 |
Case Report
Ovarian mucinous adenocarcinoma and false negative frozen pathology: A case report and review of the literature
1 Resident Physician, Department of Obstetrics, Gynecology and Reproductive Sciences, University of California at San Diego, 9300 Campus Point Drive, MC 7433, La Jolla, CA 92037, USA
2 Assistant Professor, Division of Gynecologic Oncology, Department of Obstetrics, Gynecology and Reproductive Sciences, University of California at San Diego, 3855 Health Sciences Drive, La Jolla, CA 92037, USA
Address correspondence to:
Renee T Sullender
9300 Campus Point Drive, MC 7433, La Jolla, CA 92037,
USA
Message to Corresponding Author
Article ID: 100153Z08RS2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Sullender RT, Binder PS. Ovarian mucinous adenocarcinoma and false negative frozen pathology: A case report and review of the literature. J Case Rep Images Obstet Gynecol 2023;9(1):83–86.ABSTRACT
Introduction: In this case report we discuss the presentation and management of a woman with a large adnexal mass.
Case Report: This report describes a 32-year-old year healthy woman who presented with four months of increasing abdominal fullness. Computed tomography (CT) imaging showed a 34 cm fluid-filled left adnexal mass with few thin septations. Tumor markers were within normal limits. She strongly desired minimally invasive surgery in the setting of low concern for malignancy. A mini-laparotomy was performed, purse string sutures were placed through the cyst wall, and fluid was aspirated with minimal spillage. Her left tube and ovary were resected laparoscopically. Intraoperative frozen pathology returned as mucinous cystadenoma with some areas of atypia. Final pathology resulted with Grade 2 mucinous adenocarcinoma and she was taken back to the operating room for a surgical staging procedure. Pathology from her laparoscopic staging surgery was benign. She underwent chemotherapy with carboplatin/paclitaxel for Stage 1C1, Grade 2 mucinous adenocarcinoma of the ovary based on intra-operative spillage.
Conclusion: Despite reassuring imaging and tumor markers, particularly in the setting of frozen pathology with low concern for malignancy, final pathology may indicate carcinoma. Although the accuracy of intra-operative frozen pathology is generally high, both gynecologic oncologists and non-oncologic gynecologists should be aware of the limitations of the test and counsel patients that the final pathology may be discordant. Appropriate counseling about the risk of intra-operative spillage and subsequent upstaging is of particular importance.
Keywords: Adnexal mass, Frozen pathology, Ovarian cancer, Ovarian mucinous adenocarcinoma
Introduction
Adnexal masses are a common gynecologic finding. When small, they are often asymptomatic but larger masses can cause bulk symptoms such as pressure, bloating, and early satiety. Adnexal masses are more likely to be malignant when identified in post-menopausal women compared to younger patients. Providers should consider imaging findings such as size, septations, internal blood flow, and papillary projections in the adnexal masses when conducting surgical planning and when deciding if a general gynecologist or oncologist should perform the surgery. Sometimes despite low pre-operative concerns for malignancy and reassuring intraoperative frozen pathology, final pathology may result with malignancy.
Case Report
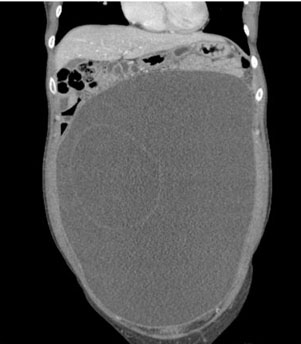
A 32-year-old nulliparous female presented to the emergency room reporting increasing abdominal fullness and discomfort. A computed tomography (CT) scan identified a 34 × 16 × 26-cm fluid filled cystic lesion likely arising from the left adnexa with a few thin septations (Figure 1 and Figure 2). There was mild ascites without peritoneal thickening or nodularity.
The gynecology service was consulted. The patient further described abdominal pressure worsening over the past four months. She denied changes in bowel or urinary function, appetite, weight, or night sweats. She had not been sexually active in three years. She reported regular monthly menses and denied any pertinent medical, surgical, or family history. Her social history was notable for being a Chinese immigrant who did not have health concerns requiring medical attention since arriving in the United States. A large mass was palpable below her ribcage both on bimanual pelvic and abdominal exams. Since the patient was stable, she was referred for outpatient follow-up with gynecologic oncology given the size of the mass.
