 |
Case Report
Cerclage placement in coexistence of vasa previa and short cervix: The role of ultrasound mapping of fetal vessels
1 Department of Obstetrics and Gynecology, Division of Maternal Fetal Medicine, NYU Langone Hospital Long Island and NYU Grossman Long Island School of Medicine, Mineola, NY, USA
Address correspondence to:
Ifeoma M Ogamba-Alphonso
259 1st St, Mineola, NY 11501,
USA
Message to Corresponding Author
Article ID: 100202Z08IA2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Ogamba-Alphonso IM, Kantorowska A, Chavez MR, Kunzier NB. Cerclage placement in coexistence of vasa previa and short cervix: The role of ultrasound mapping of fetal vessels. J Case Rep Images Obstet Gynecol 2025;11(1):69–72.ABSTRACT
Introduction: The role of cerclage in patients with cervical shortening and vasa previa is understudied. Our case highlights the use of fetal vessel mapping by ultrasound to guide surgical technique and placement of cerclage in a patient with vasa previa.
Case Report: A 38-year-old primigravida with type 1 vasa previa and progressive cervical length shortening to 1 cm with funneling and amniotic fluid sludge underwent McDonald cerclage placement utilizing fetal vessel mapping. The cerclage was successfully placed without rupture of membranes and pregnancy was prolonged.
Conclusion: Cerclage placement may be a reasonable option to prevent further cervical shortening and preterm birth in patients with vasa previa if fetal vessel mapping by ultrasound is used to guide surgical technique.
Keywords: Cerclage, Cervical insufficiency, Preterm birth, Vasa previa
Introduction
The role of cerclage in patients with cervical shortening and coexisting vasa previa is understudied. Cerclage placement may prolong the duration of pregnancy; however, it is crucial to use proper surgical techniques to prevent membrane rupture and avoid injuring fetal vessels. Our case highlights the surgical technique and utilization of fetal vessel mapping by ultrasound to guide placement of cerclage in a patient with type 1 vasa previa.
Case Report
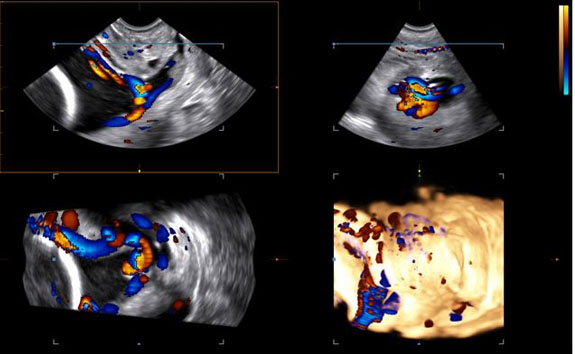
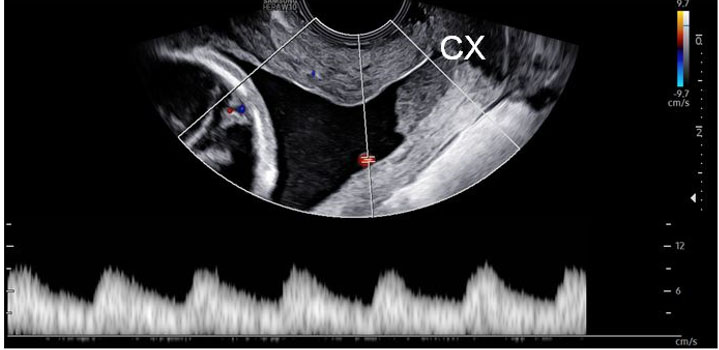
A 38-year-old G1P0 with in vitro fertilization (IVF) conception complicated by vanishing twin at nine weeks and history of abdominal myomectomy undergoing anatomical survey at 19w6d was incidentally noted to have cervical length (CL) of 1.7 cm with amniotic fluid sludge. Posterior velamentous cord insertion with fetal vessels traveling across the internal os and along the maternal right side of the cervical canal, consistent with type 1 vasa previa (Figure 1 and Figure 2) was visualized. The patient was counseled regarding management options and prognosis, and was started on vaginal progesterone 200 mg nightly.
At 21w2d, CL was 1 cm with funneling and sludge. Cervical cerclage was discussed as a surgical management option given continued cervical shortening despite compliance with progesterone. The unique risks posed by vasa previa were discussed such as further cervical shortening increasing the risks of both pregnancy loss and fetal hemorrhage, although cerclage placement posed its own risks given fetal vessels in the cervical canal. The patient consented to the procedure and McDonald cerclage was placed successfully. Color Doppler ultrasonography was utilized to map fetal vessel location prior to surgery to reduce the risk of fetal hemorrhage during cerclage placement and to allow for maximum gain in CL (Figure 3).
Intraoperative findings revealed 100% effacement, 1–2 cm dilation with bulging clear membranes. Typical placement of transcervical balloon to displace membranes cephalad could not be utilized due to the location of the fetal vessels and risk of rupture with placement. Therefore, steep Trendelenburg was utilized with retrograde bladder filling to reduce fetal membranes from the cervical canal. Prior vessel mapping allowed for maximal tissue length gain superiorly, along maternal left and posteriorly, with less significant cephalad advancement in the maternal right cervical region where the vasa previa was located (highest risk of hemorrhage). The patient was treated with antibiotics due to finding of amniotic fluid sludge [1]. Furthermore, vaginal progesterone was continued after cerclage placement.
