 |
Case Report
A case report of recurrent ovarian torsion following oocyte cryopreservation managed with dual technique oophoropexy
1 Department of Obstetrics and Gynecology, Division of Reproductive Endocrinology and Infertility at Washington University School of Medicine in St. Louis, Missouri, USA
2 Department of Obstetrics and Gynecology, Division of Minimally Invasive Gynecologic Surgery at Washington University School of Medicine in St. Louis, Missouri, USA
Address correspondence to:
Emily E Spurlin
Washington University in St Louis, 4444 Forest Park Ave, Ste 3100, St. Louis, MO 63108,
USA
Message to Corresponding Author
Article ID: 100174Z08ES2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Spurlin EE, de Souza KM, Keller SL, Ratts VS, Omurtag KR, Jimenez PT. A case report of recurrent ovarian torsion following oocyte cryopreservation managed with dual technique oophoropexy. J Case Rep Images Obstet Gynecol 2024;10(1):43–48.ABSTRACT
Introduction: Ovarian torsion is a known risk of ovarian hyperstimulation done as part of fertility treatments. The purpose of this case report is to describe an unusual case of recurrent ovarian torsion following oocyte cryopreservation that was ultimately managed with ovarian detorsion and dual technique oophoropexy.
Case Report: The patient presented is a 25-yearold female with history of recurrent ovarian torsion who underwent fertility preservation with ovarian cryopreservation in the setting of risk for ovarian loss in the case of recurrent torsion episodes. Following ovarian hyperstimulation and oocyte retrieval, the patient experienced three recurrent episodes of torsion which were surgically managed. On the third episode, a dual technique oophoropexy was performed using both utero-ovarian ligament plication and ovarian fixation.
Conclusion: This case describes an unusual presentation of an uncommon complication of ovarian stimulation. During her surgical management of recurrent ovarian torsion, ovarian conservation was prioritized and a dual oophoropexy technique was utilized which has thus far prevented further recurrent episodes of torsion.
Keywords: Case report, Oophoropexy, Ovarian fixation, Recurrent ovarian torsion, Utero-ovarian plication
Introduction
Ovarian torsion is a gynecologic emergency occurring when the ovary and/or fallopian tube rotates around the infundibular pelvic and the utero-ovarian ligaments. It typically manifests as acute onset abdominal pain and has an estimated annual prevalence of 2–15% among women presenting with such pain [1],[2]. Although ovarian torsion can affect physiologically normal ovaries, it predominately occurs in patients with underlying ovarian pathology or enlarged ovaries following ovarian stimulation cycles [3],[4]. The rotation along the ovarian vascular supply causes tissue hypoxia due to compromised blood flow which triggers intense pain and ultimately necrosis of the affected ovary if not promptly treated.
Definitive diagnosis and treatment of ovarian torsion requires surgical assessment, commonly via laparoscopy [5],[6]. Historically, oophorectomy was the treatment of choice to prevent complications, such as thromboembolism. However current evidence supports a more conservative approach, emphasizing ovarian detorsion with or without cystectomy; this practice has demonstrated the potential to preserve ovarian function without increasing risk for adverse events [6],[7],[8],[9].
Recurrent ovarian torsion is uncommon with a recurrence rate ranging from 2% to 12% [6],[10]. The risk of recurrence may be higher in cases where no underlying adnexal pathology is identified and is often attributed to the laxity of the utero-ovarian ligament [11]. In cases of recurrent torsion, the option of oophoropexy can be considered as a preventative measure against future episodes. Various approaches can be employed for this procedure, such as suturing the ovary to the posterior and anterior abdominal walls or plicating the utero-ovarian ligament [12],[13]. In instances of recurrent episodes, it may be prudent to refer the patient to a reproductive endocrinologist for reproductive counseling, particularly if a prior oophorectomy has been performed.
Here we report a case of recurrent ovarian torsion affecting both ovaries, with one episode necessitating oophorectomy. Due to the ongoing risk of future torsion episodes leading to loss of fertility, the patient underwent oocyte cryopreservation. Unfortunately, her oocyte cryopreservation cycle was complicated by three recurrent episodes of ovarian torsion, prompting the performance of oophoropexy using two distinct techniques, fixation and utero-ovarian ligament plication, as a preventive measure.
