|
Case Report
Spontaneous uterine rupture at 34 weeks of a woman who has previously received post-cesarean chemotherapy for breast cancer
1 Medical Student, University of Queensland, Medical School, Brisbane, QLD 4006, Australia
2 Department of Emergency Medicine, Rockhampton Hospital, QLD 4700, Australia
3 Department of Obstetrics and Gynaecology, Ipswich Hospital, Ipswich, QLD 4305, Australia
Address correspondence to:
Lilantha Wedisinghe
Ipswich Hospital, Chelmsford Avenue, Ipswich, QLD 4305,
Australia
Message to Corresponding Author
Article ID: 100184Z08JB2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Bhambra J, Peiris SP, Wong C, Wedisinghe L. Spontaneous uterine rupture at 34 weeks of a woman who has previously received post-cesarean chemotherapy for breast cancer. J Case Rep Images Obstet Gynecol 2024;10(2):41–45.ABSTRACT
Introduction: A young and healthy gravida-2 para-1 woman presented to a regional hospital with a spontaneous (pre-labor) uterine rupture at 34 weeks 3 days gestation.
Case Report: She had undergone multi-agent chemotherapy for breast cancer, two weeks after her first cesarean delivery four years prior. No known causative factor for uterine rupture other than having an uncomplicated cesarean section was found.
Conclusion: This case report considers whether the effects of chemotherapy on the wound healing process might have contributed to an increased risk for uterine rupture.
Keywords: Cesarean section, Chemotherapy, Spontaneous, Uterine rupture
Introduction
Uterine rupture is a rare but potentially catastrophic complication of pregnancy, characterized by a broad, full-thickness (perimetrium, myometrium, and endometrium) separation of the uterine wall during pregnancy or delivery leading to changes in maternal or fetal status. The worldwide incidence of uterine rupture in all women is estimated to be around 1 per 1000; uterine rupture is most common in women with a history of previous cesarean section delivery with an incidence estimated to be as high as 1 in 100 [1],[2]. Data on the prevalence of spontaneous uterine rupture is not clear. This report details a case of spontaneous rupture in a multigravida woman with a previous history of a single elective cesarean section at 32 weeks gestation, and triple negative breast cancer treated with mastectomy, chemotherapy, radiation, and Goserelin. In particular, this report discusses the potential effects of chemotherapy on scar formation and explore whether this may increase the risk of uterine rupture.
Case Report
Presentation
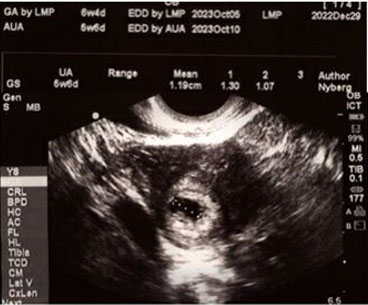
A gravida-2, para-1 woman in her early 30s presented to the obstetrics unit of a regional hospital due to severe intermittent lower abdominal pain at 34 weeks 3 days gestation with an otherwise uncomplicated antenatal course. The patient was a working professional, had received routine antenatal care, and had a supportive partner throughout the pregnancy. Her obstetric history is significant for a previous, uncomplicated, elective lower uterine segment cesarean section (LUSCS) at 32 weeks gestation four years prior due to an antenatal diagnosis of invasive triple negative right breast cancer, diagnosed at 28 weeks gestation, which resulted in delivery of a healthy baby boy.
The patient presented to the obstetrics department with a 13 hour history of severe intermittent abdominal pain which started at 1 AM, waking her from sleep. At 2 PM, she presented to the obstetric department of a private hospital upon prompting by a midwife, who conducted a cardiotocographic (CTG) trace, and was reviewed by her private obstetrician who excluded any sinister pathology including pre-term labor. As the pain did not improve, the patient re-presented to her local public hospital at 4 PM and was reviewed by a Resident Medical Officer (RMO) who noted that the patient was in obvious pain; her vitals were stable and within normal limits; fetal movements were felt; and a repeat CTG showed no signs of fetal distress. The patient denied any episodes of dizziness or change in vision, with her only complaint being abdominal pain. On physical exam, mild generalized tenderness of the abdomen was noted as well as a herniation in the left lower quadrant (LLQ). This was reducible with gentle pressure and resulted in a significant reduction of the patients’ symptoms. The previous LUSCS scar was mild to moderately tender on palpation. Speculum examination revealed a long, closed cervix. At this time the differential diagnosis made by the RMO was uterine rupture versus herniation of abdominal contents, and a Consultant Obstetrician was asked to review the patient.
