 |
Case Report
Rare case of pregnancy and breast cancer
1 MBBS, DGO, FRCOG, MRCOG, PGDPC, PGDMLE, Senior Consultant, Department of Gynecology & Obstetrics, Rainbow Children’s Hospital, 3/3-3/4, Amblipura Village, Varthur Hobli, Sarjapur Road, Bengaluru, Karnataka 560103, India
2 MBBS, Diploma in Medical Radio-Diagnosis, Senior Consultant Radiologist, Department of Radiology, Rainbow Children’s Hospital, 3/3-3/4, Amblipura Village, Varthur Hobli, Sarjapur Road, Bengaluru, Karnataka 560103, India
3 MBBS, MD, Associate Consultant, Department of Gynecology & Obstetrics, Rainbow Children’s Hospital, 3/3-3/4, Amblipura Village, Varthur Hobli, Sarjapur Road, Bengaluru, Karnataka 560103, India
Address correspondence to:
Shefali Tyagi
MBBS, DGO, FRCOG, MRCOG, PGDPC, PGDMLE, Senior Consultant, Department of Gynecology & Obstetrics, Rainbow Children’s Hospital, Sarjapur Road, Bengaluru, Karnataka,
India
Message to Corresponding Author
Article ID: 100206Z08ST2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Tyagi S, Bhagat S, Gauthami M. Rare case of pregnancy and breast cancer. J Case Rep Images Obstet Gynecol 2025;11(1):89–91.ABSTRACT
Introduction: Breast cancer is the most common cancer during pregnancy. When breast cancer is diagnosed during pregnancy or in the first year of postpartum, it is termed as pregnancy-associated breast cancer (PABC). Pregnancy-associated breast cancer affects one in every 30,000 pregnancies, with an increased incidence in recent years mainly due to higher maternal age at delivery.
Case Report: In this case report, we describe the case of 29-year-old woman diagnosed with PABC. She was diagnosed with breast cancer and conceived the same month. She underwent breast conservation surgery in the first trimester followed by chemotherapy in the second trimester. With multispecialty support we could prolong the pregnancy till 35+ weeks, post which a healthy baby was delivered by cesarean section. The case report explains the management and treatment protocol (surgery, chemotherapy, obstetrics management, and outcome).
Conclusion: Management and treatment protocol of PABC needs to be tailor made for the affected patient as there are multiple variables to be managed.
Keywords: Chemotherapy, Duct carcinoma, Mammography, Pregnancy-associated breast cancer
Introduction
Breast cancer is the most common cancer during pregnancy. When breast cancer is diagnosed during pregnancy or in first year of postpartum, it is termed as pregnancy-associated breast cancer (PABC). Pregnancy-associated breast cancer affects one in every 30,000 pregnancies, with an increased incidence in recent years mainly due to higher maternal age at delivery [1]. Management and treatment protocol of PABC needs to be tailor made for the affected patient as there are multiple variables to be managed. In this case report, we describe the case of 29-year-old woman diagnosed with PABC and the management and treatment protocol (surgery, chemotherapy, obstetrics management, and outcome).
Case Report
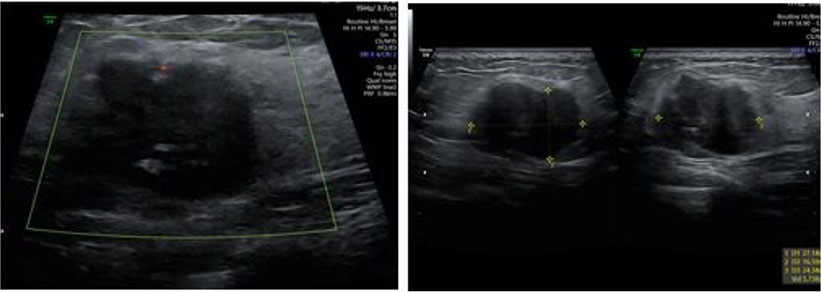
A 29-year-old woman, who had lumpectomy in 2016 which was found to be benign, visited for preconception counseling. Unfortunately, she had not retained the medical notes and discharge summary of that surgery. She again presented with a lump in the same breast and was recommended to have an ultrasound which showed BIRADS 4–5 suspicious of malignancy (Figure 1). Mammography picked up a 3 × 2.3 cm mass in upper-inner quadrant (UIQ) of left breast with left axillary lymphadenopathy. She was referred to a breast oncologic surgeon who recommended a biopsy. The mass was diagnosed as invasive ductal carcinoma (IDC) grade 3, ki-67>25% and a positron emission tomography (PET) scan was recommended. During this period, she missed her periods and tested positive for pregnancy and hence PET scan was deferred. She was offered termination, but she declined. She underwent left breast conservation surgery with axillary sampling and clearance. She was diagnosed as stage IDC III p T2N2Mo, HPR T 3 cm IDC IIILVI +9/22 nodes positive. The patient underwent chemotherapy with Doxorubicin and Cyclophosphamide from second trimester three weekly for 4 cycles. Her anomaly scan was normal, but she had complete placenta previa due to which she had repeated episodes of bleeding per vaginum. This required multiple admissions to the hospital to try and prolong the pregnancy. Her antenatal growth scans were done regularly to assess the growth of fetus and look for any lesions (metastasis) in liver.
