 |
Case Report
Female paraurethral leiomyoma: A lateral transvestibular approach to a symptomatic tumor
1 Urology and Nephrology Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2 Simon Cancer Center, Indiana University, Indianapolis, Indiana, United States of America
3 Department of Urology, The Ohio State University, Columbus, Ohio, United States of America
Address correspondence to:
Farzaneh Sharifiaghdas
MD, No. 103, 9th Boostan St, Pasdaran St, Tehran, Tehran Province, Zip Code# 166668111,
Iran
Message to Corresponding Author
Article ID: 100173Z08NR2024
Access full text article on other devices

Access PDF of article on other devices

How to cite this article
Rostaminejad N, Kianinejad N, Soltani-Tehrani A, Sharifiaghdas F. Female paraurethral leiomyoma: A lateral transvestibular approach to a symptomatic tumor. J Case Rep Images Obstet Gynecol 2024;10(1):38–42.ABSTRACT
We report a rare case of leiomyoma of the female urethra. A 31-year-old married woman, gravid and para one with no history of prior surgery, malignancy or other significant disease was referred to our clinic with a complaint of a mass protruding from the top of the vagina and difficulty voiding from 18 months ago. The mass had a rapid growth causing urinary obstructive symptoms, dyspareunia which turned to a vast palpable mass protruding the vagina. A definite surgical excision was launched via a lateral transvestibular approach demonstrating no attachment to the urethral tract. The histopathology report confirmed spindle cell tumor consistent with leiomyoma. During the 6-month follow-up period, there was no tumoral recurrence, and neither initial obstructive symptoms nor emerging de-novo incontinency were not observed. In resection of such tumors, care should be taken to spare urethral sphincter in order to prevent future incontinency.
Keywords: Genitourinary tract, Paraurethral leiomyoma, Tumor
Introduction
A leiomyoma is a benign tumor of smooth muscle origin that could affect mainly gastrointestinal and genitourinary tract. Leiomyoma may involve the renal capsule, ureter, bladder wall, urethra, or paraurethral origin in the urinary tract, though the two latter (urethra and paraurethral) are a rare presentation of leiomyoma [1]. Although leiomyomas are benign in nature and surgery is definitive curative management, the vicinity of the tumor to important structures such as nerves and muscles may cause a challenge for a surgeon to spare those organs. In the present study, we introduce a female with a paraurethral tumor, apply our new technique in our center, and enumerate potential hazards in coping with these cases.
Case Report
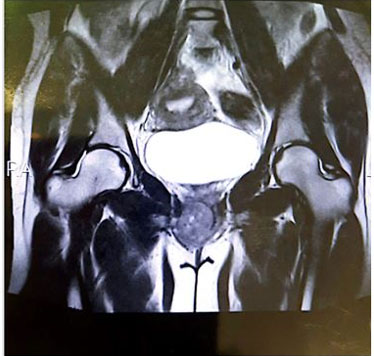
A 31-year-old woman gravida and para one was referred to our clinic due to a gradually enlarging mass that had noticed 18 months earlier, accompanied by dyspareunia and difficulty in urination. The patient reported no significant history of prior surgeries or medical treatments, and the size of the tumor did not appear to correlate with her menstrual cycle. Upon examination, a large, rounded tumor was observed on the right side of the urethral meatus, protruding toward the left (Figure 1). Although the tumor felt firm upon palpation, it appeared to be unconnected to its surrounding structures. Post-void residual volume was measured at 300 mL. During cystourethroscopy, no obvious tumors were detected within the urethra or bladder. However, the examination revealed the protruding effect of the paraurethral tumor. Transvaginal ultrasound and pelvic magnetic resonance imaging (MRI) indicated a tumor measuring 6×5 cm at its largest dimensions, located adjacent to the urethra and exerting pressure (Figure 2). Following thorough patient education regarding potential risks and obtaining informed consent, surgery was performed based on a tentative diagnosis.
