 |
Case Report
Primary mucinous adenocarcinoma intestinal type of the vulva arising at site of prior vulvar Crohn’s disease: A case report and review of the literature
1 Cleveland Clinic Akron General Obstetrics and Gynecology, Akron, OH, USA
2 Cleveland Clinic Obstetrics and Gynecology Institute, Cleveland, OH, USA
3 Cleveland Clinic Obstetrics and Gynecology Institute, Section of Gynecologic Oncology, Cleveland, OH, USA
4 Cleveland Clinic Akron General Hematology and Medical Oncology, Akron, OH, USA
5 Cleveland Clinic Akron General Obstetrics and Gynecology, Division of Gynecologic Oncology, Akron, OH, USA
Address correspondence to:
Lisa Rauh-Benoit
MD, MPH, 9500 Euclid Avenue, Cleveland, Ohio 44195,
USA
Message to Corresponding Author
Article ID: 100182Z08SW2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Waldrop S, Dinicu A, Kelley J, Sindel A, Rizzo A, Rauh-Benoit L. Primary mucinous adenocarcinoma intestinal type of the vulva arising at site of prior vulvar Crohn’s disease: A case report and review of the literature. J Case Rep Images Obstet Gynecol 2024;10(2):30–33.ABSTRACT
Introduction: Vulvar mucinous adenocarcinoma is a rare subtype that likely arises from atopic gastrointestinal tissue. The evaluation and treatment of this condition often requires a multidisciplinary approach.
Case Report: Our patient is a 55-year-old female with a history of Crohn’s disease who initially presented with a painless vulvar mass associated with occasional bleeding. Notably, the mass presented at the site of a prior rectovaginal fistula. A vulvar biopsy was performed with pathology consistent with intestinal type mucinous adenocarcinoma. Further workup was notable for imaging showing retroperitoneal and pelvic metastatic lymphadenopathy, hypermetabolic liver and bony metastases, and pulmonary nodules concerning for metastases. Following discussion at tumor board, the patient was recommended treatment with 5-fluorouracil, leucovorin, oxaliplatin (FOLFOX), and bevacizumab. Unfortunately, prior to starting chemotherapy, the patient presented to the emergency department with dizziness and weakness and was found to have brain metastases. She ultimately elected to be discharged home on hospice care.
Conclusion: Vulvar mucinous adenocarcinoma is a rare subtype tumor with limited literature on treatment options. For these rare cases, clinicians can consider treatment modalities for colon carcinomas rather than vulvar carcinomas.
Keywords: Crohn’s disease, Mucinous adenocarcinoma, Vulvar cancer
Introduction
Mucinous adenocarcinoma of the vulva is an extraordinarily rare malignancy with the suspected origin being ectopic intestinal mucosa. In this case report, we will discuss an incidence of mucinous adenocarcinoma of the vulva discovered at the site of previous fistula secondary to Crohn’s disease. Upon review of the limited literature, the majority of vulvar mucinous adenocarcinoma presented as a painless, pruritic mass over the span of one to nine months [1],[2]. This subtype of adenocarcinoma is very rare with few descriptions of management in the literature. In describing this case, we will review the decision to deviate from standard regimens for vulvar cancer. In addition, we will highlight the likely role of Crohn’s disease in the natural history of this cancer [3] .
Case Report
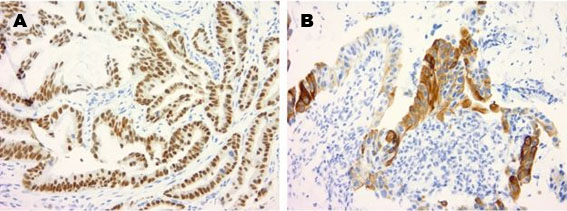
This patient is a 55-year-old female who initially presented to our gynecologic oncology clinic with complaints of a painless right vulvar mass for nearly six months. She endorsed occasional bleeding from the mass but denied any vaginal bleeding or discharge. At the time of presentation, she was asymptomatic. Her past medical history was notable for Crohn’s disease, anxiety, gastroesophageal reflux disease, osteoarthritis, and iron deficiency anemia. She had a remote history of a rectovaginal fistula, a complication of Crohn’s disease that had been repaired. Her family history was positive for breast cancer in her maternal grandmother and colon cancer in her maternal grandfather. At the time of her initial visit, physical exam showed a 5 cm right labial mass with necrotic edges and fungation medially, as well as palpable extension and appearance of necrotic tumor within lower third of the vagina. Of note, the patient reported that this site harbored her prior rectovaginal fistula. The mass appeared to abut the rectum and anus but there was no gross involvement of these structures. The urethra also did not appear involved on exam. Prominent subcentimeter lymph nodes were noted in the right inguinofemoral region, whereas none were palpable in the left inguinal space. A vulvar biopsy was performed, and three samples were obtained, and all three specimens confirmed diagnosis of intestinal type mucinous adenocarcinoma positive for CK20 and CDX2 (Figure 1 and Figure 2).