At her initial appointment with gynecologic oncology, the imaging and normal tumor markers cancer antigen 125 (CA-125) 35 U/mL, carbohydrate antigen 19-9 (CA 19-9) 22 U/mL, lactate dehydrogenase (LDH) 193 U/L, alpha fetoprotein (AFP) 2.9 ng/mL, inhibin B 45 pg/mL were reviewed. Given the normal tumor markers and the simple fluid filled cyst, the risk of cancer was deemed to be low. She was specifically counseled on the risk of upstaging if cancer was found including the risk of spillage. The decision was made to attempt a mini-laparotomy with drainage of the simple appearing cystic fluid followed by laparoscopic resection of abnormal mass. The patient strongly desired future fertility and wanted fertility sparing surgical staging even if cancer was found.
During surgery, a 6-cm supraumbilical vertical incision was made. Two purse string sutures were placed through the cyst wall with 2-0 vicryl without rupturing the mass. A 3-mm incision was made through the cyst wall, the suction was placed in the mass, and the purse string stitches were tightened around the suction to limit the fluid from leaking into the abdomen. Approximately 9 liters of clear fluid was drained. An additional cyst within this mass was palpable and was penetrated with the suction with an additional liter of brown fluid drained. The purse-string suture was then tied down after removal of suction. The cyst was then placed back into the abdomen and the fascial incision was partially closed with 0-vicryl on a UR-6 needle. A 12-mm balloon port was then placed directly through the open portion of the incision. Right and left lateral 5-mm accessory ports were then placed under direct visualization. The cyst was found to be arising from the left ovary with a dilated left fallopian tube. The left peritoneum lateral to the infundibulopelvic ligament was entered and dissected to visualize the left ureter. The left tube and ovary were then removed in the usual fashion with the Ligasure device.
The supraumbilical port was removed. The mass was elevated to the level of the anterior abdominal wall and removed through the laparotomy incision after some extension to accommodate the residual mass intact. The mass was sent to pathology for frozen section. Some fluid was noted in the cul-de-sac during laparoscopy. Omentum and bowel were inspected without evidence of disease. Her remaining pelvic organs were unremarkable. The vertical fascial incision was then closed with a running stitch of 0-vicryl on a UR-6 needle.
Frozen section returned as mucinous cystadenoma with some areas of atypia but unable to determine the percentage of atypical tissue. Surgical staging was not performed given no obvious evidence of malignancy. The patient was discharged home on post-operative day 1 when she was meeting post-operative milestones.
Final pathology then resulted with Grade 2 mucinous adenocarcinoma of the ovary with an unremarkable fallopian tube. Given a final diagnosis of mucinous carcinoma with possible surgical spillage of fluid in the pelvis, the decision was made to perform a second surgical staging procedure.
The next month, she underwent an uncomplicated diagnostic laparoscopy, omentectomy, appendectomy, peritoneal biopsies, pelvic lymph node dissection, and pelvic washings, all of which were negative for carcinoma. The periaortic lymph nodes were evaluated transperitoneally. There were no enlarged lymph nodes and minimal lymphatic tissue was seen in the pelvis. The decision was made not to perform periaortic lymph node dissection in the context of low incidence of lymphatic involvement with mucinous cancers. She was subsequently noted to have Grade 2, Stage 1C1 disease given the possible intra-operative spill. She has since received 3 cycles of carboplatin/paclitaxel and is doing well without evidence of recurrence 1 year after surgery. She has not yet attempted pregnancy.
Our organizational Institutional Review Board judged that this case report did not require their review. Patient consent was obtained to present her case in the literature.