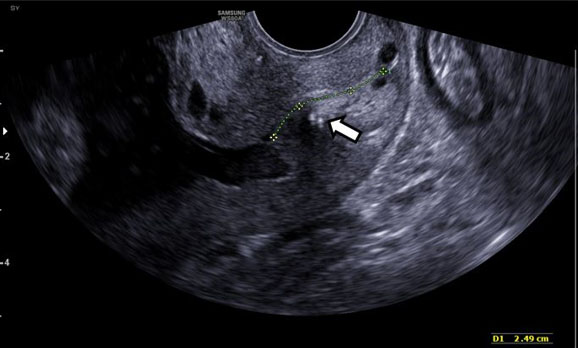
Postoperative ultrasound (at 22w2d) demonstrated CL of 2.7 cm without funneling and reduced sludge (Figure 4). Cervical length remained stable and the patient was asymptomatic until 27 weeks, when further cervical shortening to 1.2 cm was noted and antenatal corticosteroids were administered for fetal lung maturity. The couple greatly desired close outpatient surveillance rather than inpatient monitoring. Utilizing patient-centered decision making and to optimize timing of delivery, CL and tocometer were monitored weekly. At 34w0d, she underwent an uncomplicated planned Cesarean delivery because of vasa previa in the setting of pregnancy complicated by short cervix. The cerclage was removed after the completion of the cesarean section. She delivered a female neonate weighing 2310 g. The baby was admitted to the neonatal intensive care unit (NICU) on continuous positive airway pressure (CPAP). She was transitioned to room air by day 2 of life and received phototherapy for hyperbilirubinemia. Otherwise, the neonatal course was uncomplicated, and the baby was discharged on day 6. Gross placental examination showed velamentous cord insertion with intact fetal vessels running through the amniotic membranes (Figure 5).


Discussion
Vasa previa occurs when unprotected fetal vessels traverse the cervix. Two main types are described: Type 1, which is caused by velamentous cord insertion, and Type 2, which occurs secondary to a succenturiate lobe or multilobed placenta, with fetal vessels coursing over the cervix between the lobes [2]. Risk factors for vasa previa include assisted reproductive technology, low-lying placenta, placenta previa, and multiple gestation. Our patient had multiple risk factors, including IVF conception and pregnancy that began as a multifetal gestation.
Vasa previa occurs in approximately 1:2500 pregnancies and carries significant risks [2]. If rupture of membranes occurs, fetal vessels can rupture, causing rapid fetal exsanguination. It is critically important to prevent preterm labor (PTL) and preterm premature rupture of membranes (PPROM). Cervical length can be used to predict risk of PPROM/PTL. Serial cervical surveillance in patients with vasa previa, with change in clinical management based on CL, has previously been described [3],[4]. However, the role of cerclage in these patients is understudied. Cerclage is likely underutilized because of concerns about injury to fetal vessels during placement. Cerclage may be a reasonable option in preventing further cervical shortening and preterm birth if fetal vessel mapping by ultrasound is used to guide surgical technique.
Our case demonstrates that cerclage can be safely performed in patients with vasa previa when vessels are carefully mapped using ultrasound. Oyelese et al. have previously described ultrasound mapping of fetal vessels before Cesarean to guide placement of the uterine incision [5]. This technique can be adapted to guide cerclage placement in patients with vasa previa and short cervix. In our case, cerclage was successfully placed without rupture of membranes despite vessels in the cervical canal and cervical dilation. Surgical management aided in prolongation of pregnancy, allowing for the patient-driven choice of close outpatient monitoring rather than a prolonged hospital stay, and ultimately a scheduled late preterm delivery following steroids. Ultrasound mapping of the fetal vessels is a useful tool that can aid cerclage placement in patients with short cervix and vasa previa.
Conclusion
The coexistence of vasa previa should not preclude patients with short cervix from receiving optimal care. Based on the success of our case, we suggest that cerclage placement may be a reasonable option to prevent further cervical shortening and preterm birth in patients with vasa previa if fetal vessel mapping by ultrasound is used to guide surgical technique.
REFERENCES
1.
Oh KJ, Romero R, Park JY, et al. Evidence that antibiotic administration is effective in the treatment of a subset of patients with intra-amniotic infection/inflammation presenting with cervical insufficiency. Am J Obstet Gynecol 2019;221(2):140.e1–8. [CrossRef]
[Pubmed]

2.
Society of Maternal-Fetal (SMFM) Publications Committee; Sinkey RG, Odibo AO, Dashe JS. #37: Diagnosis and management of vasa previa. Am J Obstet Gynecol 2015;213(5):615–9. [CrossRef]
[Pubmed]
3.
Garretto D, Budorick NE, Figueroa R. Antenatal diagnosis of velamentous cord insertion and vasa previa: Preparing for a good outcome when the cervix is shortened. J Ultrasound Med 2012;31(6):963–5. [CrossRef]
[Pubmed]
4.
Odibo AO, Talucci M, Berghella V. Prediction of preterm premature rupture of membranes by transvaginal ultrasound features and risk factors in a high-risk population. Ultrasound Obstet Gynecol 2002;20(3):245–51. [CrossRef]
[Pubmed]
5.
Oyelese Y, Iammatteo M, Domnitz S, Chavez MR. Vasa previa: Avoiding incising the membranes at cesarean delivery. Am J Obstet Gynecol 2022;227(5):770–2. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Ifeoma M Ogamba-Alphonso - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Agata Kantorowska - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Martin R Chavez - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nadia B Kunzier - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Ifeoma M Ogamba-Alphonso et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}