 |
Case Report
Case report: Rare case of spontaneous and non-traumatic vulvar epidermoid cyst
1 Assistant Professor, Radiology Department, Aga Khan University Hospital, Karachi, Sindh, Pakistan
2 Specialist Radiologist, Radiology Department, Bahrain Specialist Hospital, Al Juffair, Manama, Bahrain
3 Consultant Radiologist, Radiology Department, Jinnah Postgraduate Medical Center, Karachi, Sindh, Pakistan
4 Radiology Resident, Radiology Department, Aga Khan University Hospital, Karachi, Sindh, Pakistan
5 Women Imaging Fellow, Radiology Department, Aga Khan University Hospital, Karachi, Sindh, Pakistan
Address correspondence to:
Fatima Qaiser
Aga Khan University Hospital, Stadium Road, Karachi, Sindh,
Pakistan
Message to Corresponding Author
Article ID: 100208Z08GS2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Shafqat G, Shaikh A, Kaleemi R, Ahmed M, Qaiser F. Case report: Rare case of spontaneous and non-traumatic vulvar epidermoid cyst. J Case Rep Images Obstet Gynecol 2025;11(1):97–101.ABSTRACT
Introduction: Epidermoid cysts are nodular structures lined with stratified squamous epithelium. In most cases, epidermoid cysts arise in the head and neck region, or in extremities, with their occurrence in the female genital tract being rare. Cases of epidermoid cysts in the female genital tract tend to have a history of trauma—mostly surgical or due to female genital tract mutilation. We present a case of biopsy proven vulvar epidermoid cyst which arose without a background of prior surgical history, female genital mutilation, or other trauma.
Case Report: A 25-year-old multigravida female with two children presented with progressive painless vulvar swelling for around two years, without any history of trauma or prior surgery. Vulvar ultrasound examination revealed a well-circumscribed, ovoid subcutaneous tissue mass arising from the labia majora with internal linear echogenic and anechoic foci, as well as raised through-transmission. Magnetic resonance imaging (MRI) examination revealed an exophytic, round-to-ovoid subcutaneous mass lesion in the vulvar region which returned iso- to hyperintense signals on T1, hyperintense signals on T2-weighted images, and hyperintense signals on diffusion weighted imaging (DWI), while demonstrating a peripheral rim of enhancement on T1 post-contrast images. The patient underwent surgical excision without any complications and histopathology reaffirmed the diagnosis of vulvar epidermoid cyst having a stratified squamous epithelial lining.
Conclusion: While epidermoid cysts of the female genital tract are rare occurrences in patients lacking prior surgical or traumatic history, they need to be considered as possible differential diagnoses in patients presenting with characteristic symptoms and imaging findings. Further evaluation of the clinical course and imaging findings of epidermoid cysts in the female genital tract, as well as the efficacy of different imaging modalities and interventions is essential to improve their diagnosis and management.
Keywords: Epidermoid cyst, Female genital tract, Non-traumatic, Vulvar lesion
Introduction
Epidermoid cysts are nodular structures with a lining of stratified squamous epithelium. While numerous cases of epidermoid cysts stemming from head and neck or extremities are reported, epidermoid cysts arising from the female genital tract are rare [1]. In such cases, the etiology either draws on trauma of the female genital tract, female circumcision, or episiotomy. In this article, a case of biopsy proven vulvar epidermoid cyst lacking any prior trauma or surgical history has been reported.
Case Report
This case is of a young married female with two children, both delivered via cesarian section. She presented to the clinic with progressive painless vulvar swelling for around two years. There was no trauma or surgical history. The patient sought medical attention primarily due to the increasing size of the lesion, as well as discomfort associated with it.
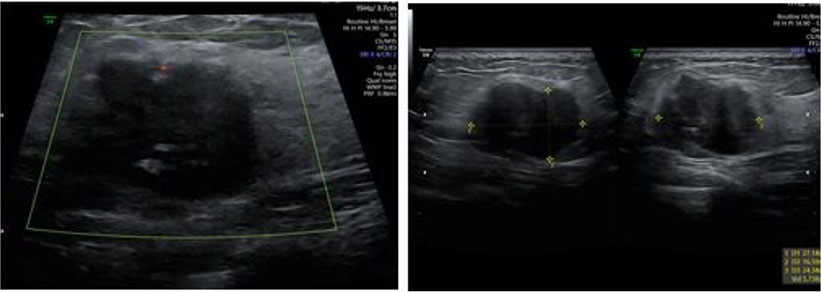
The patient was referred to the radiology department to perform vulvar ultrasound. Ultrasound revealed a well-circumscribed, ovoid subcutaneous tissue mass arising from the labia majora. The mass had internal linear echogenic foci, as well as raised through-transmission. It measured around 67 × 34 mm and lacked vascularity on color Doppler examination (Figure 1).