Case Report
The patient is a 25-year-old female with a significant medical history of recurrent ovarian torsion. At the age of 9, she experienced her initial episode of ovarian torsion, leading to an emergency surgery resulting in left salpingo-oophorectomy. Three years later at age 12, she had a subsequent episode involving the remaining ovary, which was managed with laparoscopic detorsion preserving the ovary. The following year, at age 13, she underwent an interval surgery with the intention of performing oophoropexy on remaining right ovary. However, during the diagnostic laparoscopy it was observed that the right ovary was secured with adhesive tissue, rendering the oophoropexy unnecessary. Going forward, she had annual follow-up with a pediatric gynecologist and was placed on oral contraceptive pills to suppress follicular development.
Nine years later at age 22, the patient experienced a recurrent episode of ovarian torsion. She underwent urgent laparoscopic detorsion and cyst drainage. Additionally at the time of surgery, an oophoropexy was performed in which the ovary was fixated to the round ligament with 0-vicryl suture. Following this third episode of ovarian torsion, she was counseled by her pediatric gynecologist to consider fertility preservation with oocyte cryopreservation given risk for subsequent episodes which could potentially result in oophorectomy of her remaining right ovary.
At age 25, the patient had a consultation with a reproductive endocrinologist and elected to proceed with oocyte cryopreservation. Laboratory results at that time revealed an anti-mullerian hormone (AMH) level of 2.08 ng/mL. A baseline ultrasound indicated surgically absent left ovary with normal appearing right ovary, measuring 40×16×32 mm with antral follicle count (AFC) of 17.
The patient underwent a long agonist protocol, initiating gonadotropin-releasing hormone (GnRH) agonist in the luteal phase of her proceeding cycle. At baseline testing, her AFC was 25 and estradiol was 12.1 pg/mL. She was initiated on 225 international units (IUs) recombinant follicle-stimulating hormone (rFSH) and the dose of GnRH agonist was decreased. On day three of stimulation, her estradiol rose appropriately to 181.8 pg/mL and menotropin (Menopur) was added for a dosing of 150 IU rFSH and 75 IU Menopur. On stimulation day nine with a peak estradiol of 2125 pg/mL and three follicles greater than 18 mm, she administered 10,000 IU human chorionic gonadotropin (hCG) to trigger final follicular maturation and resumption of meiosis. An ultrasound guided follicle aspiration was performed 36 hours later. A total of nine oocytes were retrieved, out of which seven were mature and cryopreserved.
The patient initially did well following oocyte retrieval. She was seen in the office postoperative day four with nausea and dull abdominal pain. During the examination, there were no concerning findings, and a pelvic ultrasound revealed an enlarged ovary measuring 95×45×88 mm with visible color Doppler flow. The discomfort was attributed to the expected postoperative state, and conservative management was advised with precautions to return with worsening symptoms.
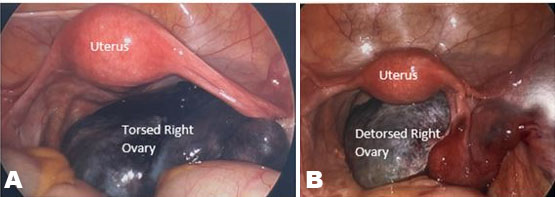
Seventeen days following oocyte retrieval, the patient experienced sudden onset right lower quadrant pain with nausea and vomiting that started after picking up a heavy object. The pain felt similar to her past episodes of torsion. She was advised to go to the emergency department (ED) where an exam was performed with moderate tenderness in the right lower quadrant on abdominal exam and significant right adnexal tenderness and palpable mass on bimanual exam. A transvaginal ultrasound demonstrated an enlarged right ovary measuring 96×73×43 mm without color Doppler flow. She was urgently taken to the operating room. On diagnostic laparoscopy, the right ovary was noted to be edematous, dusky, and twisted three times around the infundibulopelvic (IP) ligament (Figure 1A). The torsion was reduced and color to the ovary was noted to improve (Figure 1B). Upon normalization of anatomy, the prior oophoropexy to the round ligament was not noted to be intact; an expected finding given prior oophoropexy utilized absorbable suture. Considering the degree of ovarian edema at the time of surgery and concerns regarding tissue friability, the decision was made not to perform a repeat oophoropexy during the same procedure. The patient was discharged same day with specific instructions for limited physical activity to minimize the risk of recurrent episodes.
