 |
Case Report
Mature teratoma during pregnancy: A case report
1 Resident Doctor in Obstetrics and Gynecology Department, University Hospital Center Ibn Rochd, Casablanca 20100, Morocco
2 Professor in Obstetrics and Gynecology Department, University Hospital Center Ibn Rochd, Casablanca 20100, Morocco
3 Head of Service in Obstetrics and Gynecology Department, University Hospital Center Ibn Rochd, Casablanca 20100, Morocco
Address correspondence to:
Imane Joudar
Department of Gynecology and Obstetrics, University Hospital Center Ibn Rochd, Casablanca, Morocco; Faculty of Medicine and Pharmacy, Hassan II University, 1 rue des hôpitaux, Casablanca,
Morocco
Message to Corresponding Author
Article ID: 100150Z08IJ2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Joudar I, El Abbassi I, Khalloufi C, Jalal M, Lamrissi A, Bouhya S. Mature teratoma during pregnancy: A case report. J Case Rep Images Obstet Gynecol 2023;9(1):70–74.ABSTRACT
Introduction: The mature teratoma or dermoid cyst of the ovary is a benign tumor with a good prognosis which constitutes less than 1% of ovarian tumors. Its association with pregnancy is rare.
Case Report: We report the case of a 30-year-old woman admitted for acute pelvic pain with an abdomino-pelvic mass diagnosed on pelvic ultrasound supplemented by pelvic magnetic resonance imaging (MRI). The indication for surgical exploration was given because of her presentation with pain raising, the size of the mass, and the risk of torsion. The patient underwent conservative treatment based on a cystectomy with multiple biopsies, the anatomical-pathological result of which was in favor of a mature ovarian teratoma. Through the analysis of this observation and the data of the literature, we will discuss the different aspects of this association.
Conclusion: Mature teratoma and pregnancy are still a rare entity. Expectant management is appropriate in asymptomatic small mature teratoma. However in symptomatic or large mature teratoma surgical intervention is needed.
Keywords: Expectant management, Mature teratoma, Ovarian cystectomy, Pregnancy, Radiological examinations
Introduction
Mature cystic teratoma is the most common ovarian teratoma. It is in most cases asymptomatic unless it becomes more complicated or increases in volume. Its diagnosis is generally confused with other clinical and paraclinical differential diagnosis [1],[2].
The diagnosis is usually suggested by ultrasound and confirmed by computed tomography (CT) scan or magnetic resonance imaging (MRI) in the presence of an ovarian mass containing fat. Histology holds the greatest importance in the confirmation of the diagnosis of a mature teratoma. The treatment is exclusively surgical with different methods. Fertility preservation remains the main concern in treatment [3]. Its discovery during pregnancy is an even rarer fact. Few cases have been reported in the literature.
Case Report
Mrs. L.A, 30 years old, Gravida 1 Para 0, without any past history of significance, presented with lower abdominal pain in the presence of pelvic-abdominal mass discovered two months ago. She was four months pregnant and the mass noted to be gradually increasing when she was generally well. The mass was at the level of the umbilicus.
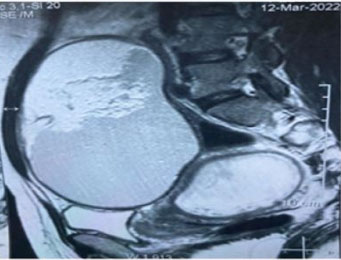
Pelvic ultrasound revealed a large homogeneous hyperechoic abdomino-pelvic mass of 15×15 cm in an evolving single-fetal pregnancy of 16 weeks (Figure 1). Tumor markers were normal levels. The pelvic and abdominal MRI confirmed the presence of an abdomino-pelvic mass partitioned under the umbilical, well encapsulated, 16 cm in long axis, of probable ovarian origin with three components, tissue, fatty and calcium, evoking a germ cell tumor of the immature teratoma type classified 0’Rads 4 (Figure 2).