A colonoscopy and an endoscopy were performed with no abnormal findings. The patient also underwent a magnetic resonance imaging (MRI) of her abdomen and pelvis, which showed prominent inguinal and retroperitoneal lymph nodes concerning for metastatic involvement. Unfortunately, there was a significant delay in the patient following up after the above work-up due to psychosocial issues. When she returned to our clinic three months after her initial visit, carcinoembryonic agent (CEA) was elevated to 81 and carbohydrate antigen (CA) 19-9 was elevated to 124. A positron emission tomography (PET) scan showed a fluorodeoxyglucose (FDG) avid soft tissue mass consistent with known neoplastic process, retroperitoneal and pelvic metastatic lymphadenopathy, hypermetabolic liver and bony metastases, and multiple small pulmonary nodules concerning for metastases. The patient’s case was discussed at tumor board with recommendation for a colorectal chemotherapy regimen and as such was referred to medical oncology given their expertise with these plans. After that consultation, a plan to proceed with a 5-fluorouracil, leucovorin, oxaliplatin (FOLFOX), and bevacizumab and to consider palliative radiation therapy for symptomatic management was made.
Prior to starting chemotherapy, the patient presented to the emergency department with dizziness and weakness, and was found to have a left dorsal cerebellar parenchymal hypodensity and mass effect on non-contrast head computed tomography (CT). An MRI brain was ordered and showed multiple enhancing parenchymal lesions concerning for metastasis, including a 3.5 cm lesion in the left superior cerebellar hemisphere, a 1.6 cm enhancing lesion in the dorsal vermis and a 3 mm lesion in the right orbital frontal region. The patient was admitted for consideration of gamma knife surgery. With multidisciplinary input, the patient ultimately deferred gamma knife surgery and was discharged home with hospice given her rapid decline and concern for toxicity related to radiation.

Discussion
Mucinous adenocarcinoma intestinal type of the vulva is a rare presentation of mucinous adenocarcinoma with limited case studies available. Upon review of 22 case studies, the origin of this rare presentation has been the focal point of discussion. The authors of one of the first reported cases of mucinous adenocarcinoma of the vulva suspected that stray rectal mucosa from a fourth-degree laceration repair may have been a precipitating feature [4]. Others have theorized that a focus of intestinal tissue remains present in the lower vagina due to the division of the cloaca during embryologic development and later undergoes malignant transformation like a primary adenocarcinoma of the colon [2]. It has been further postulated that this phenomenon could be secondary to the predisposition of destruction and inflammatory pathology characteristic of Crohn’s disease laying the foundation malignant growth. While vulvar manifestations of Crohn’s disease are well described, the most malignant transformation is squamous cell in histology unlike the intestinal-type adenocarcinoma described here [5]. We believe this may be the first report with the connection between Crohn’s disease and vulvar mucinous adenocarcinoma. With the rising incidence of Crohn’s disease and fact that 1 in 5 individuals suffering from Crohn’s may develop fistulas and have potential for residual foci of colonic tissue, it is important that providers thoroughly evaluate the vagina and vulva in these women [6]. Given paucity of literature on the topic, average time from vulvar manifestation to cancer cannot be ascertained so careful examination is warranted at regular intervals.