Twenty-four days following oocyte retrieval and seven days following ovarian detorsion, the patient presented to an outside hospital while on vacation with symptoms consistent her prior torsion episodes and underwent an urgent laparoscopic detorsion. Oophoropexy was not performed.
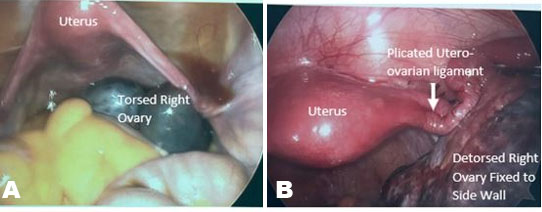
Twenty-nine days following oocyte retrieval, twelve days following first torsion episode, and five days following second torsion episode, the patient once again presented to ED with symptoms consistent with ovarian torsion. She was taken to the operating room (OR) where torsion was confirmed (Figure 2A) and was successfully reduced. Considering the recurrent episodes and the interval decrease in ovarian size and edema, the decision was made to perform oophoropexy. With this assistance of the Minimally Invasive Gynecologic Surgery service at our institution, the right utero-ovarian ligament was plicated using three vertical mattress sutures with 0-silk. Special care was taken to avoid suturing the fallopian tube and following plication, the utero-ovarian length was significantly shortened. In addition, the lateral aspect of the ovary was sutured to the lateral aspect of the right round ligament using 0 V-lock sutures in a running manner (Figure 2B). After completion of the oophoropexy, the ovary demonstrated minimal mobility.
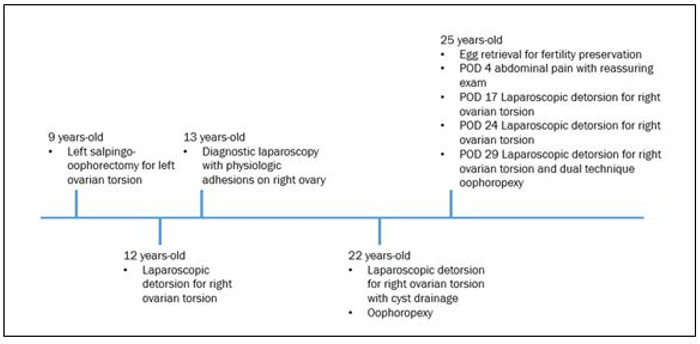
Following recovery from the third laparoscopic detorsion with oophoropexy, the patient experienced an improvement in her pain symptoms and at her final postoperative follow-up visit she expressed satisfaction and gratitude for her care. For a timeline of all torsion episodes, see Figure 3. At the time of publication, over one year following the most recent oophorpexy utilizing a dual technique, she has not experienced any further episodes of ovarian torsion.
Discussion
Ovarian torsion is an uncommon gynecologic emergency, and recurrent episodes of ovarian torsion are even more infrequent. Nevertheless, the implications of recurrent torsion can be devastating, leading to infertility and surgical menopause. Historically, removing the necrotic ovary was the treatment of choice given the questionable viability and possible postoperative complications, namely infection or venous thromboembolism. However, there is now a wide body of literature documenting the feasibility and safety of ovarian conservation in cases of torsion [14],[15],[16].
Potential risk factors for recurrent torsion include younger age specifically <20 years old, and absence of ovarian pathology [10],[17]. These risk factors likely indicate a certain degree of inherent laxity in the suspensory ligaments, which increases the risk for torsion. The management of recurrent ovarian torsion includes various treatment options, including ovarian cystectomy or aspiration, hormonal therapy such as oral contraceptive pills to suppress follicular cyst formation, fixating the ovary with oophoropexy, and discussions regarding fertility preservation [6]. In this case report, all of these approaches were employed.
Oophoropexy is a surgical procedure performed to decrease risk for recurrent ovarian torsion. It typically involves the shortening of the ovarian suspensory ligaments or fixating the ovary to adjacent structures, such as the round ligament, posterior uterine wall, or pelvic side wall. Various materials, including absorbable and non-absorbable sutures, loop suture (EndoLoop), or clips can be used for fixation. It is important to note that while fixation decreases the likelihood of recurrent torsion, it does not completely eliminate the possibility. Previous studies have reported a risk of torsion after oophoropexy as high at 30% [10],[17]. No method of oophoropexy has been found to be superior [17].
