 |
Case Report
A rare case of giant mature ovarian teratomas: A case report
1 MBBS, Senior House Officer, Department of Obstetrics and Gynecology, Queen Elizabeth Hospital, Barbados
Address correspondence to:
Keturah Murray
Queen Elizabeth Hospital, Martindales Road, St Michael,
Barbados
Message to Corresponding Author
Article ID: 100217Z08KM2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Murray K. A rare case of giant mature ovarian teratomas: A case report. J Case Rep Images Obstet Gynecol 2025;11(2):42–46.ABSTRACT
Mature cystic ovarian teratomas, also known as dermoid cysts, are common benign ovarian neoplasms. These tumors are composed of tissues from all three germ cell layers: ectoderm, mesoderm, and endoderm. Once diagnosed, prompt management is essential due to risk of complications such as torsion and rupture. Here we present the case of a 14-year-old female who presented with abdominal pain and was found to have a giant ovarian cysts. She underwent successful surgical management and had an unremarkable postoperative course, with no complications noted at follow-up.
Keywords: Cyst, Mature teratoma, Ovary
Introduction
Teratomas are germ cell tumors; they can be divided into two categories; mature and immature [1]. Mature teratomas (MCT) are benign, in contrast immature teratomas are malignant [2]. Mature teratomas are considered the most common benign ovarian tumor in childhood and adolescence [1]. Due to advances in imaging techniques, especially ultrasonography, diagnosing this disease is much easier today, and finding cysts larger than 10 cm is very rare [3]. Although often asymptomatic, large neoplasms can cause abdominal and flank pain [4]. Complications include but are not limited to torsion, rupture, and risk of malignant transformation [5].
Case Report
A 14-year-old nulliparous female with without any preexisting comorbidities presented to the Accident and Emergency Department (A&E) of the Queen Elizabeth Hospital, Barbados, with a four-day history