Surgical technique
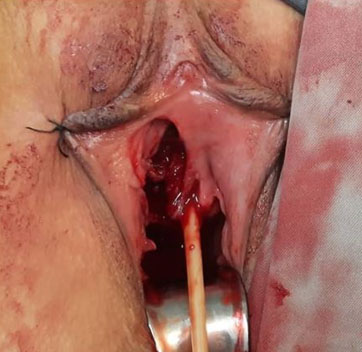
After general anesthesia, in dorsal lithotomy position, a foley catheter was placed. With a scalpel no. 15 size, a delicate dissection was performed transvestibularly at the most lateral point of the tumor using Metzenbaum scissors and wet gauze soaked with epinephrine, sharp and blunt dissection was advanced to detach the tumor from its underlying tissues. The tumor was lying on bladder neck and urethra on its proximal and medial boundaries. Care was taken not to make inadvertent damage to the rhabdo and smooth urethral sphincter. No frank invasion to the above organs and vaginal wall was observed. A 5.5×5×4 rubbery tumor was resected and the surgical site was repaired with 4-0 vicryl sutures in two rows. The patient was discharged after and the foley catheter was kept for 48 hours. During the 6-month post-op period, the patient did not experience any urinary incontinency, voiding symptoms or dyspareunia and healing process went uneventful (Figure 3, Figure 4, Figure 5).
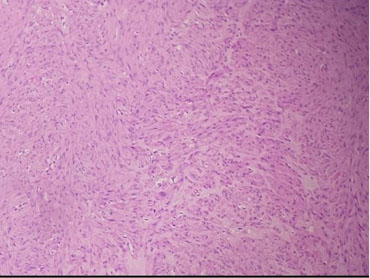
The histopathology examination of the tumor after immunohistochemistry (IHC), smooth muscle actin (SMA), and Desmin staining was positive for CD68, S100, CKEA, IAE3, and CD34 affirming spindle cell tumor consistent with leiomyoma (Figure 6).



Discussion
Periurethral masses are frequently encountered in women and can pose diagnostic and therapeutic dilemmas. In a study involving a significant number of women admitted for surgery due to periurethral masses, the primary pathologies identified were urethral diverticulum (84%), vaginal cysts (7%), and leiomyoma (5%) [2]. Additionally, other potential etiological factors such as urethral caruncles, Skene gland abscesses or cysts, mucosal prolapse, and Gartner’s duct cysts may also be observed [3]. In the case of leiomyoma, a transvaginal ultrasonography may report a solid tumor with a homogenous internal echo. Leiomyoma in pelvic MRI is portrayed hypointense or isointense in T1 and hyperintense or isointense in T2 and not invading to urethra and surrounding structures [4]. Cystourethroscopy is a valuable tool to rule out pathologies originating from bladder and urethra and also makes biopsy of the tumor feasible if there is any doubt of the entity of the tissue.
Leiomyomas in the genitourinary system can emerge from various structures containing smooth muscle. While the renal capsule is most commonly associated with their origin within this category [5], leiomyomas can also manifest in the ureter, bladder, urethra, and epididymis in men [6]. These tumors typically exhibit estrogen receptors on their surface, suggesting a propensity for enlargement during pregnancy or hormonal therapy and implying a potential role for hormonal treatment [7]. However, instances of leiomyomas appearing after menopause may challenge this hypothesis [8]. Some argue that leiomyomas originating from the smooth muscle surrounding the urethra are more accurately termed “paraurethral” tumors [9], whereas others define a tumor as urethral if it is firmly attached to the urethra and cannot be dissected without causing mucosal damage [3].
