 |
Case Report
Metastatic teratoma in a young female: A rare case of bowel involvement
1 MBBS, FCPS Part 1, Resident, Obstetrics and Gynecology, Dow University of Health Sciences, Karachi, Sindh, Pakistan
2 MBBS, House Officer, Obstetrics and Gynecology, Dow University of Health Sciences, Karachi, Sindh, Pakistan
3 MBBS, Student, Obstetrics and Gynecology, Dow University of Health Sciences, Karachi, Sindh, Pakistan
Address correspondence to:
Muhammad Mustafa
House no. 3/109, Street no. 10, Maqboolabad, Bahadurabad, Karachi East, Karachi, Sindh,
Pakistan
Message to Corresponding Author
Article ID: 100205Z08KM2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Memon KJ, Ahsan A, Farooqui T, Mahboob H, Mustafa M. Metastatic teratoma in a young female: A rare case of bowel involvement. J Case Rep Images Obstet Gynecol 2025;11(1):83–88.ABSTRACT
Introduction: Teratocarcinoma is a type of germ cell tumor that can occur in the ovaries or testes. It has features of both teratoma and carcinoma. It is considered a malignant tumor and can be aggressive, sometimes spreading to other parts of the body, such as the peritoneum. Treatment typically involves a combination of surgery and chemotherapy, although the tumor’s response to treatment can vary.
Case Report: This article discusses a rare instance of ovarian teratocarcinoma with peritoneal metastasis that is unresponsive to chemotherapy in a 24-year-old female patient. The patient has a positive family history of hepatocellular carcinoma. The patient underwent two sessions of chemotherapy but the tumor was unresponsive and the β-human chorionic gonadotropin (β-hCG) levels kept rising but a-fetoprotein levels decreased. Discussion: The diagnosis of teratocarcinoma in this case was hypothesized on histopathologic examination. Its heterogeneity was demonstrated by the aggressive behavior of bulky peritoneal carcinomatosis and resistance to the treatment. Throughout the clinical course this teratocarcinoma was resistant to bleomycin, cisplatin, etoposide (BEP) and paclitaxel, cisplatin, ifosfamide, and mesna (TIP) regimens which allows for in depth exploration of unique teratocarcinoma care.
Conclusion: This case exemplifies that rare cases of ovarian teratocarcinoma are chemotherapy resistant and difficult to treat hence new and better treatment strategies should be explored.
Keywords: Carcinoma, Germ cell tumor, Peritoneal metastasis, Teratoma
Introduction
Teratoma is a benign tumor that consists of a mixture of differentiated tissues and three germ layer derivatives, while teratocarcinoma also consists of embryonal carcinoma cells [1]. The most common type is sacrococcygeal teratomas, they are rare but predominantly occur in infants [2]. In adult females, benign ovarian teratoma is common, while testicular teratoma in adults is malignant [3]. Mature cystic teratomas are common ovarian tumors, and in some cases, they can be associated with anti-N-methyl-d-aspartate receptor encephalitis, presenting with psychiatric symptoms that respond to tumor resection and immunotherapy [4],[5]. The malignant transformation is rare but has a higher incidence in older patients and larger tumors [4],[6]. Risk factors for malignant transformation are older age, larger tumor size, elevated CA-125 levels, and postmenopausal status [7]. Mature and immature tumors can relapse if the tumor resection is incomplete [8]. Growth factors play a crucial role in teratoma cell proliferation [9]. Mature cystic teratomas and dermoid cysts are common ovarian tumors, but extragonadal teratomas are rare, and the most common location is omentum [10]. According to a study, only 31 cases of omentum teratoma are reported, out of which only 4 cases have dermoid cysts and omentum teratoma coexisting [10].
Case Report
A 24-year-old divorced woman from Larkana, Sindh, Pakistan, with no known comorbidities, was diagnosed with ovarian teratocarcinoma with peritoneal metastasis. She had two previous C-sections, the last performed 2.5 years ago. Her mother had hepatocellular carcinoma.
She had her last menstrual cycle in October 2023. After receiving chemotherapy, she developed amenorrhea, lower abdominal pain, and chemotherapy-induced menopause, presenting at Dow University Hospital.