The treatment of early-stage vulvar cancers of usual histology is radical excision with bilateral inguinofemoral lymphadenectomy or sentinel lymph node evaluation. For patients with unresectable but locally advanced tumors, concurrent chemoradiation with cisplatin is standard therapy. However, it is unclear if this approach can be applied to these rare mucinous adenocarcinomas of the vulva. Sui et al. compared the outcomes of four vulvar mucinous adenocarcinoma cases in which patients had first-line therapy for vulvar cancer with radical local excision followed by adjuvant chemotherapy with four cycles of paclitaxel and carboplatin [7]. All four cases had a disease-free period, ranging from 19 to 48 months, after receiving standard treatment [1]. In their case there was no recurrence during the two years of follow-up. Given the early stage of cases reviewed, this report is uninformative for patients with advanced disease at diagnosis.
Kaltenecker et al. presented a patient with vulvar mucinous adenocarcinoma complicated by lung nodules. In this case, mitomycin-c and 5-fluorouracil were chosen for systemic chemotherapy in addition to radiation to the vulva, inguinal nodes, and lung nodules; mitomycin-c and 5-fluorocuracil were chosen due to their known efficacy in primary colorectal cancers. The current standard for primary chemotherapy for metastatic colorectal cancers is 5-fluorouracil, leucovorin, oxaliplatin (FOLFOX) with bevacizumab [8],[9]. In the absence of any significant data, it is reasonable to model treatment paradigms from the management of colorectal cancers rather than typical therapies utilized for usual squamous cell vulvar cancers.
Conclusion
In summary, vulvar mucinous adenocarcinomas of intestinal type are extremely rare but likely related to residual foci of colonic tissue from a prior traumatic or inflammatory event; in this case, likely a prior fistula or vulvar manifestation of Crohn’s disease. To the best of our knowledge, this is the first report of a vulvar mucinous adenocarcinoma as a likely consequence of prior vulvar Crohn’s. As vulvar manifestations, both benign and malignant, are described for women with Crohn’s disease, providers should be aware of this on routine physical exam and consider as part of the differential with any vulvar symptom. These cases benefit from multidisciplinary approach, including input from our medical oncology colleagues, and endoscopic and colonoscopic evaluation should be performed to rule out the vulva as a metastatic site. As these rare tumors arise from the gastrointestinal tract, treatment should mirror that recommended for colorectal cancers rather than squamous cell vulvar carcinomas.
REFERENCES
1.
Sui Y, Zou J, Batchu N, et al. Primary mucinous adenocarcinoma of the vulva: A case report and review of the literature. Mol Clin Oncol 2016;4(4):545–8. [CrossRef]
[Pubmed]

2.
Kaltenecker B, Manos R, McCall M, Sparzak P. Intestinal-type adenocarcinoma of the vulva: A case study. Gynecol Oncol Rep 2019;28:133–5. [CrossRef]
[Pubmed]
3.
Schecter WP, Hirshberg A, Chang DS, et al. Enteric fistulas: Principles of management. J Am Coll Surg 2009;209(4):484–91. [CrossRef]
[Pubmed]
4.
Ghamande SA, Kasznica J, Griffiths CT, Finkler NJ, Hamid AM. Mucinous adenocarcinomas of the vulva. Gynecol Oncol 1995;57(1):117–20. [CrossRef]
[Pubmed]
5.
Shields BE, Richardson C, Arkin L, Kornik R. Vulvar Crohn disease: Diagnostic challenges and approach to therapy. Int J Womens Dermatol 2020;6(5):390–4. [CrossRef]
[Pubmed]
6.
Roda G, Chien Ng S, Kotze PG, et al. Crohn’s disease. Nat Rev Dis Primers 2020;6(1):22. [CrossRef]
[Pubmed]
7.
National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology. Vulvar Cancer Version 1.2023. [Available at: https://www.nccn.org/professionals/physician_gls/pdf/vulvar.pdf]
8.
Mohelnikova-Duchonova B, Melichar B, Soucek P. FOLFOX/FOLFIRI pharmacogenetics: The call for a personalized approach in colorectal cancer therapy. World J Gastroenterol 2014;20(30):10316–30. [CrossRef]
[Pubmed]
9.
National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology. Colon Cancer Version 1.2023. [Available at: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf]
SUPPORTING INFORMATION
Acknowledgments
Tatiana Buhtoiarova, MD for producing and providing pathology images
Author ContributionsSavannah Waldrop - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Andreea Dinicu - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Johanna Kelley - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ariel Sindel - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Anthony Rizzo - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Lisa Rauh-Benoit - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Savannah Waldrop et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}