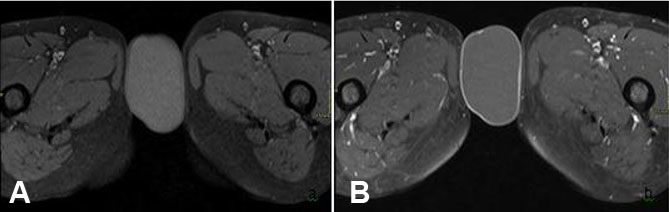
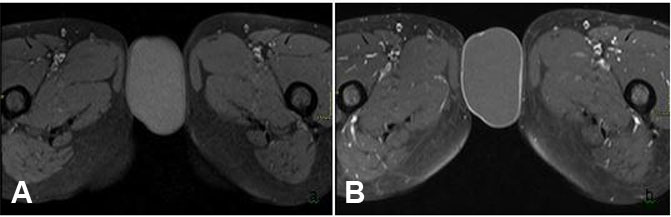
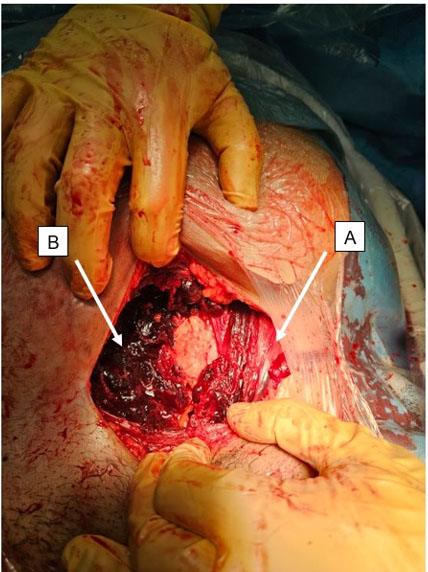
Further evaluation of the mass was undertaken via MRI pelvis—this was conducted via a 1.5 T MR system (the Magnetom Symphony, Siemens Germany). Magnetic resonance imaging examination revealed an exophytic, round to ovoid subcutaneous tissue mass involving the vulvar region, measuring around 61 × 36 mm. It returned hyperintense signals on T2-weighted sequences (Figure 2) and mild hyperintense signals on T1 (Figure 3) with a thin peripheral rim of enhancement on T1 post-contrast sequences (Figure 3). Additionally, the mass showed diffusion restriction (Figure 4). These imaging features were consistent with vulvar epidermoid cyst, and surgical excision was recommended. The patient underwent surgical excision without any complications and histopathology reaffirmed the diagnosis of vulvar epidermoid cyst having a stratified squamous epithelial lining.


Discussion
Epidermoid cysts, alternatively referred to as epidermal inclusion or epidermal cysts are fairly common benign lesions arising from intradermal or subcutaneous tissues on the face, scalp, trunk, neck, or extremities. Limited cases of epidermoid cysts arising from other areas, such as the palms or soles, fingers, breasts, and male/female genitalia are reported [1],[2]. While epidermoid cysts arise most commonly from head and neck structures for only 3% arise from the female genital tract [2].
Among cases of epidermoid cysts arising from the female genital tract, majority emerge from the clitoris [1], with female circumcision or genital trauma being common predisposing factors [3],[4]. Indeed, female genital mutilation has been reported as a major cause of epidermoid cysts of the clitoris. In one case, for instance, an epidermoid cyst of the clitoris had been reported in a middle-aged multiparous female who experience Type III genital mutilation when she was 8 years old [5]. In our case, however, the patient lacked any history of trauma, surgery, or genital mutilation.