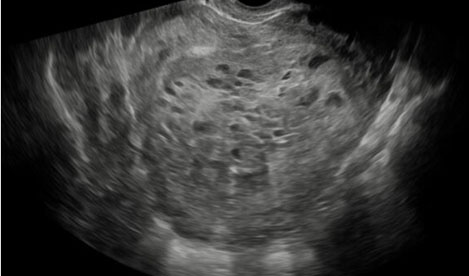
On October 14, 2023, a pelvic mass was excised at Indus Hospital, Larkana. Ultrasound showed an 11×10 cm adnexal mass. Gross examination revealed a solid, lobulated, gray-white tumor with cystic spaces. Histology confirmed teratocarcinoma, consisting of teratomatous and embryonal carcinomatous elements, with pleomorphism, necrosis, and high mitotic activity. The teratomatous component included primitive mesenchymal tissue, neural elements, chondroid tissue, and cystic structures lined by respiratory and intestinal epithelium, while the malignant epithelial component showed granular and papillary structures with yolk sac differentiation. (Representative Blocks of Tumor Examined >04).
On November 11, 2023, a computed tomography (CT) scan of the whole abdomen showed multiple heterogeneously enhancing peritoneal masses, the largest measuring 9.2×6.8 cm in the pelvis. Another lesion in the right mid-abdomen measured 4.4×5.0 cm. There was mild to moderate ascites, nodular omental thickening, and mesenteric involvement. The right distal ureter was compressed, causing mild hydronephrosis, but the liver, spleen, gallbladder, kidneys, pancreas, and adrenal glands were normal.
She began BEP chemotherapy (bleomycin, cisplatin, etoposide) on November 11, 2023, completing four cycles by February 7, 2024.
On March 21, 2024, a follow-up CT scan showed tumor progression, with the largest pelvic mass increasing to 11.3×7.5 cm (previously 9.2×6.8 cm) and a mid-abdominal lesion increasing to 6.0×7.5 cm (previously 4.4×5.0 cm). Minimal ascites persisted, but omentum thickening had resolved. The liver, spleen, pancreas, gallbladder, kidneys, and adrenal glands remained normal. There were no hepatic, pulmonary, or bony metastases.
On June 5, 2024, a CT abdomen and pelvis post-second-line chemotherapy showed stable disease, with no significant change in tumor size. Multiple calcified peritoneal lesions persisted, and mild left adrenal gland bulkiness was noted. There was no evidence of intrapulmonary, hepatic, or bony metastasis.
She remained in chemotherapy-induced menopause with a stable disease process. She began TIP chemotherapy (paclitaxel, cisplatin, Ifosfamide, and Mesna) on 1st April 2024, completing four cycles by 5th of June 2024. A follow-up chest X-ray was done on 12th of July 2024 which was unremarkable.
As shown in Figure 1, a magnetic resonance imaging (MRI) of the pelvis was done, which showed a normal uterus measuring 3.8 × 3.4 2.6 in craniocaudal (CC) × transverse (TR) × anteroposterior (AP) dimensions. Multiple lobulated abnormal signal intensity lesions were seen in the pelvis, most of them demonstrate iso-to-hypointense signals on T1-weighted images. Hypo- to hyperintensity identified on T2-weighted images with heterogeneous post-contrast enhancement. One of the largest lesions was seen in the midline of the pelvis with multi-loculated intercystic spaces, approximately 9.1 × 7.0 × 5.3 cm in TR AP × CC dimensions, while one of the largest mesenteric lesions subjacent to the anterior abdominal wall approximately measured 4.8 × 4.6 × 2.8 cm in CC × TR × AP dimensions. The lesions were inseparable from pelvic ileal loops and uterine fundus, displacing the uterus toward the midline in the pelvis. Similar lesions were seen in the pouch of Douglas, the largest one measuring 4.2 × 3.4 cm, displacing the uterus anteriorly. The bilateral adnexal region also had lobulated lesions. The lower abdomen showed another multi-lobulated heterogeneously enhancing lesion mesenteric lesion measuring 7.6 × 3.8 cm in axial dimension within the center of the mesentery, inseparable from the adjacent bowel loops, but had no bowel obstruction. No inguinal pelvic lymphadenopathy was identified, bones appeared normal, with no evidence of marrow replacement, and the vascular structures appeared normal in the pelvis. These findings were secondary to known teratocarcinoma with peritoneal involvement.