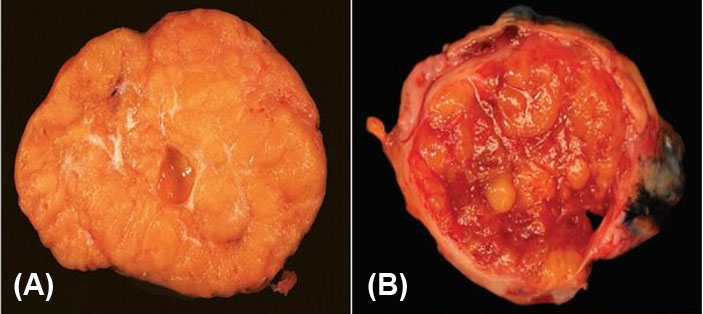
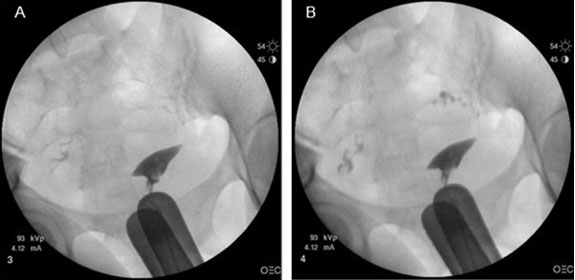
The patient benefited from a laparotomy with exploration (Figure 3): Fallopian tubes, left ovary, and gravid uterus looked normal. The right ovary was enlarged, measuring approximately 20 cm in long axis, non-adherent, with a smooth surface, without exophytic vegetation. No ascites or peritoneal implants were seen. A right cystectomy with several biopsies was performed as well as a sample of lavage fluid for cytology. The anatomo-pathological result was in favor of a mature and multi-tissue ovarian teratoma with no immature component (Figure 4).



Discussion
The frequency of ovarian tumors discovered during pregnancy is between 0.3% and 5.4%. The most common benign organic ovarian tumors during pregnancy are dermoid cysts and cystadenomas [4]. It had been speculated that hormonal changes due to pregnancy may be responsible for an increase in the size of dermoid cysts. In a prospective study, Caspi et al. followed 49 young women with a known dermoid cyst of less than 6 cm. In the 68 pregnancies that occurred, the size of the cysts remained stable throughout the pregnancy [5].
The main risk of complication of dermoid cysts during pregnancy is adnexal torsion, estimated at around 8%, especially in the 1st trimester and at the beginning of the 2nd trimester. There were no noted cases of malignant degeneration of dermoid cysts in the two follow-up studies by Caspi et al. and Caruso et al. during pregnancy [5]. Tumor markers are not reliable during pregnancy to assess the risk of malignancy. Ultrasound remains the reference examination for characterizing an ovarian tumor during pregnancy. Its specificity is lower for the diagnosis of malignancy than outside of pregnancy. Magnetic resonance imaging is an excellent examination in the diagnosis of ovarian tumors during pregnancy and provides additional information to ultrasound [6]. Laparoscopy is the gold standard in the management of this pathology. Cystectomy presents the best choice to preserve the ovarian parenchyma as much as possible. Oophorectomy or salpingo-oophorectomy may be necessary if the lesion involves the entire ovary and no recognizable parenchyma remains [7].
Surgery should be avoided in the 1st trimester, however, is indicated in case of symptomatic ovarian tumor raising suspicion of adnexal torsion [8]. In other cases, an ultrasound check will be carried out at the beginning of the 2nd trimester to ensure that it persists. In the case of a benign-looking ovarian tumor that does not increase in size, less than 6 cm, the risk of complication is low and expectant management with follow-up are recommended. In the case of a presumed benign ovarian tumor larger than 6 cm, the data in the literature are insufficient to conclude between abstention and intervention [9]. An increase in the size of the tumor would be an element prompting an intervention. In the event of a surgical decision, the risk of miscarriage is evaluated at 2.8% and must be clearly explained to the patient. Subsequently and regardless of the trimester of pregnancy, the discovery of a presumed benign symptomatic ovarian tumor, raising fears of adnexal torsion, remains an indication for surgery. It is noted that after 20 gestational weeks (GWs) the risks of torsion are rare, and that after the 23 GWs, the risks of obstetric complications (premature delivery) from surgery are higher. These data encourage postponing surgery after delivery in the case of a presumed benign asymptomatic ovarian tumor after 20–23 GW [10].