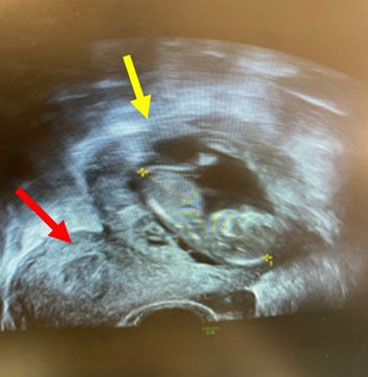
Two consultants promptly reviewed the patient and conducted an ultrasound scan, the findings of which were concerning for a uterine rupture. The decision was made to take the patient to theater for an emergency LUSCS under general anesthesia.
Four years prior to this event, the patient underwent treatment for triple negative breast cancer, which had been diagnosed 28 weeks into her first pregnancy. After her elective LUSCS at 32 weeks gestation, the patient was started on Zoladex (Goserelin) in an attempt to preserve ovarian follicles in preparation for eradicative cancer treatment. Approximately two weeks post-LUSCS she was started on a chemotherapeutic course comprising of carboplatin every three weeks and paclitaxel every week for four cycles. This was followed by regime of Adriamycin and Cytoxan (Doxorubicin and Cyclophosphamide) for four cycles (May–July) followed with weekly injections of Neulasta (Pegfilgrastim), a granulocyte colony-stimulating factor analogue. Bilateral mastectomy with right axillary node dissection and left sentinel node biopsy was undertaken two months later (October, four years prior to uterine rupture) with good margins and no nodal involvement. A Deep Inferior Epigastric Perforator flap reconstruction was also undertaken at the time; this was complicated post-operatively by a surgical site infection which was adequately treated with antibiotics. Lastly, the patient’s cancer treatment was completed with adjuvant radiation of 25 fractions to the right breast. The patient remains in remission to this day.
Management
The abdomen was opened though a Pfannenstiel incision. On entering the peritoneum intact membranes were noted bulging through a full-thickness defect of the anterior-lower uterine segment, which extended from the right uterine angle to the left (the full length of the previous scar) which extended 5 cm inferiorly. The left uterine artery was found 1 mm lateral to this angle extension. The left broad ligament was torn out in its full length. The fetal head within intact membranes was protruding through the defect. There was no involvement of the posterior wall of the uterus, the bladder or the bowel. While a small hemoperitoneum was evident, no major arterial bleeder was found. A live infant was delivered, a healthy baby girl at 2165 g with clear liquor (2 L were measured suggesting polyhydramnios) and APGAR scores of 6 and 9 (at 1 minute and 5 minutes of life respectively). The placenta was delivered and appeared normal (posterior and fundal in location) with no signs of placental abruption. Umbilical cord blood gas results were within normal limits. The uterine cavity was checked and was empty. Uterus was exteriorized and inspected. It was found to be otherwise unremarkable with normal tubes and ovaries. Carbetocin and Ergometrine were given to aid in hemostasis and the uterus was closed in two layers after securing the uterine angles. The left broad ligament tear was repaired with 2-0 vicryl. Hemostasis was achieved. Misoprostol 1 mg was also administered rectally during which the uterus was found to be well contracted. Total measured blood loss was 1 L.