In the case presented, the patient was referred to a reproductive endocrinologist specialist for discussion of oocyte cryopreservation for fertility preservation. During the initial consultation, it was acknowledged that ovarian torsion is a rare complication of ovarian stimulation, complicating less than 0.5% of retrievals [18],[19],[20]. However, considering the patient’s history, the risk was expected to be higher. Given her age of 24, an AMH of 2 ng/mL and AFC of 17, a plan was made for a long agonist with close monitoring of follicular development. The patient was given strict torsion precautions and advised to limit activity. At the patient’s last torsion surgery (age 22) prior to ovarian stimulation, oophoropexy was performed with fixation of the ovary to the round ligament with absorbable vicryl suture. Vicryl has a retention period of 28–35 days and absorption rate of 56–70 days, so it logically follows that the prior oophoropexy would have no longer been functional [21]. In this case and in the case where a patient had not previously undergone oophoropexy, prophylactic fixation prior to ovarian stimulation could be considered as an additional preventive measure.
Despite the implemented precautions, the patient experienced three recurrent episodes of torsion following ovarian stimulation. It is possible that the patient would have benefited from oophoropexy at the initial torsion surgery at our institution. However, during the surgery, it was determined that suturing the large, edematous ovary with multiple friable corpus lutea would have posed a substantial bleeding risk and would have been unlikely to be a successful fixation. The second torsion surgery was performed at a small local hospital where the patient was vacationing and oophoropexy was not performed. At the third surgery (second surgery at our center) the post-stimulation edema was significantly less with notable laxity at the utero-ovarian ligament upon de-torsion making oophoropexy using two techniques with utero-ovarian ligament plication and fixation to the sidewall a viable option which was ultimately successful (Figure 2).
Taken together, the presented case highlights an uncommon presentation of a rare complication of ovarian stimulation. Ovarian torsion is a known risk of ovarian stimulation, but experiencing this complication three times within four weeks following retrieval is certainly unusual. However, considering the patient’s history of recurrent torsion, elevated risk was anticipated. Prompt evaluation and timely surgical intervention allowed for the preservation of her remaining ovary. By performing utero-ovarian ligament plication with a permanent suture and fixing the ovary to the lateral side wall, the risk of future torsion episodes is expected to be low. Additionally, with the cryopreservation of seven mature oocytes, the patient has a 56% chance of achieving a live birth should she need to utilize them in the future [22] resulting in an overall favorable outcome for the patient.
Conclusion
Patients with recurrent ovarian torsion are at increased risk of undergoing unilateral or bilateral oophorectomy, which can have significant implications for their future fertility. Therefore, it is important to discuss fertility preservation options, such as oocyte cryopreservation with these patients if they desire future fertility. In cases where patients with recurrent torsion undergo ovarian stimulation and retrieval, there should be a high degree of suspicion for recurrent torsion in the setting of acute postoperative pain. It is crucial to make every effort to preserve the affected ovary during surgery. Considering oophoropexy may be appropriate to decrease the likelihood of future torsion episodes.
REFERENCES
1.
Sasaki KJ, Miller CE. Adnexal torsion: Review of the literature. J Minim Invasive Gynecol 2014;21(2):196–202. [CrossRef]
[Pubmed]

2.
Bouguizane S, Bibi H, Farhat Y, et al. Adnexal torsion: A report of 135 cases. [Article in French]. J Gynecol Obstet Biol Reprod (Paris) 2003;32(6):535–40.
[Pubmed]
3.
Shadinger LL, Andreotti RF, Kurian RL. Preoperative sonographic and clinical characteristics as predictors of ovarian torsion. J Ultrasound Med 2008;27(1):7–13 [CrossRef]
[Pubmed]
4.
Gelbaya TA. Short and long-term risks to women who conceive through in vitro fertilization. Hum Fertil (Camb) 2010;13(1):19–27. [CrossRef]
[Pubmed]
5.
Cohen SB, Oelsner G, Seidman DS, Admon D, Mashiach S, Goldenberg M. Laparoscopic detorsion allows sparing of the twisted ischemic adnexa. J Am Assoc Gynecol Laparosc 1999;6(2):139–43. [CrossRef]
[Pubmed]
6.