Histology is essential for confirming the diagnosis of mature teratoma. The prognosis is excellent, subsequent regular ultrasound monitoring, theoretically throughout the period of genital activity, should be considered [9],[10].
Conclusion
Mature teratoma is a benign tumor with a good prognosis. Diagnosis is presumed by radiological examinations and confirmed by pathology. Its management should be directed as often as possible toward conservative surgical treatment with preservation of fertility.
Its association with pregnancy is still a rare entity. Expectant management with follow-up is recommended in the case of persistent but stable presumed benign ovarian tumors of less than 6 cm. Surgery is indicated when the mass is large in size or if the patient is symptomatic.
REFERENCES
1.
Bouzoubaa W, Jayi S, Alaoui FZF, Chaara H, Melhouf MA. Immature teratoma of the ovary: About a case. [Article in French]. Pan Afr Med J 2017;27:263. [CrossRef]
[Pubmed]

2.
Chenana A, Kouach J, Moussaoui D, Dehayni M. International Journal of Innovation and Applied Studies 2016;15(3):503–14.
3.
Thomassin-Naggara I, Toussaint I, Perrot N, et al. Characterization of complex adnexal masses: Value of adding perfusion- and diffusion-weighted MR imaging to conventional MR imaging. Radiology 2011;258(3):793–803. [CrossRef]
[Pubmed]
4.
Caspi B, Levi R, Appelman Z, Rabinerson D, Goldman G, Hagay Z. Conservative management of ovarian cystic teratoma during pregnancy and labor. Am J Obstet Gynecol 2000;182(3):503–5. [CrossRef]
[Pubmed]
5.
Tariel O, Huissoud C, Rudigoz RC, Dubernard G. Presumed benign ovarian tumors during pregnancy. [Article in French]. J Gynecol Obstet Biol Reprod (Paris) 2013;42(8):842–55. [CrossRef]
[Pubmed]
6.
Haddada S, Selleret L, Fedida B, et al. Adnexal masses and pregnancy: Which diagnosis and which imaging? Imagerie de la Femme 2017;27(2):104–10.
7.
Aggarwal P, Kehoe S. Ovarian tumours in pregnancy: A literature review. Eur J Obstet Gynecol Reprod Biol 2011;155(2):119–24. [CrossRef]
[Pubmed]
8.
Cohen-Herriou K, Semal-Michel S, Lucot JP, Poncelet E, Rubod C. Management of ovarian cysts during pregnancy: Lille’s experience and literature review. [Article in French]. Gynecol Obstet Fertil 2013;41(1):67–72. [CrossRef]
[Pubmed]
9.
Dubernard G, Bazot M, Barranger E, et al. Accuracy of MR imaging combined with sonography for the diagnosis of persistent adnexal masses during pregnancy: About nine cases. [Article in French]. Gynecol Obstet Fertil 2005;33(5):293–8. [CrossRef]
[Pubmed]
10.
Bourdel N, Canis M. Treatment strategies in presumed benign ovarian tumors. [Article in French]. J Gynecol Obstet Biol Reprod (Paris) 2013;42(8):802–15. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Imane Joudar - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Imane El Abbassi - Conception of the work, Design of the work, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Chadia Khalloufi - Conception of the work, Design of the work, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mohamed Jalal - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Amine Lamrissi - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Said Bouhya - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Imane Joudar et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}