Two days post-operation the patient was feeling well with minimal bleeding per vagina. Her pain was well controlled, and she was eager to be discharged to see her new baby girl (who had been transferred to a tertiary center for additional care, mainly due to prematurity). She was mobilizing well, and examination revealed a firm central uterus at approximately 1 cm above the umbilicus. Vital signs were within normal limits and the surgical site was clean. The consultant debriefed the patient. The patient was thankful that the team had saved both her and her baby girl. The patient was discharged 40 hours post-operatively on a 10-day course of subcutaneous Enoxaparin 40 mg/d.
Discussion
Uterine rupture is a rare but potentially catastrophic obstetric complication which requires prompt identification and urgent management to prevent both maternal and neonatal mortality. The majority of cases of uterine rupture occur in women who elect to have Vaginal Births After Caesarean (VBAC). While equally catastrophic, the entity of spontaneous uterine rupture, which occurs outside the confines of labor, poses a greater clinical challenge for prompt identification and management and necessitates a high degree of clinical suspicion with severe abdominal pain often being the only consistent clinical manifestation. Identification of at-risk populations could be beneficial in prompt diagnosis and management of spontaneous uterine rupture.
There were several aspects of this patient’s presentation and previous medical history that likely contributed to her uterine rupture. It is well documented that the most significant risk factor for uterine rupture is a history of previous cesarean delivery owing to the presence of a scarred uterus which can be an area of weakness during increased uterine wall pressures (i.e., labor and associated uterine contractions). The fact that the patient’s previous pre-term cesarean delivery was at 32 weeks and likely had a less developed lower uterine segment versus at term could have potentially been a contributing risk factor for scar dehiscence or uterine rupture. Data on the significance of a previous pre-term LUSCS is sparse but does not appear to be significant factor [3]. It is possible that this patient may have been in very early labor. Her initial intermittent cramping could have been a sign of mild uterine contractions. However, on examination the patient’s cervix was found to be long and closed which clinically excluded established pre-term labor. Alternatively, cramping could also occur secondary to bleeding from scar rupture. Furthermore, the presence of an over-distended uterus, which in this case had a high likelihood given the suspected polyhydramnios at time of delivery, may further add to increased pressures on a compromised uterine wall and reduced the threshold needed for rupture to occur. Lastly, it is possible that in women receiving chemotherapy the associated immunosuppression could potentially impair wound healing, resulting in a weaker uterine scar, thereby further increasing the risk of uterine rupture post-cancer treatment.
It is thought that among the oncological population, chemotherapy may negatively impact wound healing through multiple different mechanisms, which can be summarized as impairment of the patient’s immune system leading to delayed wound healing [4],[5]. In animal studies, alkylating agents such as cisplatin and cyclophosphamide have been demonstrated to decrease the tensile strength of surgical wounds particularly during the early proliferative phases [6]. Adriamycin (Doxorubicin) has also been demonstrated to be cytotoxic to thrombocytes, leukocytes, fibroblasts, and monocytes resulting in decreased collagen synthesis and delayed wound healing in mice. A similar finding was demonstrated in a group of rats given doxorubicin postoperatively with decreased tensile strength of surgical wounds [7].
While animal studies have shown impaired effects on wound healing related to chemotherapy administration, these effects have not been directly tested in humans due to ethical reasons and observational studies that have occurred retrospectively have not demonstrated any significant difference in wound complications owing to these therapeutic agents. A study noted that there was no difference in the incidence of wound complications between patients who received postoperative chemotherapy and those who did not in the treatment of ovarian cancer [8]. Similarly, a retrospective study demonstrated that there was no difference in wound complications between patients receiving postoperative adjuvant chemotherapy and those that did not after mastectomy and immediate breast reconstruction [9]. One study commented on the effects of total body and pelvic radiation during childhood cancer treatment on uterine function (particularly infertility) but did not mention uterine rupture as a complication. Additionally, the study did not identify reports of uterine damage after chemotherapy [10].
As of the time of writing of this case study, the reviewed literature has not explored the effects of chemotherapy or Goserelin on cesarean scar formation or rates of uterine rupture post-chemotherapy. Therefore, the effect of these agents causing uterine scar dehiscence is only presumptive.