Discussion
Decision for incision
The patient was originally counseled to undergo an exploratory laparotomy by her gynecologic oncologic surgeon, in part due to the large size of the mass. However, she strongly desired a minimally invasive surgery given her lack of social support to help her during the recovery process and her desire to return to work within a few weeks. Her CT showed a simple fluid containing cyst with few thin septations and did not indicate any solid areas or any metastatic disease. Given the variety of reassuring findings, the risk of cancer was deemed to be low. The patient was educated about the risk of upstaging if cancer was found, including the risk of spillage. She was then consented for a mini-laparotomy with drainage of the cyst. Even though the mass was found to be malignant on final pathology, a mini laparotomy was a reasonable option to pursue based on the low concern for cancer and the patient’s strong preference for minimally invasive surgery. During pre-operative counseling on route of surgery, gynecologists should remember that early stage ovarian cancer can be non-specific on imaging, microscopic metastases may not be visible, and cancer markers can be normal.
As per National Comprehensive Cancer Network guidelines for Stage 1C1 disease, both observation and chemotherapy were reasonable [1]. Given her cancer showed expansile and infiltrative features, she was recommended to proceed with chemotherapy [2].
False negative frozen section
Surgeons often rely on intra-operative frozen section pathology to decide whether cancer surgical staging should be performed during an operation. In this case, the rapid frozen pathology did not suggest malignancy, so the patient did not have staging performed during her initial operation. However, had the frozen section accurately reflected malignancy, she could have had surgical staging during her initial operation and been spared a second surgery. It is important for gynecologists to be aware of the accuracy of frozen sections when performing surgery for adnexal masses.
A 2016 Cochrane Review evaluated ovarian frozen section pathology compared to the permanent paraffin section as the standard reference [3]. When a positive test was defined as invasive cancer and a negative test as either a borderline or benign tumor, the average specificity was 90.0% and the average specificity was 99.5%. When a positive test was defined as either invasive cancer or borderline and a negative test as benign tumor, the average sensitivity was 96.5% and the average specificity was 89.5%. In general, the review noted that if a frozen section showed a benign or invasive cancer, the final diagnosis was consistent 94% and 99% of the time respectively. If a frozen section showed a borderline tumor, 21% of the time the final diagnosis would be invasive cancer, indicating less accuracy in borderline tumor diagnosis. Based on this literature, surgeons can have high confidence in the accuracy of frozen pathology indicating either benign tumors or invasive cancer while recognizing that 6% of the time, the initial benign pathology may be incorrect.
The accuracy of frozen section pathology may be lower in children than adults, as suggested by a Children’s Oncology Group study of patients up to age 20 with malignant ovarian germ cell tumors which found that intra-operative frozen section was incorrect in 38.3% of patients [4].
Conclusion
Although the accuracy of intra-operative frozen pathology is generally high, gynecologists should be aware of discordance rates between rapid frozen and final pathology reports and counsel patients of this possibility. Patients with adnexal masses should always be educated about the risk of malignancy and the possibility of requiring a second surgery if the first is performed by a non-oncologist and/or if additional staging surgery is recommended based on final pathology report.
REFERENCES
1.
Armstrong DK, Alvarez RD, Bakkum-Gamez JN, et al. Ovarian cancer, Version 2.2020, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 2021;19(2):191–226. [CrossRef]
[Pubmed]

2.
Colombo N, Sessa C, du Bois A, et al. ESMO-ESGO consensus conference recommendations on ovarian cancer: Pathology and molecular biology, early and advanced stages, borderline tumours and recurrent disease†. Ann Oncol 2019;30(5):672–705. [CrossRef]
[Pubmed]
3.
Ratnavelu NDG, Brown AP, Mallett S, et al. Intraoperative frozen section analysis for the diagnosis of early stage ovarian cancer in suspicious pelvic masses. Cochrane Database Syst Rev 2016;3(3):CD010360. [CrossRef]
[Pubmed]
4.
Dicken BJ, Billmire DF, Rich B, et al. Utility of frozen section in pediatric and adolescent malignant ovarian nonseminomatous germ cell tumors: A report from the children’s oncology group. Gynecol Oncol 2022;166(3):476–80. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
We would like to thank the patient who allowed us to share her story in this article so that it may inform future gynecologic care.
Author ContributionsRenee T Sullender - Conception of the work, Design of the work, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Pratibha S Binder - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Renee T Sullender et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}