She started next cycle of chemotherapy with Paclitaxel 300 mg every three weeks. Two weeks after the 3rd cycle of chemotherapy, she again had a bout of bleeding. Given her medical condition and the fact that she had crossed 35 weeks, it was decided to deliver the baby by caesarean section. A healthy 2.6 kg male baby was delivered and was kept in Neonatal Intensive Care Unit (NICU) as a precautionary measure. Pediatric team found no need for breathing assistance, feeding was also fine and hence the baby was shifted to the mother’s side within 5 hours. The patient was discharged on Day 3 in stable condition. Soon after discharge, she underwent the pending PET scan and there were no abnormal hypermetabolic lesion in left breast or axillary lymph nodes and no evidence of distant metastasis. Currently she is continuing her chemotherapy.
Discussion
In pregnancy and lactation breast, cervical/hematological disease and melanoma are most common malignancies with the first two contributing 50% of the cases. No specific risk factors have been identified but mutations play an important role. For women in their 20s, 33% of breast cancer can be due to mutations. Women with BRCA1 germline mutation have high risk of developing PABC. The presenting symptoms of PABC can be a lump or nipple discharge [2]. However, due to physiological alterations of breast, the diagnosis can be delayed.
Ultrasound remains the first line imaging modality for diagnosing PABC as it has high sensitivity. Pregnancy-associated breast cancer appears as a hypoechoic mass with fluid in center due to cystic degeneration of central tissue accompanied by irregular margins and posterior shadowing. Ultrasound also helps diagnose nodal disease and response to chemotherapy. Mammography can be done with Mediolateral Oblique View. The combination of ultrasound and mammography has diagnostic efficacy comparable to contrast-enhanced breast magnetic resonance imaging (MRI). Contrast-enhanced MRI is restricted in pregnancy as Gadolinium based contrast agents cross the placenta to reach the baby. It stays in amniotic fluid where its ions can affect the baby [3]. A fine needle aspiration biopsy or core biopsy can help with the diagnosis. In our case Mammography had already been done by the time she realized she was pregnant, and confirmation was done by a biopsy.
Treatment modalities should be taken forward as a multidisciplinary approach with the obstetrician, oncologist, fetal medicine specialist, and pediatrician working closely together on any decisions. Surgery with mastectomy with axillary staging can be one option. Breast conservative surgery is done in few cases. Radiotherapy can be harmful for baby hence it should be deferred till after delivery. Chemotherapy is widely used in the second and third trimester. Doxorubicin, Cyclophosphamide, and Paclitaxel are common drugs used. Methotrexate is contraindicated due to birth defects associated with it.
Majority of women with PABC can have a preterm labor due to chemotherapy effect. In such cases either induction of labor or cesarean can be done. Ideally, delivery should be done three weeks from the last chemotherapy dose. Breast feeding is contraindicated during chemotherapy or hormonal therapy.
Effect of pregnancy on breast cancer
The physiological changes of pregnancy like palpable nodules, large volume, and increased density can lead to delay in diagnosis, as physical examination and imaging are difficult. Hence PABC is more likely to be diagnosed at later date. Women with PABC have increased lymph node involvement and increased risk of metastasis. The tumors are larger, high grade, and aggressive. About 70% of tumors are negative for both estrogen and progesterone receptors [4].
Effect of breast cancer on pregnancy
Pregnancy-associated breast cancer is not harmful for fetus. However, the treatment modalities (particularly chemotherapy) can lead to intrauterine growth restriction, premature delivery, low birth weight, and transient leukopenia in the fetus. In the first trimester it can cause miscarriages and up to 17% risk of fetal malformations.
Compliance with ethical standards
All procedures performed on our patient were in accordance with the ethical standards of the institutional and/or national research committee.
Conclusion
Since women are delaying pregnancies, cases of PABC are likely to increase in the future. Awareness and keeping women informed of breast examination is important. Any suspicious lump should be scanned and if required a biopsy should be taken to confirm the diagnosis. Mastectomy, axillary clearance, or breast conservative surgery are the options for PABC. Chemotherapy can be started from second trimester. Genetic counseling should be provided to all pregnant women with breast cancer.
REFERENCES
1.
Parazzini F, Franchi M, Tavani A, Negri E, Peccatori FA. Frequency of pregnancy related cancer: A population based linkage study in Lombardy, Italy. Int J Gynecol Cancer 2017;27(3):613–9. [CrossRef]
[Pubmed]

2.
Boere I, Lok C, Poortmans P, et al. Breast cancer during pregnancy: Epidemiology, phenotypes, presentation during pregnancy and therapeutic modalities. Best Pract Res Clin Obstet Gynaecol 2022;82:46–59. [CrossRef]
[Pubmed]
3.
Galati F, Magri V, Arias-Cadena PA, et al. Pregnancy-associated breast cancer: A diagnostic and therapeutic challenge. Diagnostics (Basel) 2023;13(4):604. [CrossRef]
[Pubmed]
4.
Bounous VE, Minella C, Fuso L, et al. Impact of pregnancy on breast cancer features and prognosis. Curr Oncol 2024;31(4):2305–15. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
The case presentation has not been funded or sponsored.
Author ContributionsShefali Tyagi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Swapnil Bhagat - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Gauthami M - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent for publication of the clinical details and/or clinical images was obtained from the patient.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Shefali Tyagi et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}