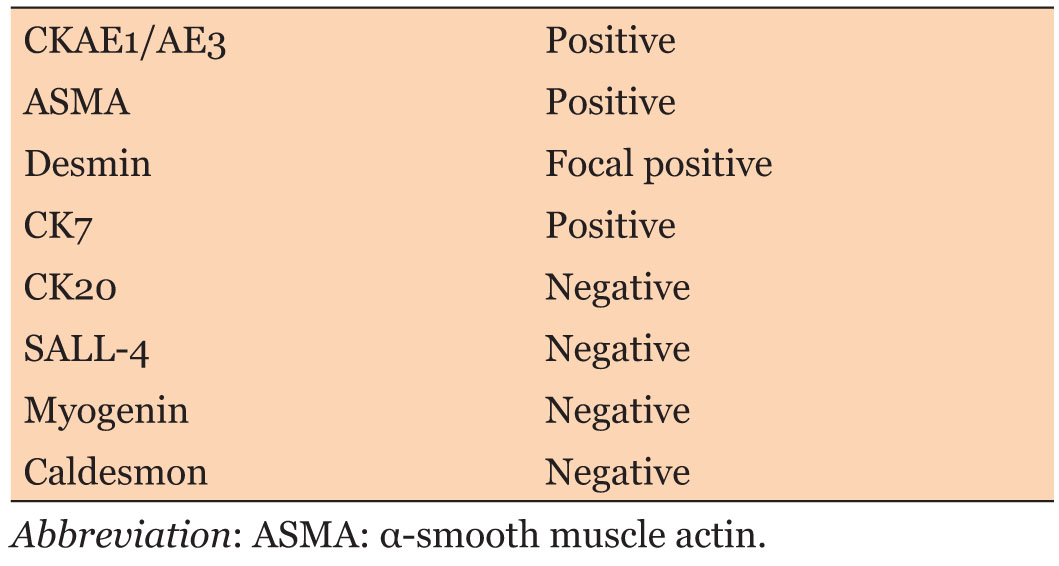
On the 25th of July 2024, a fluid cytology was performed which revealed hemorrhagic fluid mixed with tiny clusters of atypical cells exhibiting enlarged rounded hyperchromatic nuclei, vesicular chromatin, and moderate cytoplasm. Cell block preparation revealed fibrous tissue with clusters of atypical cells which suggested malignancy admixed with histiocytes, neutrophils, and multinucleated giant cells. Application of a panel of immunohistochemical markers on cell block and atypical cells, the following reactivity pattern was seen in Table 1.
On the 25th of July, a tissue biopsy was also performed. Grossly, the specimen consisted of three nodular tissue places. The larger lesion measured 3 × 2.5 × 2 cm, while the smaller lesion collectively measured 2 × 1.5 × 1 cm. On sectioning, the cut surface is identified as pale white.
Microscopically, the sections examined revealed fibrous tissue, which is composed of lobules of proliferating chondrocytes with increased cellularity. Binucleated chondrocytes were also seen, and there were areas of bone formation. Cystic spaces were identified as lined by benign epithelium. There was no evidence of somatic malignancy. In conclusion, the chondroid seen may behave aggressively since there was increased cellularity, multilobulated, and binucleation of chondrocytes. There was no convincing evidence of an adenocarcinoma or squamous cell carcinoma to commit to a diagnosis of teratocarcinoma. However, the cartilaginous area seen in this biopsy may behave aggressively. The previous biopsy on which the diagnosis of teratocarcinoma was made was not available for correlation. This biopsy was reviewed again and had the same findings.
