 |
Case Report
Natural evolution of a cesarean scar pregnancy up to 34 weeks complicated by an early subserosal uterine rupture and placenta accreta spectrum disorders
1 Department of Medicine, Cheikh Anta Diop University of Dakar, Senegal
2 Department of Obstetrics and Gynecology, Dalal Jamm National Hospital Center, Dakar, Senegal
Address correspondence to:
Mame Diarra Ndiaye
Cheikh Anta Diop University of Dakar – Dalal Jamm National Hospital Center,
Senegal
Message to Corresponding Author
Article ID: 100187Z08MN2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Ndiaye MD, Sall NR, Niass A, Gueye M, Moreira PM. Natural evolution of a cesarean scar pregnancy up to 34 weeks complicated by an early subserosal uterine rupture and placenta accreta spectrum disorders. J Case Rep Images Obstet Gynecol 2024;10(2):54–57.ABSTRACT
Cesarean scar pregnancy (CSP) is an extremely rare form of ectopic pregnancy. A 39-year-old woman with a history of multiple uterine surgeries was diagnosed with a CSP at seven weeks by transvaginal ultrasound. The CSP was misdiagnosed at 13 weeks and 5 days during a second medical opinion. At 22 weeks of gestation, a 3.8 cm subserosal uterine rupture was visualized. Expectant management was decided. A live birth was achieved through an elective cesarean section at 34 weeks of gestation. The complications were early subserosal uterine rupture and placenta accreta spectrum that led to a hysterectomy. Due to risk of uterine rupture, management should consist of early termination of the pregnancy.
Keywords: Placenta accreta, Pregnancy, Cesarean section, Uterine rupture
Introduction
Cesarean scar pregnancy (CSP) is an extremely rare form of ectopic pregnancy. There is no clear guideline regarding management. However, early termination of pregnancy is often performed. Some authors have described cases progressing to the third trimester. Reported complications include premature delivery and placenta accreta spectrum disorders.
Objectives
We report this case because it highlights a previously unreported complication of CSP, which is uterine rupture in the second trimester of pregnancy. Discovery at this age makes the decision difficult due to the viability of the fetus.
Case Report
Patient information
The patient was a 39-year-old woman, gravida 4, para 3. Surgical history
- Myomectomy in 2010
- Three cesarean sections in 2011, 2025, and 2017.
First trimester
After ultrasonography, a practitioner concluded to an ectopic cesarean scar pregnancy (CSP) at seven weeks’ gestation. Pregnancy termination was suggested. She sought a second medical opinion at 13-week day 5. The second obstetrician concluded to an evolutive intrauterine pregnancy and provided obstetrical follow-up.
Clinical findings and diagnostic assessment 22 weeks
The patient was referred for a morphological ultrasound. We noted a discontinuity of the myometrium adjacent to the bladder (Figure 1) measuring 3.8 mm. The amniotic membrane was in contact with the uterine serosa. Additionally, there was a posterior placenta previa. The amniotic fluid volume was normal, and the fetus was eutrophic with an estimated weight of 501 g (48th percentile). No morphological abnormalities were detected. No other complications of the pregnancy were noted. The patient was informed and immediately admitted in unit care.
Therapeutic intervention and timeline
Due to the fetal viability and the parents’ choice, the medical team decided on expectant management in unit care.
24 weeks
The medical team recommendations included a daily home monitoring by a midwife, wearing of a maternity belt, a complete bed rest, and weekly ultrasound follow-up at the hospital.
Obstetrical complications were a gestational diabetes mellitus (fasting glucose: 1.69 g/L, 1-hour glucose: 2.79 g/L, 2-hour glucose: 2.9 g/L) and isolated high blood pressure.
29 weeks
The uterine rupture measured 5 cm, and the amniotic fluid volume was normal. The estimated fetal weight was at the 99th percentile according to intergrowth 21st standards. Antenatal corticosteroids were administered.
Follow-up and outcome
Elective cesarean section at 34 weeks
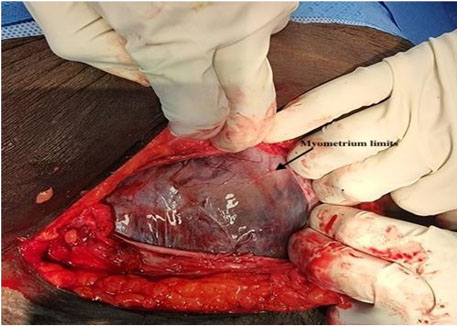
The delivery by elective cesarean section was scheduled at 34 weeks. The uterine rupture measured 7.6 cm. It was performed by two obstetricians’ seniors and a urologist. After a careful incision of the fascia, we observed the serosa and the amniotic membrane (Figure 2). Following the opening of the amniotic membrane, the fetus was delivered. The male newborn weighed 2740 grams (96th percentile) with an Apgar score of 9/10 and no morphological anomalies.
During the procedure we diagnosed a placenta accreta spectrum disorder, involving the bladder. Uncontrollable hemorrhage necessitated a hysterectomy. The urologist performed hemostasis on the bladder. Blood loss was 1150 mL. Hospitalization duration for the patient and her baby was five days. Postpartum follow-up continued until 2 months and 11 days.