Conclusion
Spontaneous uterine rupture is a difficult entity to diagnose and anticipate, compared with intrapartum uterine rupture, and requires a high index clinical suspicion. Immunocompromised states which may lead to impaired wound healing after cesarean sections may be a potential risk factor for subsequent uterine rupture. Research is needed to ascertain the effects of chemotherapy immediately post-cesarean section on cesarean scar healing as well as being a risk factor for spontaneous uterine rupture.
Patient’s perspective
Firstly, I’d like to thank the doctors and other medical staff for their quick response when my condition was discovered. I am very grateful that both myself and my baby are healthy and recovering, as the circumstances could have been much dire. I appreciate that the doctors at the Base Hospital took my concerns and comments about the pain I was experiencing seriously and did not “brush off” the pain as ligament stretching, as other medical staff in different medical centers did. The pain I felt was very intense, coming in waves and located in one spot—I knew it was something more than ligament stretching as paracetamol or heat packs did not help. It was difficult to walk and stand straight when I was feeling the pain. I’d like to see further research of the effects of chemotherapy and reconstructive surgery on mothers wishing to fall pregnant after a cancer diagnosis. Breast cancer is commonly seen as an “old person’s disease” and there seems to be a lack of research into people who are diagnosed at a young age and the consequences that follow this. Again, thank you to the nursing, doctors, and hospital staff who assisted in saving both myself and my baby’s life.
Ethics approval and consent to participate
The patient has seen the manuscript and has given her informed, written consent for this publication.
REFERENCES
1.
Hofmeyr GJ, Say L, Gülmezoglu AM. WHO systematic review of maternal mortality and morbidity: The prevalence of uterine rupture. BJOG 2005;112(9):1221–8. [CrossRef]
[Pubmed]

2.
Guiliano M, Closset E, Therby D, LeGoueff F, Deruelle P, Subtil D. Signs, symptoms and complications of complete and partial uterine ruptures during pregnancy and delivery. Eur J Obstet Gynecol Reprod Biol 2014;179:130–4. [CrossRef]
[Pubmed]
3.
Al-Zirqi I, Daltveit AK, Forsén L, Stray-Pedersen B, Vangen S. Risk factors for complete uterine rupture. Am J Obstet Gynecol 2017;216(2):165.e1–8. [CrossRef]
[Pubmed]
4.
Payne WG, Naidu DK, Wheeler CK, et al. Wound healing in patients with cancer. Eplasty 2008;8:e9.
[Pubmed]
5.
Deptula M, Zielinski J, Wardowska A, Pikula M. Wound healing complications in oncological patients: Perspectives for cellular therapy. Postepy Dermatol Alergol 2019;36(2):139–46. [CrossRef]
[Pubmed]
6.
Gulcelik MA, Dinc S, Gulcelik NE, et al. Optimal timing for surgery after adriamycin treatment in rats. Surg Today. 2004;34(12):1031–4. [CrossRef]
[Pubmed]
7.
Morishita T, Toriyama K, Takanari K, et al. <Editors' Choice> Effect of postoperative doxorubicin administration on ischemic wound healing. Nagoya J Med Sci 2018;80(3):357–66. [CrossRef]
[Pubmed]
8.
Kolb BA, Buller RE, Connor JP, DiSaia PJ, Berman ML. Effects of early postoperative chemotherapy on wound healing. Obstet Gynecol 1992;79(6):988-92.
[Pubmed]
9.
Furey PC, Macgillivray DC, Castiglione CL, Allen L. Wound complications in patients receiving adjuvant chemotherapy after mastectomy and immediate breast reconstruction for breast cancer. J Surg Oncol 1994;55(3):194–7. [CrossRef]
[Pubmed]
10.
Critchley HOD, Wallace WHB. Impact of cancer treatment on uterine function. J Natl Cancer Inst Monogr 2005;(34):64–8. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
We thank the patient for giving her consent and for taking time to write her perspective.
Author ContributionsJaspreet Bhambra - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Shashika Prabuddhani Peiris - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Curtis Wong - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Lilantha Wedisinghe - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Jaspreet Bhambra et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.