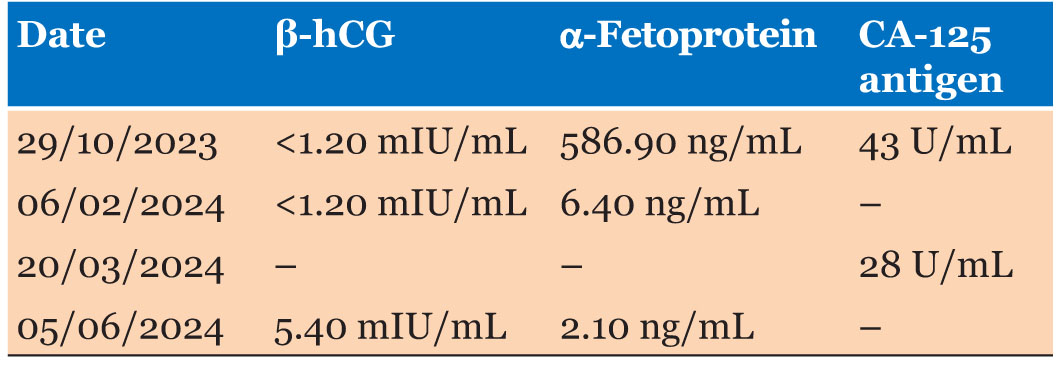
Even after both sessions of chemotherapy, the β-hCG levels kept rising while the a-fetoprotein (AFP) levels decreased. The levels of CA-124 antigen decreased after the first session of chemotherapy as depicted in Table 2.
A follow-up CT scan was done on the 28th of February 2025, which reported an increase in comparison to the previous scan of the size of one of the pelvic lesions seen. However, the rest of the lesions showed no interval change in size or number since the previous study.

Discussion
Here, we report a challenging case of ovarian teratocarcinoma in a 24-year-old woman with large peritoneal metastasis resistant to standard chemotherapy regimens. Her clinical course, including prior resistance to BEP and TIP regimens, as well the continued presence of elevated β-hCG levels, allows for an in-depth analysis of her unique teratocarcinoma care and treatment refractoriness. An infrequently encountered germ cell tumor is ovarian teratocarcinoma, which represents a combination of embryonal carcinoma and elements typically found in prepubertal cluster cancer (teratomas). Nevertheless, the aggressive presentation of this case in terms of bulky peritoneal carcinomatosis and treatment of refractory disease demonstrates its heterogeneity. The age of the patient and widespread metastasis are both noteworthy since teratocarcinomas that extensively involve the peritoneum are uncommon in these types of tumors. Usually, surgical resection is the mainstay treatment for teratoma with malignant transformation, but chemotherapy also has a role in selective patients; this is determined by cell type [11]. Chemotherapy for single-cell type malignant transformation teratoma resulted in long-term survival in some patients, but to achieve the maximum response, local therapy after chemotherapy is important [11]. Newer treatment options include fertility-sparing cytoreduction, which is done if the malignant ovarian germ cell tumor is chemotherapy-sensitive, fertility-sparing cytoreductive surgery should be considered as the initial treatment for advanced-stage tumors [12]. Along with cytoreduction, neoadjuvant chemotherapy can also be advantageous. Immature teratoma is also a subtype of malignant ovarian germ cell tumor. Moreover, cytoreduction can be done for immature teratomas as well [12].
Conservative standard treatment protocols for teratocarcinoma typically involve the BEP regimen, which was initially performed on this patient. Imaging showed ongoing and increasing disease despite four cycles of BEP, likely representing progression with enlarging peritoneal masses and calcified lesions. Refusal of BEP and subsequent change to the TIP regimen, plus the low response seen, reflects that more individualized or innovative therapeutic approaches are needed. All this emphasizes a critical void in the treatment protocols for the unmanageable spread of teratocarcinoma. In postmenopausal women, oophorectomy is the standard treatment, and it should be considered in premenopausal women as well, with multiple teratomas in one ovary and in women with large teratomas, which is destroying normal ovarian tissue [13].
The diagnosis of teratocarcinoma was originally hypothesized upon histopathological examination. Serial imaging disclosed active disease despite aggressive interventions, and the masses were not shrinking but remained stable. This raises important questions about the biology of the tumor and metabolism with conventional chemotherapy drugs. The fact that another solid tumor progressed unabated despite months of chemotherapy, resulting in the appearance on MRI and CT scan of “stable disease,” reflects how little our current regimens can effectively target all components somewhat resistant, such as this one. The serum markers of the patient revealed decreasing levels of AFP after treatment, which is consistent with response to therapy for teratocarcinoma. Recurrent tumor nodule (TN) resulted in a further rise in β-hCG even under aggressive management, although this may imply failure or resistance to treatment. These biological properties thicken the plot concerning treatment monitoring and disease progression, with an additional level of complexity provided by varying levels of CA-125 [3].