Surgical excision remains the cornerstone of treatment for both urethral and paraurethral conditions. Transurethral resection has shown favorable outcomes in treating urethral tumors [8], while a transvaginal approach has been commonly utilized for paraurethral leiomyomas [9],[10]. To the best of our knowledge, our study represents the first reported use of a transvestibular approach for resecting paraurethral leiomyomas. This approach may reduce the risk of urethrovaginal fistula by preserving the vaginal mucosa and offering improved visualization of periurethral structures. Regardless of the approach chosen, meticulous care must be exercised as based on the tumor location. The proximity of it to the bladder neck and internal sphincter or to the mid-urethra, which has an inner smooth muscle longitudinal coat and outer smooth muscle circular coat covered by a horseshoe-shaped external striated sphincter, increases the risk of inadvertent damage [11]. Furthermore, the distal urethra contains the compressor urethra muscle, urethrovaginal sphincter muscle, and bulbocavernosus muscle, all of which should be spared during any surgical procedures [12].
Conclusion
A paraurethral leiomyoma is an uncommon benign tumor derived from smooth muscle with receptors that exhibit some sensitivity to estrogen and may advance gradually. Transvaginal ultrasound and pelvic MRI serve as valuable tools for characterizing any interlabial mass, while cystourethroscopy can be beneficial for excluding other pathologies. Employing a lateral translabial incision is a practical surgical approach for achieving enhanced visualization of the tumor and adjacent tissues, while performing the dissection, care is taken to preserve the vaginal mucosa to reduce the risk of future fistula formation.
REFERENCES
1.
Belis JA, Post GJ, Rochman SC, Milam DF. Genitourinary leiomyomas. Urology 1979;13(4):424–9. [CrossRef]
[Pubmed]

2.
Blaivas JG, Flisser AJ, Bleustein CB, Panagopoulos G. Periurethral masses: Etiology and diagnosis in a large series of women. Obstet Gynecol 2004;103(5 Pt 1):842–7. [CrossRef]
[Pubmed]
3.
Badr MR, Ahmed Higazy AMG, Said Abuelbaga MMR, Mahmoud Mostafa DE. Paraurethral leiomyoma during pregnancy: A case report and review of the literature. Journal of Gynecologic Surgery 2020;36(3):144–6.
4.
Pavlica P, Bartolone A, Gaudiano C, Barozzi L. Female paraurethral leiomyoma: Ultrasonographic and magnetic resonance imaging findings. Acta Radiol 2004;45(7):796–8. [CrossRef]
[Pubmed]
5.
Zuckerman IC, Kershner D, Laytner BD, Hirschl D. Leiomyoma of the kidney. Ann Surg 1947;126(2):220–8.
[Pubmed]
6.
Yusim IE, Neulander EZ, Eidelberg I, Lismer LJ, Kaneti J. Leiomyoma of the genitourinary tract. Scand J Urol Nephrol 2001;35(4):295–9. [CrossRef]
[Pubmed]
7.
Kato T, Kobayashi T, Ikeda R, et al. Urethral leiomyoma expressing estrogen receptors. Int J Urol 2004;11(7):573–5. [CrossRef]
[Pubmed]
8.
Lee MC, Lee SD, Kuo HT, Huang TW. Obstructive leiomyoma of the female urethra: Report of a case. J Urol 1995;153(2):420–1. [CrossRef]
[Pubmed]
9.
Migliari R, Buffardi A, Mosso L. Female paraurethral leiomyoma: Treatment and long-term follow-up. Int Urogynecol J 2015;26(12):1821–5. [CrossRef]
[Pubmed]
10.
Rezai S, Bue SL, Bahl N, Chadee A, Gottimukkala S, Fishman A. A true paraurethral leiomyoma, a case report and review of literature. Obstet Gynecol Int J 2017;6(5):00218.
11.
Faiena I, Koprowski C, Tunuguntla H. Female urethral reconstruction. J Urol 2016;195(3):557–67. [CrossRef]
[Pubmed]
12.
Cardozo L, Staskin D, editors. Anatomy. In: Textbook of Female Urology and Urogynecology: Clinical Perspectives. 5ed. Boca Raton: CRC Press; 2023.
SUPPORTING INFORMATION
Author Contributions
Niloofar Rostaminejad - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nazanin Kianinejad - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Amir Soltani Tehrani - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Farzaneh Sharifiaghdas - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Niloofar Rostaminejad et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}