 |
Case Report
Surgical management of 12-year-old with complete septate uterus with duplicated cervices and obstructed left hemivagina: A case report
1 Associate Professor, Department of Obstetrics and Gynecology, University of Michigan, Ann Arbor, MI, USA
2 Assistant Professor, Department of Obstetrics and Gynecology, University of Wisconsin, Madison, WI; Fellow, Department of Obstetrics and Gynecology, University of Michigan, Ann Arbor, MI, USA
3 Professor, Department of Obstetrics and Gynecology, University of Michigan, Ann Arbor, MI, USA
Address correspondence to:
Monica W Rosen
MD, Department of Obstetrics and Gynecology, University of Michigan, 1500 E. Medical Center Dr., Ann Arbor, MI 48109,
USA
Message to Corresponding Author
Article ID: 100185Z08MR2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Rosen MW, O’Brien K, Ferrell E, Randolph JF. Surgical management of 12-year-old with complete septate uterus with duplicated cervices and obstructed left hemivagina: A case report. J Case Rep Images Obstet Gynecol 2024;10(2):46–49.ABSTRACT
Introduction: When a patient with an obstructed hemivagina presents in childhood, either hormonal suppression or a staged procedure is proposed for management of the obstruction.
Case Report: This case report is a 12-year-old patient presenting for evaluation of hematocolpos with a complete septate uterus, duplicate cervices, bilateral kidneys, and obstructed left hemivagina who was surgically managed with a complete vaginal septum resection and hysteroscopic metroplasty in one procedure shortly after diagnosis.
Conclusion: This anomaly is not only rare, and the first presented in the literature, but it also importantly demonstrates that if desired by the family after a consideration of benefits and risks, resection of both vaginal and uterine septa can be safely performed in a young post-menarchal patient without the need for a staged procedure later in life.
Keywords: Hysteroscopic metroplasty, Obstructed hemivagina, Utero-cervical septum, Vaginal septum resection
Introduction
Obstructive uterine and vaginal anomalies include imperforate hymen, transverse vaginal septum, obstructed hemivagina, vaginal or cervical atresia or aplasia, and other variants. Historically, obstructive anomalies have been identified at the time of anticipated puberty when hematocolpos, hematometra, or both are discovered in girls with primary amenorrhea. However, advancements in prenatal ultrasonography and screening for congenital anomalies have led to earlier detection. Identification of an obstructive Müllerian anomaly should prompt a urinary system assessment; due to a shared embryonic origin of intermediate mesoderm, genital tract malformations are associated with renal abnormalities in up to 38% of individuals [1].
While obstructive anomalies typically require surgical intervention, there is often a role for hormonal suppression of menses. Menstrual suppression is frequently used to manage symptoms until surgery can be performed or to delay the initial surgery for various reasons. For young adolescents, this may allow more time for the vaginal mucosa to be exposed to estrogen and for growth of the vagina and vulva—thereby requiring a less technically challenging surgery and preventing postoperative vaginal strictures due to a hypoestrogenic state. Alternatively, after a detailed discussion, patients and families may wish to avoid hormonal medications and instead proceed directly to surgery.
Septate uterus is one of the nine categories of uterine anomalies defined by the American Society for Reproductive Medicine (ASRM) Müllerian Anomalies Classification 2021 (MAC2021) [2]. This guide elaborates on treatment options when a vaginal component with obstruction is present, including various combinations of hormone suppression and vaginal dilation, and the addition of surgical management to further address the uterine aspect of the anomaly. Traditional recommendations include hysteroscopic metroplasty with septum resection in those who desire childbearing to reduce risks of miscarriage, preterm birth, and malpresentation [3]. This practice has been challenged in studies like the TRUST trial, which argues against surgical intervention and claims similar outcomes in live birth rate with expectant management [4].
We review a 12-year-old patient with hematocolpos and a complete septate uterus with duplicated cervices and obstructed left hemivagina but absent renal anomalies, who was successfully managed with surgical intervention shortly after diagnosis.
Case Report
A 12-year-old nulligravida presented to her pediatrician for a scoliosis evaluation in June 2022. A magnetic resonance imaging (MRI) workup mentioned a cystic structure that was only partially imaged, measuring approximately 6 cm and located 51 mm to the left of the midline. It appeared to be possibly within the superior vagina near the junction with the cervix. The patient noted that for six months she had been experiencing cyclical monthly cramps lasting a few days each, which resolved without medication and did not interfere with her school activities. At this point, she had not experienced any vaginal bleeding.
