 |
Case Report
Surgical management of vaginal suburethral mesh erosion with ultra-thick amniotic membrane augmentation
1 Assistant Professor, Dept. Physician Assistant Studies, University of Kentucky Health Science, Lexington, KY, USA
2 Student, Dept. Physician Assistant Studies, University of Kentucky Health Science, Lexington, KY, USA
Address correspondence to:
Magdalene Karon
MD, 160 N Eagle Creek Dr # 205, Lexington, KY 40509,
USA
Message to Corresponding Author
Article ID: 100214Z08MK2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Karon M, Scheitzach C. Surgical management of vaginal suburethral mesh erosion with ultra-thick amniotic membrane augmentation. J Case Rep Images Obstet Gynecol 2025;11(2):28–31.ABSTRACT
Introduction: The transvaginal mesh sling is a primary consideration for urinary stress incontinence. However, the mesh is sharp and can erode through the vagina mucosa, making intercourse painful for both partners. Proximity to the urethra can also contribute to urethral and urinary infections which complicates the healing process of the open wound area. The exposed mesh necessitates resection with debridement of surrounding tissue. Primary closure may be difficult and cause fibrosis. Amniotic membrane is known to have anti-inflammatory and anti-scarring properties, which may facilitate closure and prevent post-surgical healing delays. Herein, we evaluate the adjunctive use of ultra-thick amniotic membrane (AM) to augment the surgical repair site for a complex mesh exposure.
Case Report: A 50-year-old Caucasian female (gravida 2, para 2) presented with vaginal mesh exposure (4 mm by 2 mm by 5 mm) from a transvaginal sling, placed approximately a year ago for stress urinary incontinence. The chief complaints were pain, bleeding, and dyspareunia. The patient underwent transvaginal excision of the exposed mesh and removal of neighboring scar and non-viable tissue. The vaginal defect with suture and adjunctive ultra-thick AM was incorporated into the closure. At one month post-op, the operative site was completely covered with vaginal mucosa and she did not have pain, bleeding, symptoms of prolapse or urinary incontinence. Six months later, the patient had no complaints.
Conclusion: This case report demonstrates the utilization and benefits of using ultra-thick AM augmentation in the setting of a vaginal mesh erosion complication.
Keywords: Amniotic membrane, Mesh complications, Mesh erosion, Surgical revision
Introduction
Transvaginal meshes for pelvic organ prolapse were ordered to be removed from the United States market by the FDA in April 2019. Still, transvaginal mesh sling remains in use for correction of stress urinary incontinence in the United States. The mesh sling can successfully correct urethral hypermobility and, thus, stress urinary incontinence; however, complications that arise from erosion can be harmful to surrounding structures [1]. Thus, the tissue has difficulty healing and warrants resection, debridement of surrounding non-viable tissue, and surgical closure [2]. The surgical repair of mesh erosion can be complicated by lack of viable surrounding tissue, constant presence of vaginal flora, and co-morbidities for poor wound healing [3]. In such cases, utilization of adjunctive treatments or surgical techniques to facilitate the closure of the defect would be beneficial. One such adjunctive treatment is amniotic membrane (AM), which may act as a protective barrier but is also known to have regenerative properties such as anti-inflammatory and anti-scarring properties. Accordingly, AM has been used in various clinical applications, such as dermal and ocular wounds, to help promote accelerated and regenerative healing. While the AM originates from the obstetrical branch of our specialty, its expanding multidisciplinary applications underscore its potential to significantly contribute to the gynecological domain as well. Herein, we evaluate the adjunctive use of ultra-thick AM to augment the surgical repair site for a complex mesh exposure.
Case Report
A 50-year-old Caucasian female (gravida 2, para 2) presented with vaginal mesh exposure from a transvaginal sling, placed approximately a year ago for stress urinary incontinence. The chief complaints were pain, bleeding, and dyspareunia. Examination revealed an exposed mesh defect that was 4 mm by 2 mm by 5 mm.
Treatment If Relevant
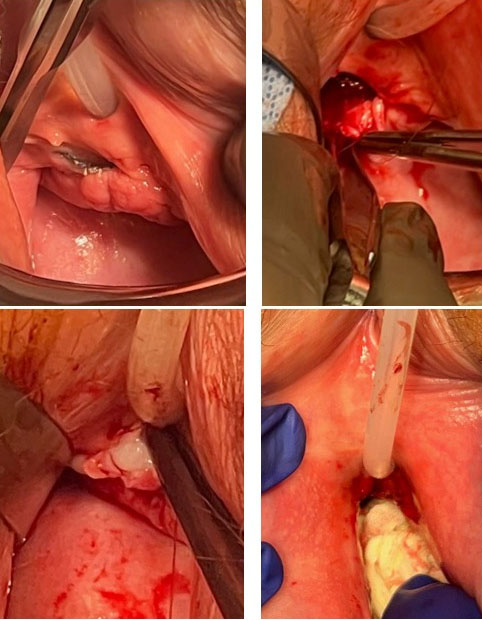
The patient underwent transvaginal excision of the exposed mesh and removal of neighboring scar and non-viable tissue. The vaginal defect was closed with 4-0 poliglecaprone 25 suture (Monocryl; Johnson & Johnson, New Brunswick, NJ) and undyed poliglecaprone 25 suture. Adjunctive ultra-thick AM (Neox RT; BioTissue, Miami, FL) was incorporated into the tissue defect after the mesh was removed and oversewn with two layers of poliglecaprone 25 suture (Figure 1). Care was taken to avoid trauma to the urethra and its meatus.