Conclusion
This is an interesting case of ovarian teratocarcinoma along with peritoneal metastasis that exemplifies the difficulties in treating a rapidly proliferating and chemotherapy-insensitive tumor. Given that the patient met progression criteria on both standard and second-line treatments, future strategies should include a more personalized approach or an innovative therapy. This increases our knowledge of teratocarcinoma and highlights the necessity of continuing research into more potent therapies for refractory cases. To create new therapeutic strategies, further study is needed to elucidate the molecular and genetic mechanisms of chemotherapy resistance in teratocarcinoma.
REFERENCES
1.
Bulic-Jakus F, Katusic Bojanac A, Juric-Lekic G, Vlahovic M, Sincic N. Teratoma: From spontaneous tumors to the pluripotency/malignancy assay. Wiley Interdiscip Rev Dev Biol 2016;5(2):186–209. [CrossRef]
[Pubmed]

2.
Forrester MB, Merz RD. Descriptive epidemiology of teratoma in infants, Hawaii, 1986–2001. Paediatr Perinat Epidemiol 2006;20(1):54–8. [CrossRef]
[Pubmed]
3.
The Epidemiology of Human teratomas [Internet]. [Available at: https://ouci.dntb.gov.ua/en/works/4azakZNl]
4.
Papadias K, Kairi-Vassilatou E, Kontogiani-Katsaros K, Argeitis J, Kondis-Pafitis A, Greatsas G. Teratomas of the ovary: A clinico-pathological evaluation of 87 patients from one institution during a 10-year period. Eur J Gynaecol Oncol 2005;26(4):446–8.
[Pubmed]
5.
Zhou X, Sun D, Feng L, et al. Ovarian teratoma associated with anti-N-methyl-D-aspartate receptor encephalitis: A report of 5 cases and review of the literature. [Article in Chinese]. Zhonghua Fu Chan Ke Za Zhi 2014;49(4):281–6.
[Pubmed]
6.
Black JD, Roque DM, Pasternak MC, et al. A series of malignant ovarian cancers arising from within a mature cystic teratoma: A single institution experience. Int J Gynecol Cancer 2015;25(5):792–7. [CrossRef]
[Pubmed]
7.
Park CH, Jung MH, Ji YI. Risk factors for malignant transformation of mature cystic teratoma. Obstet Gynecol Sci 2015;58(6):475–80. [CrossRef]
[Pubmed]
8.
Göbel U, Calaminus G, Engert J, et al. Teratomas in infancy and childhood. Med Pediatr Oncol 1998;31(1):8–15. [CrossRef]
[Pubmed]
9.
Engström W, Tally M, Granerus M, Hedley EP, Schofield P. Growth factors and the control of human teratoma cell proliferation. Recent Results Cancer Res 1991;123:145–53. [CrossRef]
[Pubmed]
10.
Hegde P. Extragonadal omental teratoma: A case report. J Obstet Gynaecol Res 2014;40(2):618–21. [CrossRef]
[Pubmed]
11.
Donadio AC, Motzer RJ, Bajorin DF, et al. Chemotherapy for teratoma with malignant transformation. J Clin Oncol 2003;21(23):4285–91. [CrossRef]
[Pubmed]
12.
Li J, Wu X. Current strategy for the treatment of ovarian germ cell tumors: Role of extensive surgery. Curr Treat Options Oncol 2016;17(8):44. [CrossRef]
[Pubmed]
13.
Cong L, Wang S, Yeung SY, Lee JHS, Chung JPW, Chan DYL. Mature cystic teratoma: An integrated review. Int J Mol Sci 2023;24(7):6141. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Kanwal Jan Memon - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Aiman Ahsan - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Tehreem Farooqui - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Haniah Mahboob - Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Muhammad Mustafa - Conception of the work, Design of the work, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Kanwal Jan Memon et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}