Adnexal Torsion in Adolescents: ACOG committee opinion No, 783. Obstet Gynecol 2019;134(2):e56–63. [CrossRef]
[Pubmed]
7.
Shalev E, Bustan M, Yarom I, Peleg D. Recovery of ovarian function after laparoscopic detorsion. Hum Reprod 1995;10(11):2965–6. [CrossRef]
[Pubmed]
8.
Oelsner G, Cohen SB, Soriano D, Admon D, Mashiach S, Carp H. Minimal surgery for the twisted ischaemic adnexa can preserve ovarian function. Hum Reprod 2003;18(12):2599–602. [CrossRef]
[Pubmed]
9.
Oelsner G, Bider D, Goldenberg M, Admon D, Mashiach S. Long-term follow-up of the twisted ischemic adnexa managed by detorsion. Fertil Steril 1993;60(6):976–9. [CrossRef]
[Pubmed]
10.
Bertozzi M, Esposito C, Vella C, et al. Pediatric ovarian torsion and its recurrence: A multicenter study. J Pediatr Adolesc Gynecol 2017;30(3):413–7. [CrossRef]
[Pubmed]
11.
Dasgupta R, Renaud E, Goldin AB, et al. Ovarian torsion in pediatric and adolescent patients: A systematic review. J Pediatr Surg 2018;53(7):1387–91. [CrossRef]
[Pubmed]
12.
Fuchs N, Smorgick N, Tovbin Y, et al. Oophoropexy to prevent adnexal torsion: how, when, and for whom? J Minim Invasive Gynecol 2010;17(2):205–8. [CrossRef]
[Pubmed]
13.
Bertozzi M, Magrini E, Bellucci C, Riccioni S, Appignani A. Recurrent ipsilateral ovarian torsion: Case report and literature review. J Pediatr Adolesc Gynecol 2015;28(6):e197–201. [CrossRef]
[Pubmed]
14.
Santos XM, Cass DL, Dietrich JE. Outcome following detorsion of torsed adnexa in children. J Pediatr Adolesc Gynecol 2015;28(3):136–8. [CrossRef]
[Pubmed]
15.
Shalev J, Goldenberg M, Oelsner G, et al. Treatment of twisted ischemic adnexa by simple detorsion. N Engl J Med 1989;321(8):546.
[Pubmed]
16.
Mandelbaum RS, Smith MB, Violette CJ, et al. Conservative surgery for ovarian torsion in young women: Perioperative complications and national trends. BJOG 2020;127(8):957–65. [CrossRef]
[Pubmed]
17.
Akdam A, Bor N, Fouks Y, et al. Recurrent ovarian torsion: Risk factors and predictors for outcome of oophoropexy. J Minim Invasive Gynecol 2022;29(8):1011–8. [CrossRef]
[Pubmed]
18.
Roest J, Mous HV, Zeilmaker GH, Verhoeff A. The incidence of major clinical complications in a Dutch transport IVF programme. Hum Reprod Update 1996;2(4):345–53. [CrossRef]
[Pubmed]
19.
Govaerts I, Devreker F, Delbaere A, Revelard P, Englert Y. Short-term medical complications of 1500 oocyte retrievals for in vitro fertilization and embryo transfer. Eur J Obstet Gynecol Reprod Biol 1998;77(2):239–43. [CrossRef]
[Pubmed]
20.
Gorkemli H, Camus M, Clasen K. Adnexal torsion after gonadotrophin ovulation induction for IVF or ICSI and its conservative treatment. Arch Gynecol Obstet 2002;267(1):4–6. [CrossRef]
[Pubmed]
21.
Gierek M, Kuśnierz K, Lampe P, et al. Absorbable sutures in general surgery – Review, available materials, and optimum choices. Pol Przegl Chir 2018;90(2):34–37. [CrossRef]
[Pubmed]
22.
Goldman RH, Racowsky C, Farland LV, Munné S, Ribustello L, Fox JH. Predicting the likelihood of live birth for elective oocyte cryopreservation: A counseling tool for physicians and patients. Hum Reprod 2017;32(4):853–9. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Emily E Spurlin - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Katherine M de Souza - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sarah L Keller - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Valerie S Ratts - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kenan R Omurtag - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Patricia T Jimenez - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Emily E Spurlin et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}