A subsequent pelvic ultrasound reported two endometrial canals which were visualized within the uterus and separated by a thick septum which tapered distally. The fundal contour was normal. The uterus was of normal size, measuring 6.9 cm × 3 cm × 4.9 cm. The vaginal canal was mildly distended with hypoechoic and heterogeneous fluid. About one week later, she experienced menarche with light vaginal spotting.
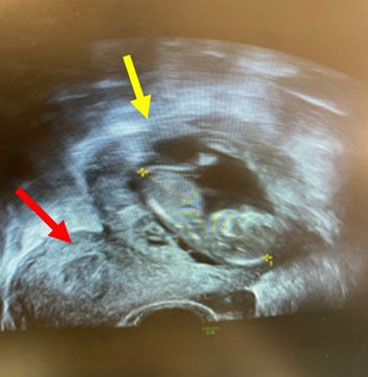
Next, a pelvic MRI revealed a complete septated uterus. A small amount of fluid was noticed within both endometrium, which did not appear dilated. The longitudinal septum of the uterus appeared to extend through the cervix and vagina. The right hemivagina was collapsed with a small amount of fluid centrally and the left hemivagina was dilated with fluid/blood product. The fluid-filled left vagina measured 4.0 cm transverse. The fluid-filled left hemivagina extended at least to the lower third suggesting a possible transverse septum on the left with resultant hematocolpos. This fluid-filled left hemivagina caused mild mass effect on the adjacent rectum with some rectal displacement to the right (Figure 1). Both right and left kidneys were seen.
The diagnosis was hematocolpos, with her anomaly classified as complete septate uterus with duplicated cervices and obstructed left hemivagina per the MAC2021. Management options discussed with the patient and her family included surgery to relieve her vaginal obstruction versus suppressing menses with hormonal medications and delaying surgical management. She was offered consultation with a reproductive specialist to discuss optimal management of her complete uterine septum, including attempting pregnancy without resection and the associated risks. She and her family opted for surgical resection with concurrent removal of both the vaginal and uterine septum.
Two months later, she underwent a complete vaginal septum resection with hysteroscopic metroplasty and preservation of the cervical septum.
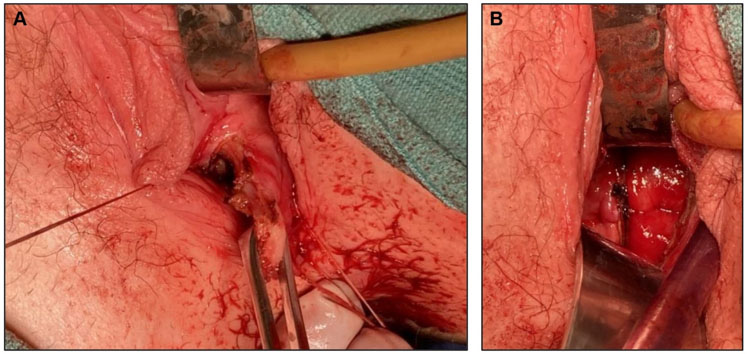
An intraoperative vaginal examination noted a normal-appearing right cervix with a left oblique vaginal septum extending from the right cervix to 3 cm proximal to the hymen. Three stay sutures of 3-0 Vicryl were placed on traction in a triangle directly into the oblique vaginal septum. A #11 scalpel was used to make a stab incision between the stay sutures to drain the hematocolpos. Approximately 200 cc of old blood were evacuated from the obstructed left hemivagina. The Ligasure Maryland device was then used to completely resect the vaginal septum, after which a left cervix was identified without evidence of epithelialization.
Next, a hysteroscope was introduced—first into the right cervix, then into the left cervix. There was no obvious evidence of a fenestration at any point in the utero-cervical septum, which appeared to be complete, extending from the midline septation between the two cervices to the uterine fundus. An 8 French pediatric Foley catheter balloon was inserted into the right uterine cavity and inflated under direct visualization, with the hysteroscope in the left uterine cavity to allow for incision planning. The catheter was inflated with 3 cc of sterile saline. The Twizzle tip hysteroscopic device was used to incise the septum over the distension from the Foley balloon, in the lower portion of the cavity just above the level of the internal os, until the balloon was visualized in the right cavity. The balloon was deflated and removed, and the remaining portion of the uterine septum was sequentially taken down with the Twizzle device (Figure 2).
The procedure was completed in an outpatient setting, and the patient was discharged on the day of her procedure without incident. At her 10-day postoperative visit, she was healing well, without pain and with minimal vaginal bleeding.
Verbal assent from the patient and written consent from her parents for her information to be included in this case report were obtained by the authors. Institutional review board review was not required by our institution, as all information was obtained during standard clinical care.

