 |
Case Report
Retroperitoneal mass presenting as stress urinary incontinence: A rare case presentation
1 DO, Capt, MC, USAF, Department of Gynecologic Surgery & Obstetrics, Naval Medical Center Portsmouth, Virginia, USA
2 DO, LT, MC, USN, Department of Gynecologic Surgery & Obstetrics, Naval Medical Center Portsmouth, Virginia, USA
3 MD, Ret Col USAF, FACOG, URPS, Department of Gynecologic Surgery & Obstetrics, Naval Medical Center Portsmouth, Virginia, USA
Address correspondence to:
Nichole Nilsen
DO, 620 John Paul Jones Cir, Portsmouth, VA 23708,
USA
Message to Corresponding Author
Article ID: 100188Z08NN2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Nilsen N, Fraiman A, Leach DA. Retroperitoneal mass presenting as stress urinary incontinence: A rare case presentation. J Case Rep Images Obstet Gynecol 2024;10(2):58–61.ABSTRACT
Introduction: The management of urologic injuries at the time of midurethral sling placement is well described but lacks specific guidance on when further anatomic investigation may be warranted. We present a rare case of an upper urinary tract problem and retroperitoneal mass causing lower urinary tract symptoms, specifically severe stress urinary incontinence.
Case Report: A 54-year-old female with stress urinary incontinence underwent attempted retropubic midurethral sling placement that was abandoned after repeated urinary tract injury at time of placement. A computed tomography (CT) urogram that was completed after repair of the injury identified a large retroperitoneal mass encasing the right kidney and ureter. Subsequent resection of this mass resulted in immediate resolution of the patient’s stress urinary incontinence.
Conclusion: Though urologic injuries at time of midurethral sling placement can be due to anatomic variation, further investigation is not often pursued. In the absence of relevant guidelines, clinically significant anatomic abnormalities may often be missed and left unaddressed. Though we present a rare case of stress urinary incontinence (SUI) that resolved after large mass resection, there are several risk factors present in this case that may inform clinicians when to pursue further evaluation and management.
Keywords: Midurethral sling trocar injury, Retroperitoneal mass, Stress urinary incontinence, Urinary tract injury
Introduction
The management of urologic injuries at the time of midurethral sling placement is well described but lacks specific guidance on when further anatomic investigation may be warranted. Though it is understood that anatomic variation can lead to trocar injury, further investigation is seldom pursued. In the absence of relevant guidelines, clinically significant abnormalities may often be missed and left unaddressed. We believe there are certain circumstances in which additional perioperative evaluation would reduce risk and improve outcomes. We present one such case today describing a large retroperitoneal mass causing stress urinary incontinence. The mass was discovered with imaging that was obtained due to urinary tract injury at time of midurethral sling placement, therefore we also provide suggestions that may lead to improved management and possible future guideline development.
Case Report
A 54-year-old G5P2 presented with a principal complaint of chronic stress urinary incontinence present for several years. On her intake questionnaire she had an International Consultation on Incontinence Questionnaire-Urinary Incontinence (ICIQ-UI) score of 18 (out of 21). On exam she demonstrated urethral hypermobility, a positive cough stress test, and had a normal post void residual by portable bedside sonogram. No other anatomic abnormalities were visualized or palpated on a detailed initial abdominopelvic exam. Review of systems was otherwise unremarkable. Initial efforts at symptom control through weight loss and pelvic floor physical therapy over the course of nine months were unsuccessful. She declined a trial of pessary and requested surgical management with a midurethral sling. Placement was subsequently attempted through a retropubic approach but was abandoned due to repetitive right sided cystotomy. Her postoperative ICIQ-UI score was 20 (out of 21).
Three months later, after an uneventful postoperative course and further counseling, she underwent transobturator midurethral sling placement to take advantage of its lower risk of bladder injury [1]. While the left helical trocar was placed without difficulty, placement of the right trocar resulted in proximal urethra and bladder neck injury. The procedure was again aborted, and the injury repaired. Subsequent retrograde ureterogram and cystogram prior to leaving the operating room were unremarkable.
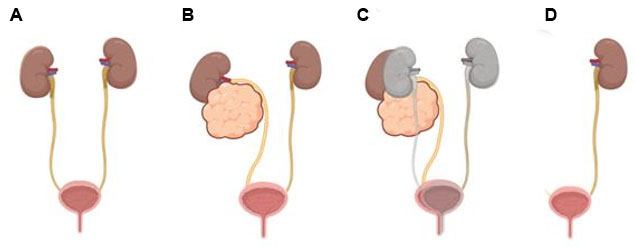
Her stress incontinence symptoms progressively worsened over the next several months during which time she also developed urinary urgency without evidence of associated urinary tract infection. Urodynamics were performed demonstrating a leak point pressure of 27 cm H2O at 200 mL infused consistent with intrinsic sphincter deficiency. Her bladder capacity was 511 mL, normal detrusor compliance was observed, and there were no contractions seen; her uroflow and post void residual were also both normal. To be sure worsening urinary symptoms were not due to an ongoing surgical defect or fistula, cystoscopy was performed with no abnormal findings noted. This was followed by a voiding cystogram and CT urogram with the latter demonstrating a right retroperitoneal lipomatous lesion with mass effect on the right kidney and right ureter (Figure 1). Magnetic resonance imaging (MRI) was also obtained and further detailed a retroperitoneal fatty mass centered inferior to the right kidney with encasement of the right ureter and multiple prominent enhancing septations characteristic of atypical lipoma or liposarcoma (Figure 2). Anterior and superior rotation of the lower pole of the kidney was also noted along with medial displacement of the associated ureter. She was referred to surgical oncology and a core needle biopsy revealed lipomatous lesion. After tumor board review and discussion of pathology, imaging, and management plans, the patient elected for removal. The mass was treated as a liposarcoma, therefore surgical removal led to removal of adjacent structures of her right kidney and ureter. After the mass removal, the final pathology resulted as benign and she reported immediate improvement in incontinence (changing 1 pad daily from 8–9 previously) following excision and expressed satisfaction with her degree of control. The displacement of this patient’s kidney and ureter caused a similar elevation of the right posterior bladder anteromedially, rotating the dome and extraperitoneal portion inferiorly into and under the ipsilateral pubic ramus and into the surgical field (Figure 3 and Figure 4). The increased tension also immobilized the urethrovesical junction resulting in loss of support and significant incontinence. With excision of this mass, anatomy was restored, tension was alleviated, and her urinary incontinence was corrected.