Discussion
Cesarean scar pregnancy (CSP) is a rare but increasingly reported condition due to rising cesarean section rates. Its prevalence is approximately 1:2226 (0.04%) of pregnancies [1] and 6.1% of ectopic pregnancies [2]. Cesarean scar pregnancy is a potentially life-threatening condition, which underscores its significance in modern obstetrics.
In this case, diagnosis was made at seven weeks by ultrasound. Cesarean scar pregnancy is often asymptomatic; when symptoms do occur, they are nonspecific and include metrorrhagia and pelvic pain. The average gestational age at occurrence is 7.5 ± 2.5 weeks according to some authors.
According to Zhang et al. [3], early CSP is frequently misdiagnosed as normal intrauterine pregnancy and other obstetrical conditions. According to Pedraszewskii et al. [1], in advanced pregnancies beyond 12 weeks, transabdominal ultrasound produces images that are difficult to interpret, making diagnosis more challenging than in early pregnancy. According to Hameed et al. [2], diagnosis is primarily made by ultrasound. Unlike intrauterine pregnancy, CSP is located below the midsagittal line of the uterus, with the gestational sac embedded in the uterine scar and the uterine cavity empty [4].
In this presented case, a diagnostic error at 13 weeks led to simple monitoring of the pregnancy until 22 weeks of gestation. The consequence was an early uterine rupture at 22 weeks, the threshold of fetal viability. This situation presents an ethical dilemma between maternal risk and fetal viability. Indeed, there is an intrinsic risk of complete uterine rupture, hysterectomy [5], placenta accreta spectrum disorders [6], and bladder invasion [7]. Moreover, a systematic review by Silva reports 48.1% of preterm deliveries in cases of expectant management [6]. The uncertain prognosis and fetal viability led us to adopt expectant management. This approach required significant human resources and resulted in a hysterectomy. Whatever a live birth delivery was obtained.
Generally, pregnancy termination by various methods is accepted. These methods include the use of methotrexate, high-intensity focused ultrasound (HIFU), uterine artery embolization, and surgical treatment via hysteroscopy [1],[2].
Natural evolution of CSP can lead to a large uterine rupture at second trimester. To our knowledge, this is the first article to describe early subserosal uterine rupture as a complication of pregnancy in a scarred uterus. Although there are no established guidelines for managing CSP, the possibility of uterine rupture in the second trimester supports the consideration of pregnancy termination in the first trimester.
The expectant management leads also to placenta accreta spectrum disorder and hysterectomy.
A live birth can be obtained with expectant management.
Conclusion
We reported an unprecedented case of subserosal uterine rupture in the second trimester, complicating a cesarean scar pregnancy. The viability of the fetus and the severity of the diagnosis present a dilemma, making management challenging. Termination of pregnancy in the first trimester is imperative when a CSP is diagnosed. Diagnosing CSP at 13 weeks of gestation can be difficult and requires special attention and training. Subserosal uterine rupture can be closely monitored until beyond 28 weeks of gestation.
REFERENCES
1.
Pędraszewski P, Wlaźlak E, Panek W, Surkont G. Cesarean scar pregnancy – A new challenge for obstetricians. J Ultrason 2018;18(72):56–62. [CrossRef]
[Pubmed]

2.
Hameed MSS, Wright A, Chern BSM. Cesarean scar pregnancy: Current understanding and treatment including role of minimally invasive surgical techniques. Gynecol Minim Invasive Ther 2023;12(2):64–71. [CrossRef]
[Pubmed]
3.
Zhang Y, Gu Y, Wang JM, Li Y. Analysis of cases with cesarean scar pregnancy. J Obstet Gynaecol Res 2013;39(1):195–202. [CrossRef]
[Pubmed]
4.
Timor-Tritsch IE, Monteagudo A, Calì G, D’Antonio F, Kaelin Agten A. Cesarean scar pregnancy: Diagnosis and pathogenesis. Obstet Gynecol Clin North Am 2019;46(4):797–811. [CrossRef]
[Pubmed]
5.
Calì G, Timor-Tritsch IE, Palacios-Jaraquemada J, et al. Outcome of cesarean scar pregnancy managed expectantly: Systematic review and meta-analysis. Ultrasound Obstet Gynecol 2018;51(2):169–75. [CrossRef]
[Pubmed]
6.
Silva B, Viana Pinto P, Costa MA. Cesarean scar pregnancy: A systematic review on expectant management. Eur J Obstet Gynecol Reprod Biol 2023;288:36–43. [CrossRef]
[Pubmed]
7.
Caserta NMG, Bacha AM, Grassiotto OR. Cesarean scar ectopic pregnancy: Invasion of the bladder wall detected by magnetic resonance imaging. Radiol Bras 2017;50(3):197–8. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Mame Diarra Ndiaye - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ndèye Racky Sall - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Aminata Niass - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mamour Gueye - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Philippe Marc Moreira - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Mame Diarra Ndiaye et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}