Discussion
This case details the rare presentation of a 12-year-old with hematocolpos and a complete septate uterus with duplicated cervices and obstructed left hemivagina in the absence of a renal anomaly—likely a variant of obstructed hemivagina with ipsilateral renal anomaly (OHVIRA), or Herlyn–Werner–Wunderlich syndrome. Obstructed hemivagina with ipsilateral renal anomaly may present with various uterine and renal anomalies, but most commonly with a uterus didelphys, a unilateral obstructed hemivagina with hematocolpos, and ipsilateral renal agenesis. In a case series from 2006, only 3/27 patients identified with OHVIRA did not have a urologic anomaly [5]. Furthermore, our patient’s unique variant of an oblique vaginal septum, complete septate uterus, and absence of renal anomalies has never, to our knowledge, been reported.
Management options for an obstructed hemivagina with hematocolpos include surgical intervention or menstrual suppression; however, full suppression can be difficult to achieve, with the possibility of breakthrough bleeding, persistent dysmenorrhea, or development of endometriosis secondary to retrograde menstruation due to the obstruction [5]. For those wishing to avoid using exogenous hormones, vaginal septum excision may be offered at the time of diagnosis. Limitations of performing surgery at such a young age include the potential for emotional trauma and decreased visualization due to a smaller vaginal opening.
This case details a single-staged approach for surgical treatment of both an obstructed hemivagina and a complete uterine septum in a child. Typically, when a patient with an obstructed hemivagina presents in childhood, a staged procedure is proposed for management of the obstruction [6] . This involves the resection of a window of tissue from the vaginal septum in childhood to relieve the obstruction, with a planned second procedure in adolescence for resection of the remaining vaginal septum and, if applicable, the uterine septum. Our case demonstrates that a 12-year-old can successfully undergo a vaginal septum resection with a hysteroscopic metroplasty, without risk of vaginal stenosis and re-obstruction.
Recent debate has questioned whether uterine septum resection is necessary without an infertility diagnosis or prior pregnancy loss, as the live birth rate may be similar without the procedure. For patients without these diagnoses, ASRM recommends offering uterine septum resection following a discussion regarding potential risks and benefits of the procedure [7]. Our patient and her family desired to complete both vaginal and uterine procedures in one setting instead of her potentially returning for a future additional surgery.
Conclusion
This unique anomaly is not only, to our knowledge, the first of its kind to be presented, it also demonstrates the important principle that complete resection can be performed in a young child post-menarche, without need for a staged procedure later in life. Given controversies surrounding the definition of a septate uterus in the TRUST trial, more studies are needed to better quantify the possible adverse effects of a septum on pregnancy and childbirth. Joint decision-making and respect for patient autonomy regarding fertility goals and options should be utilized when planning management of this anomaly.
REFERENCES
1.
Patel V, Gomez-Lobo V. Obstructive anomalies of the gynecologic tract. Curr Opin Obstet Gynecol 2016;28(5):339–44. [CrossRef]
[Pubmed]

2.
Pfeifer SM, Attaran M, Goldstein J, et al. ASRM Müllerian anomalies classification 2021. Fertil Steril 2021;116(5):1238–52. [CrossRef]
[Pubmed]
3.
Zlopasa G, Skrablin S, Kalafatić D, Banović V, Lesin J. Uterine anomalies and pregnancy outcome following resectoscope metroplasty. Int J Gynaecol Obstet 2007;98(2):129–33. [CrossRef]
[Pubmed]
4.
Rikken JFW, Kowalik CR, Emanuel MH, et al. The randomised uterine septum transsection trial (TRUST): Design and protocol. BMC Womens Health 2018;18(1):163. [CrossRef]
[Pubmed]
5.
Sack BS, Speck KE, Hryhorczuk AL, et al. An interdisciplinary approach to Müllerian outflow tract obstruction associated with cloacal malformation and cloacal exstrophy. J Clin Med 2022;11(15):4408. [CrossRef]
[Pubmed]
6.
Smith NA, Laufer MR. Obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome: Management and follow-up. Fertil Steril 2007;87(4):918–22. [CrossRef]
[Pubmed]
7.
Practice Committee of the American Society for Reproductive Medicine. Electronic address: ASRM@asrm.org; Practice Committee of the American Society for Reproductive Medicine. Uterine septum: A guideline. Fertil Steril 2016;106(3):530–40. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Monica W Rosen - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Katie O’Brien - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Emily Ferrell - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
John F Randolph - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Monica W Rosen et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}