Discussion
This case highlights the importance of anatomic considerations in the management of stress urinary incontinence in select cases. Previously described risk factors for trocar injury include the presence of endometriosis and adhesions due to prior cesarean delivery, among others [2],[3]. One can also intuitively understand how lower urinary tract displacement from adhesive disease secondary to prior cesarean, endometriosis, pelvic masses such as fibroids, or other abdomino-pelvic surgery could cause urethrovesical dysfunction similar to that described in this report. Correcting adhesive disease caused by prior surgery or diseases such as endometriosis could not only reduce risk of trocar injury but potentially resolve urinary symptoms altogether.
Our review of the literature revealed several other reports of urinary incontinence corrected by removal of paraurethral, retropubic and anterior vaginal wall masses as well as one case of retroperitoneal teratoma excision that incidentally resolved overactive bladder symptoms [4],[5],[6]. To our knowledge, the association of stress incontinence with a retroperitoneal mass has not been previously described and our case is the only reported instance of a mass causing only urinary tract symptoms. In all other reports, and in this author’s experience with post cesarean adhesive disease, either abnormal physical exam findings or non-urologic symptoms prompted further evaluation. In the absence of preoperative symptoms and exam findings, aberrant anatomy may not be recognized until surgical difficulties or poor post-surgical symptom control is encountered. Data directing further management strategies in these circumstances are currently lacking [7].
Through our experience with this case and review of the available literature, we suggest consideration of further anatomic investigation in these following scenarios:
- Repeat cystotomy occurring at time of retropubic midurethral sling placement or any urologic injury occurring at the time of transobuturator sling placement.
- When there is no improvement in symptom control after technically successful midurethral sling placement.
- Preoperatively when symptom onset is rapid or is temporally related to prior pelvic surgery (e.g., uterus/lower uterine segment adhered to anterior abdominal wall after cesarean).
- Preoperatively in women with non-detrusor mediated urinary incontinence in the absence of urethral hypermobility and without risk factors for intrinsic sphincter deficiency (ISD) (myelopathy, advanced age, radical pelvic surgery or radiation and prior continence or prolapse surgery).
Though urologic injuries at time of midurethral sling placement as well as poor symptom control thereafter can be due to anatomic variation, further investigation is seldom pursued. In the absence of relevant guidelines, the opportunity to identify and optimally manage many clinically significant abnormalities may be missed.
Conclusion
We have presented a rare case of stress urinary incontinence caused by a large retroperitoneal mass. By using BioRender software technology, we were better able to conceptualize how the retroperitoneal mass distorted the anatomy contributing to surgical complications. Highlighting the importance of anatomic considerations in the management of stress urinary incontinence is important in select cases. It is our hope that surgeons find the lessons learned here useful and that they eventually be used to inform guideline development.
REFERENCES
1.
Huang ZM, Xiao H, Ji ZG, Yan WG, Zhang YS. TVT versus TOT in the treatment of female stress urinary incontinence: A systematic review and meta-analysis. Ther Clin Risk Manag 2018;14:2293–303. [CrossRef]
[Pubmed]

2.
Stav K, Dwyer PL, Rosamilia A, Schierlitz L, Lim YN, Lee J. Risk factors for trocar injury to the bladder during mid urethral sling procedures. J Urol 2009;182(1):174–9. [CrossRef]
[Pubmed]
3.
Casas-Puig V, Bretschneider CE, Walters MD, Ferrando CA. Risk factors for bladder perforation at the time of retropubic midurethral sling placement. Female Pelvic Med Reconstr Surg 2022;28(7):444–51. [CrossRef]
[Pubmed]
4.
Elmelund M, Thind P, Klarskov N. Retropubic cartilaginous cyst presenting as stress urinary incontinence. Int Urogynecol J 2015;26(3):455–7. [CrossRef]
[Pubmed]
5.
Yonguc T, Bozkurt IH, Polat S, et al. Surgical management of female paraurethral cyst with concomitant stress urinary incontinence. Int Braz J Urol 2017;43(6):1194. [CrossRef]
[Pubmed]
6.
Jeong GA. Retroperitoneal leiomyoma of the uterus mimicking sarcoma in perimenopausal woman: Case report. J Menopausal Med 2014;20(3):133–7. [CrossRef]
[Pubmed]
7.
Kavanagh A, Sanaee M, Carlson KV, Bailly GG. Management of patients with stress urinary incontinence after failed midurethral sling. Can Urol Assoc J 2017;11(6Suppl2):S143–6. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
The authors thank BioRender software company for its use in creating images to demonstrate the subject anatomy.
Author ContributionsNichole Nilsen - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Aviv Fraiman - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Douglas A Leach - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Nichole Nilsen et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}