Outcome and Follow-up
Patient’s recovery was assessed at one month post-operatively and then via telehealth for follow-up, as she was in good health and did not have any complaints. At one month post-op, the operative site was completely covered with vaginal mucosa. There was no granulation tissue present, which can lead to bleeding and can be tender. She had no post-operative urethritis or cystitis. Only one preoperative prophylactic intravenous (IV) dose of cephalosporin was used. The patient was able to resume intercourse one month after the procedure. She did not have pain, bleeding, symptoms of prolapse or of urinary incontinence/leakage as before. Physical examination did not reveal scarring in the operative site and tissues had normal turgor. Six months later, the patient had no complaints.
Discussion
Amniotic membrane is often considered to be a biological bandage when used in the clinical context of promoting wound healing by acting as a mechanical protective barrier and providing anti-inflammatory and anti-scarring properties to modulate the healing process. Numerous reports have also been published reporting the successful repair of vaginal fistula using placental/umbilical allografts [4],[5]. Posterior colporrhaphy and anal sphincteroplasty procedures have also been complemented with placental/umbilical allograft to help prevent frequent occurrence of this defect [6],[7],[8],[9]. This case report adds to the available literature and demonstrates successful repair of a vaginal mesh erosion with adjunctive ultra-thick AM. Such technique may be considered in cases with extensive tissue damage or in patients with co-morbidities for poor wound healing.
The patient expressed great satisfaction with the procedure, and felt relief to be free from the pain, bleeding, and dyspareunia that had previously affected her quality of life. She was also happy that the healing process occurred so fast, and no longer felt the need to return for follow-up visits as the operative site was completely covered without symptoms as early as one-month post-operation.
Conclusion
Vaginal mesh erosions and fistulas can be a healing challenge and sometimes require multiple procedures with recurrence of open wounds. Vaginal location makes healing challenging due to constant presence of vaginal flora and colon bacteria cross-contamination. This case report suggests complementing vaginal surgical repairs with amniotic membrane (AM) may promote healing without prolonged granulation reaction and excessive fibrosis.
REFERENCES
1.
Lin YH, Lee CK, Chang SD, Chien PC, Hsu YY, Tseng LH. Focusing on long-term complications of mid-urethral slings among women with stress urinary incontinence as a patient safety improvement measure: A protocol for systematic review and meta-analysis. Medicine (Baltimore) 2021;100(24):e26257. [CrossRef]
[Pubmed]

2.
Gomes CM, Carvalho FL, Bellucci CHS, Hemerly TS, Baracat F, de Bessa J Jr, et al. Update on complications of synthetic suburethral slings. Int Braz J Urol 2017;43(5):822–34. [CrossRef]
[Pubmed]
3.
Artsen AM, Liang R, Meyn L, Bradley MS, Moalli PA. Dysregulated wound healing in the pathogenesis of urogynecologic mesh complications. Sci Rep 2023;13(1):21437. [CrossRef]
[Pubmed]
4.
Clark J, Tulenko T, Echols K. 83 Dehydrated human amniotic membrane and amniotic fluid for the treatment of rectovaginal fistulas. American Journal of Obstetrics & Gynecology 2021;224(6):S796. [CrossRef]
5.
Barski D, Gerullis H, Ecke T, Varga G, Boros M, Pintelon I, et al. Repair of a vesico-vaginal fistula with amniotic membrane – Step 1 of the IDEAL recommendations of surgical innovation. Cent European J Urol 2015;68(4):459–61. [CrossRef]
[Pubmed]
6.
Karon M. Viable umbilical tissue use in laparoscopic myomectomy: Study design and short-term post-operative outcomes [29Q]. Obstetrics & Gynecology 2018;131:192S. [CrossRef]
7.
Karon M, Duan-Arnold Y. Flowable dehydrated amniotic membrane allograft augments McDonald cerclage in high-risk women for preterm birth prevention, a case series. J Women Health Care Issues 2020;3(4). [CrossRef]
8.
Karon M, Duan-Arnold Y. Flowable dehydrated amniotic membrane allograft augments McDonald cerclage in high-risk women for preterm birth prevention, a case series. J Women Health Care Issues 2020;3(4). [CrossRef]
9.
Karon M, Trimpe DM. Novel use of viable cryopreserved umbilical tissue in posterior colporrhaphy in high risk patients [16J]. Obstetrics & Gynecology 2019;133:111S. [CrossRef]
SUPPORTING INFORMATION
Author Contributions
Magdalene Karon - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Cameron Scheitzach - Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 2025 Magdalene Karon.. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}