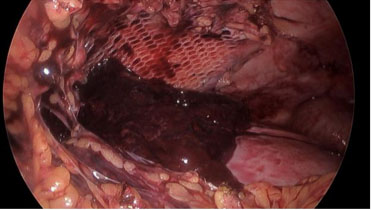
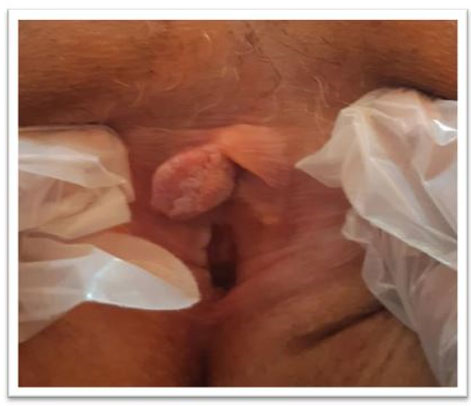
Exploratory laparoscopy was performed which demonstrated hemoperitoneum and free floating mesh with purulent fluid consistent with infected mesh. Omental-uterine adhesions were noted over the previous hysterotomy which appeared to be the source of hemoperitoneum (Figure 3). Lysis of adhesions was performed and the mesh was removed. The procedure went without any complications and the patient was sent to recovery in stable condition. She received postoperative antibiotics for intra-abdominal infection. Postoperatively she did well and was stable for discharge home on postoperative day five.


Discussion
The patient’s presentation with acute abdominal findings during pregnancy, in association with a history of umbilical hernia repair one year prior, required exclusion of both obstetric and non-obstetric causes when determining diagnosis. Acute abdominal findings can often be overshadowed by typical findings in pregnancy such as vomiting, nausea, and pain. Therefore, determining the root cause of an acute complaint in a pregnant patient warrants a more thorough investigation. Obstetric causes that were addressed in an attempt to rule out sources of acute abdominal findings in this case included placental abruption, abnormal placentation, preterm labor, and uterine rupture. Non-obstetric causes that were investigated included appendicitis and cholecystitis, as well as post-procedure related complications of small bowel obstruction, adhesions, infections, and recurrent hernias. In this case, she had a gestational age of 22 weeks with stable vitals. Her only complaint of increased pain along with a history of constipation and lack of concerning vital signs were more suggestive of severe constipation rather than an acute abdominal process. On further examination, however, a physical exam confirmed a distended abdomen with rebounding and guarding, creating concern for acute processes. Speculum exam was significant for closed cervix with no pooling of fluid or vaginal bleeding, making obstetrical causes of placental abruption and preterm labor less likely. Laboratory findings of mild leukocytosis were more consistent with an infection but also seen in normal pregnancy. Imaging studies continued to rule out possible causes as seen by CT which did not show appendicitis or cholecystitis. However, it was concerning for a possible placenta percreta. Ultrasound was conducted and inflammation of the bowel was noted as well as free fluid in the umbilical region. No placental abnormalities were seen which made placental disorders less likely. Once the majority of obstetrical causes were ruled out following physical exam, laboratory results, and imaging studies, exploratory laparoscopy was performed. This procedure found infected mesh and omental-uterine adhesions which appeared to be the source of hemoperitoneum.
When considering complications for umbilical hernia repair with mesh, complications can be divided into early and late presenting complications. Early complications typically include infection, hematoma, and seroma. Late appearing complications include obstructions, adhesions, recurrence, and chronic pain. Comorbidities such as liver disease, ascites, obesity, diabetes, and primary suture repair without mesh are associated with increased recurrence. Postoperative complications are most often seen in the first eight weeks after repair. However, in this case the patient did not present within the typical time frame as depicted by the literature. She presented with a postoperative mesh infection one year after repair which is outside the typical time frame.
Conclusion
This patient’s presentation of acute abdominal findings during pregnancy with a history of umbilical hernia repair one year prior required exclusion of both obstetric and non-obstetric causes to determine diagnosis. There is little published evidence to guide obstetricians in counseling patients on the impact of pregnancy on prior umbilical hernia mesh repair. This case emphasizes the need for surveillance for mesh related complications during subsequent pregnancies in women with a history of mesh umbilical hernia repair.
REFERENCES
1.
Augustin G, Majerovic M. Non-obstetrical acute abdomen during pregnancy. Eur J Obstet Gynecol Reprod Biol 2007;131(1):4–12. [CrossRef]
[Pubmed]

2.
Diegelmann L. Nonobstetric abdominal pain and surgical emergencies in pregnancy. Emerg Med Clin North Am 2012;30(4):885–901. [CrossRef]
[Pubmed]
3.
Oma E, Jensen KK, Bisgaard T, Jorgensen LN. Association of primary ventral hernia and pregnancy. Ann Surg 2020;272(1):170–6. [CrossRef]
[Pubmed]
4.
Winsnes A, Haapamäki MM, Gunnarsson U, Strigård K. Surgical outcome of mesh and suture repair in primary umbilical hernia: Postoperative complications and recurrence. Hernia 2016;20(4):509–16. [CrossRef]
[Pubmed]
5.
Arroyo A, García P, Pérez F, Andreu J, Candela F, Calpena R. Randomized clinical trial comparing suture and mesh repair of umbilical hernia in adults. Br J Surg 2001;88(10):1321–3. [CrossRef]
[Pubmed]
6.
Nguyen MT, Berger RL, Hicks SC, et al. Comparison of outcomes of synthetic mesh vs suture repair of elective primary ventral herniorrhaphy: A systematic review and meta-analysis. JAMA Surg 2014;149(5):415–21. [CrossRef]
[Pubmed]
7.
Schoenmaeckers E, Stirler V, Raymakers J, Rakic S. Pregnancy following laparoscopic mesh repair of ventral abdominal wall hernia. JSLS 2012;16(1):85–8. [CrossRef]
[Pubmed]
8.
Oma E, Jensen KK, Jorgensen LN. Increased risk of ventral hernia recurrence after pregnancy: A nationwide register-based study. Am J Surg 2017;214(3):474–8. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Renae Jackson - Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sahar Rehman - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kylan Hill - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
James Graham - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Renae Jackson et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}