As mentioned earlier, epidermoid cysts of the vulva are quite rare [6]. They are often multi-cystic and most of the locules have a diameter of less than 1 cm. The growth rate of these cysts tends to be low, and few grow beyond the diameter of 5 cm. The largest vulvar epidermoid cyst reported to date was in a 33-year-old female who had experienced female genital mutation, with the cyst’s diameter being 12 cm [5]. In most cases, vulvar epidermoid cysts are asymptomatic. It is, however, possible for them to be infected—in these cases, the patient can present with generalized pain or discomfort while walking.
Ultrasound is the initial modality of choice for evaluating epidermoid cysts. On ultrasound examination, epidermoid cysts appear as well-defined, ovoid, and slightly hyperechoic masses which may have linear hyperechoic foci. It is possible for these masses to have a hypoechoic peripheral rim, raised through-transmission and no flow on Doppler examination [7],[8].
Magnetic resonance imaging represents a useful modality for further evaluation of epidermoid cysts, as it can differentiate between different cystic masses, provide insights regarding infiltration of adjacent tissues, and give valuable information regarding its location. On MRI examination, cystic structures return hypointense signals on T1 and hyperintense signals on T2-weighted sequences. A key difference between epidermoid cysts and other cystic structures is that the former return hyperintense signals on diffusion weighted sequences and low signals on apparent diffusion coefficient (ADC), i.e., showing diffusion restriction, which is a characteristic feature of epidermoid cysts [8]. These findings were evident in our case too, the cyst showed hyperintense signals on T2 and also showed diffusion restriction [9].
Given the rarity of vulvar epidermoid cysts, particularly in non-traumatic settings, it can often be confused with other cysts and masses originating from the vulva. Other benign cystic lesions of the female genital tract include Bartholin gland cyst, Skene’s duct cyst or lipomas [10],[11]. Other cases of vulvar masses and cysts have identified cyst of the canal of Nuck, inclusion cysts, squamous cell carcinoma, and Bartholin gland carcinoma as important differentials [12],[13],[14],[22],[23]. However, these lesions tend to have characteristic findings on ultrasound and MRI, which have been summarized in Table 1.
Despite the characteristic imaging findings of vulvar epidermoid cysts (as outlined in Table 1), the diagnosis of epidermoid cyst can only be confirmed on histopathology—as documented in our case, this includes the demonstration of characteristic features, such as a stratified squamous epithelial lining of the cyst wall and often, a central keratinous debris. While it is rare for epidermoid cysts to undergo malignant transformation, it is certainly possible. It is estimated that around 1% of epidermoid cysts undergo malignant transformation, giving rise to basal or squamous cell carcinomas [9],[15].

Conclusion
To date, few cases of vulvar epidermoid cyst have been reported in the literature and that too, predominantly from countries where female genital mutilation is prevalent. Our case is distinct in this regard, in that the patient did not have any history of trauma or surgery, and female genital mutilation is not prevalent in this part of the world. Additionally, there is a lack of local studies on vulvar epidermoid cysts, adding to the academic value of this case report. It is important, therefore, for radiologists to consider vulvar epidermoid cysts as a possible differential when evaluating vulvar swellings, even in cases that lack trauma or surgical history.
REFERENCES
1.
Karaman E, Çim N, Akdemir Z, Elçi E, Akdeniz H. Giant vulvar epidermoid cyst in an adolescent girl. Case Rep Obstet Gynecol 2015;2015:942190. [CrossRef]
[Pubmed]

2.
Sand FL, Thomsen SF. Clinician’s update on the benign, premalignant, and malignant skin tumours of the vulva: The dermatologist's view. Int Sch Res Notices 2017;2017:2414569. [CrossRef]
[Pubmed]
3.
Kibar Ozturk M, Zindanci İ, Zemheri E, Çakır C. The largest epidermal cyst with vitiligo lesions following female genital mutilation: A case report and literature review. Acta Dermatovenerol Alp Pannonica Adriat 2018;27(4):211–3.
[Pubmed]
4.
Takpe R, Bello OO, Onebunne CA. Case report: Huge inclusion cyst as a long term complication of female genital mutilation. South Sudan Medical Journal 2019;12(3).
5.
Birge O, Erkan MM, Serin AN. Case report: Epidermoid inclusion cyst of the clitoris as a long-term complication of female genital mutilation. J Med Case Rep 2019;13(1):109. [CrossRef]
[Pubmed]
6.
Al-Jawad M, Barakat M, Dahoud S, Lbabidi NA, Kawas A, Fattal F. Vulvar epidermal cyst in a 54-yearold virgin female: A very rare case report. Int J Surg Case Rep 2024;123:110226. [CrossRef]
[Pubmed]
7.
Kim HK, Kim SM, Lee SH, Racadio JM, Shin MJ. Subcutaneous epidermal inclusion cysts: Ultrasound (US) and MR imaging findings. Skeletal Radiol 2011;40(11):1415–9. [CrossRef]
[Pubmed]
8.
DiCarlo-Meacham AM, Dengler KL, Snitchler AN, Gruber DD. Clitoral epidermal inclusion cyst leading to anorgasmia: A case report and literature review. J Pediatr Adolesc Gynecol 2020;33(3):321–3. [CrossRef]
[Pubmed]
9.
Hoang VT, Trinh CT, Nguyen CH, Chansomphou V, Chansomphou V, Tran TTT. Overview of epidermoid cyst. Eur J Radiol Open 2019;6:291–301. [CrossRef]
[Pubmed]
10.
Bhalerao-Gandhi A, Kamale V, Tiwary A. Cysts and non-neoplastic swellings. In: Madnani N, editor. Atlas of vulvovaginal disease in darker skin types. CRC Press; 2023 p. 129–39.
11.
Konstantinova AM, Michal M, Kazakov DV. Vulvar ectopic tissues, cysts, and benign adnexal tumors. Gynecologic and Obstetric Pathology, Volume 1. 2019:109-25.
12.
Hoang MP, Kazakov DV, Selim MA. Cysts, glandular lesions, and others. In: Hoang M, Selim M, editors. Vulvar pathology. New York, NY: Springer; 2014. p. 355–83.
13.
Díaz de la Noval B, García Fernández I, Álvarez Fernández B. Bulky Bartholin’s gland cyst: Case report of an incidental finding. Case Rep Womens Health 2019;22:e00115. [CrossRef]
[Pubmed]
14.
Pehlivan M, Özbay PÖ, Temur M, Yılmaz Ö, Gümüş Z, Güzel A. Epidermal cyst in an unusual site: A case report. Int J Surg Case Rep 2015;8C:114-6. [CrossRef]
[Pubmed]
15.
Nigam JS, Bharti JN, Nair V, et al. Epidermal cysts: A clinicopathological analysis with emphasis on unusual findings. Int J Trichology 2017;9(3):108–12. [CrossRef]
[Pubmed]
16.
Choudhary S, Bansal R, Gupta R, et al. Imaging of the vulva: Spectrum of disease. Radiographics 2004;24(1):79–98.
17.
Outwater EK, Siegelman ES, Hunt JL. Imaging of the female perineum. Radiographics 2001;21(2):261–78.
18.
Sala E, Rockall AG, Rangarajan D, et al. MRI of benign and malignant vulvar disease. AJR Am J Roentgenol 2005;184(2):661–7.
19.
Kania LM, Guglielmo F, Mitchell D. Interpreting body MRI cases: Classic findings in pelvic MRI. Abdom Radiol (NY) 2020;45(9):2916–30. [CrossRef]
[Pubmed]
20.
Sibal M. Ultrasound evaluation of the vagina. In: Ultrasound in gynecology. Singapore: Springer; 2017. p. 187–201.
21.
Neto JA, Carmo B, Rodrigues AM, Silva JS. Skene’s gland duct cyst: Three cases in female newborns. BMJ Case Rep 2023;16(11):e256217. [CrossRef]
[Pubmed]
22.
Addley S, Sadeghi N, Smyth SL, Johnson C, Damato S, Soleymani Majd H. Bartholin’s gland carcinoma— the diagnostic and management challenges of a rare malignancy—A case report and review of current literature. Transl Cancer Res 2023;12(1):201–8. [CrossRef]
[Pubmed]
23.
Chang SD. Imaging of the vagina and vulva. Radiol Clin North Am 2002;40(3):637–58. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Gulnaz Shafqat - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Asra Shaikh - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Raima Kaleemi - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mudassir Ahmed - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Fatima Qaiser - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Gulnaz Shafqat et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}