of stabbing left sided abdominal pain. It was sudden in onset and constant. There were no exacerbating factors; however, the pain was relieved significantly with analgesia. She denied nausea, vomiting, or flu-like symptoms. There were no urinary symptoms or abnormal vaginal discharge. Her bowel and bladder function were normal, and she denied any back pain. She had never been sexually active. There was no history of vaginal infections.
Examination revealed an obese adolescent; her body mass index (BMI) was 41 kg/m2. Her abdomen was soft and nontender, with a mass arising from the pelvis to the level of the umbilicus. Acanthosis nigricans was present in the neck folds and striae were seen on the arms, back, and abdomen. The cardiovascular and respiratory examinations were normal. Her urine pregnancy test was negative; the urinalysis was not suggestive of infection.
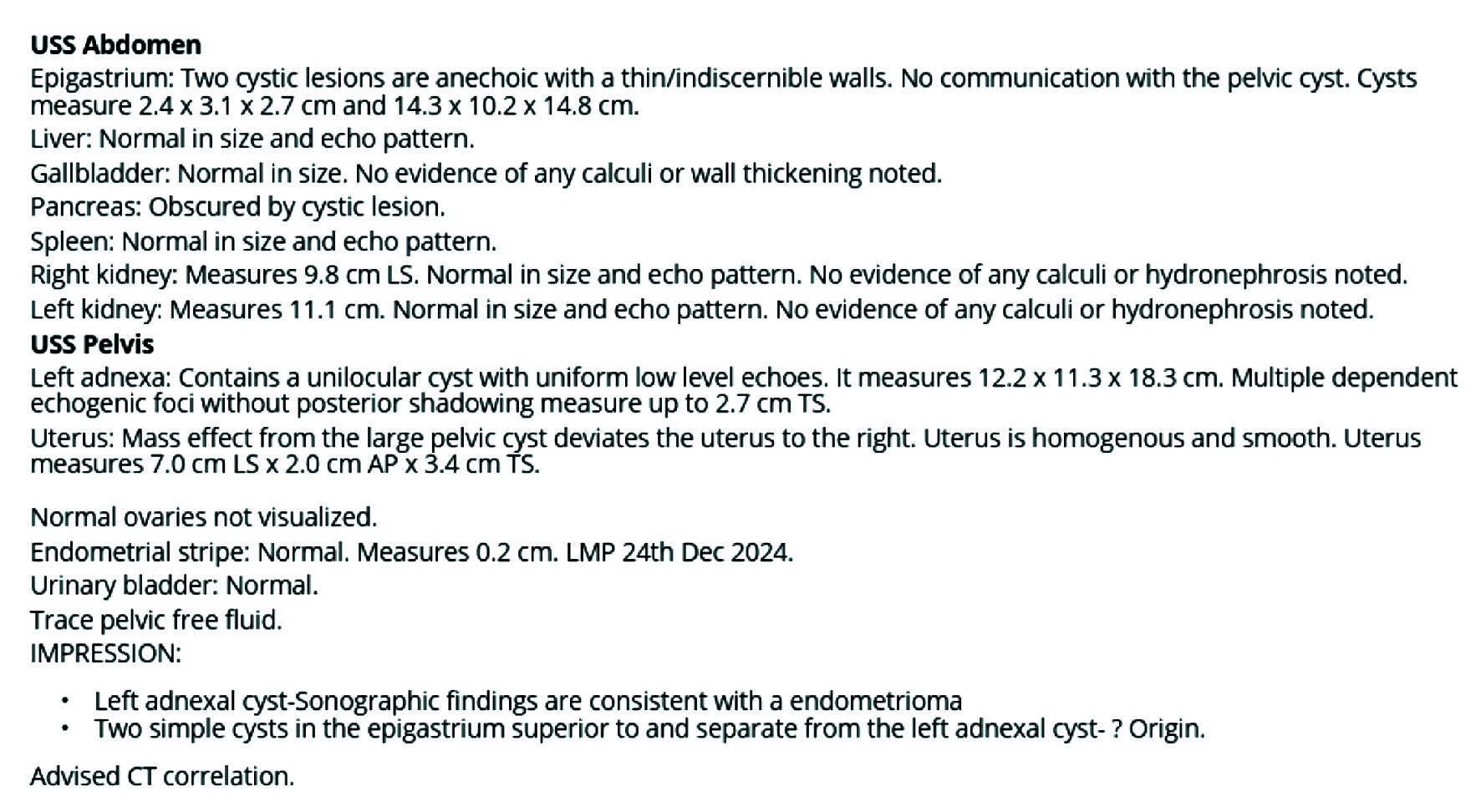
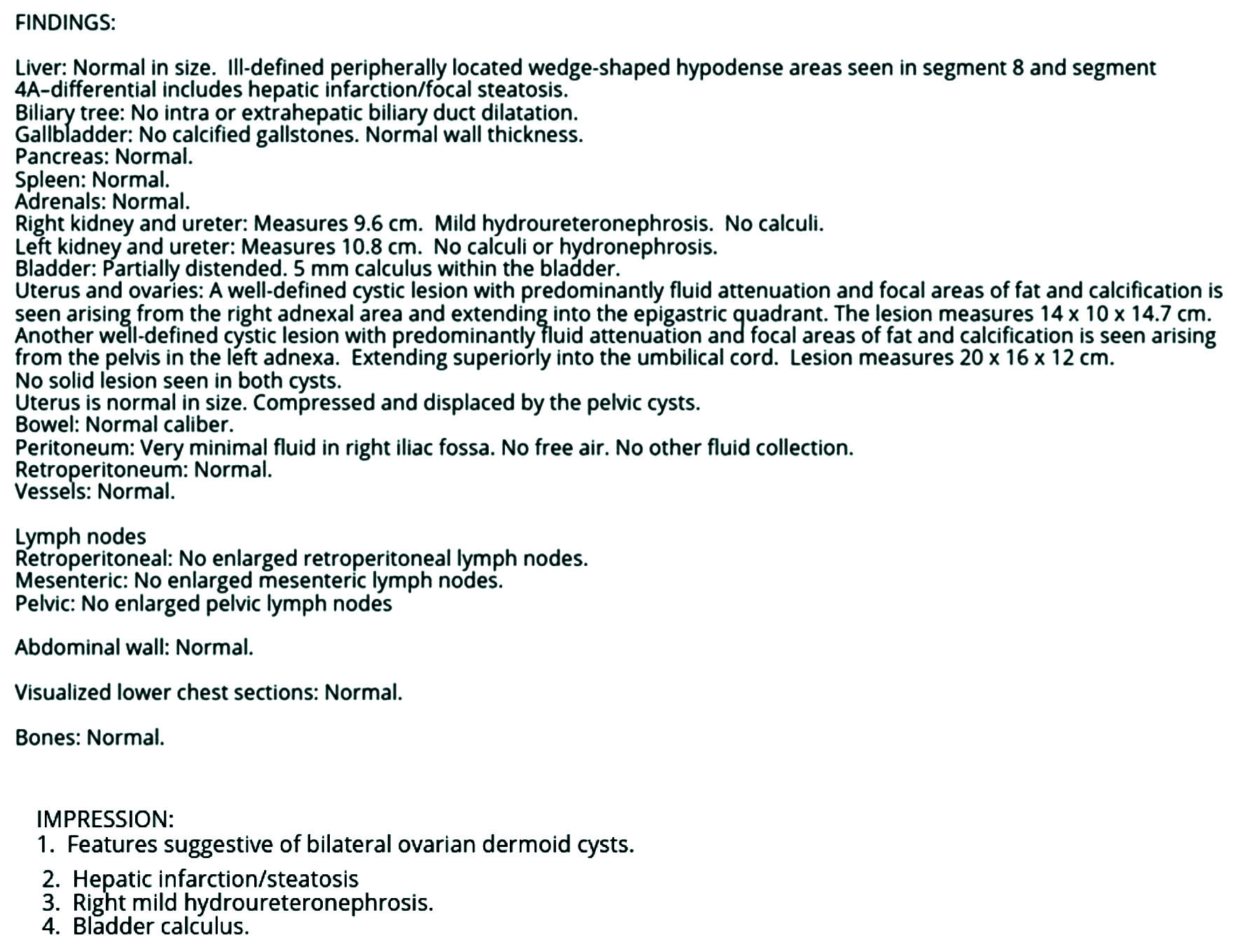
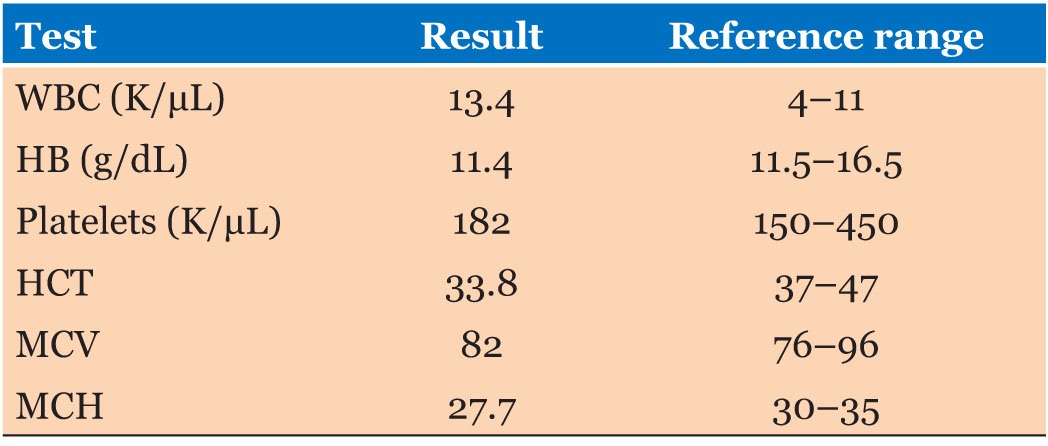
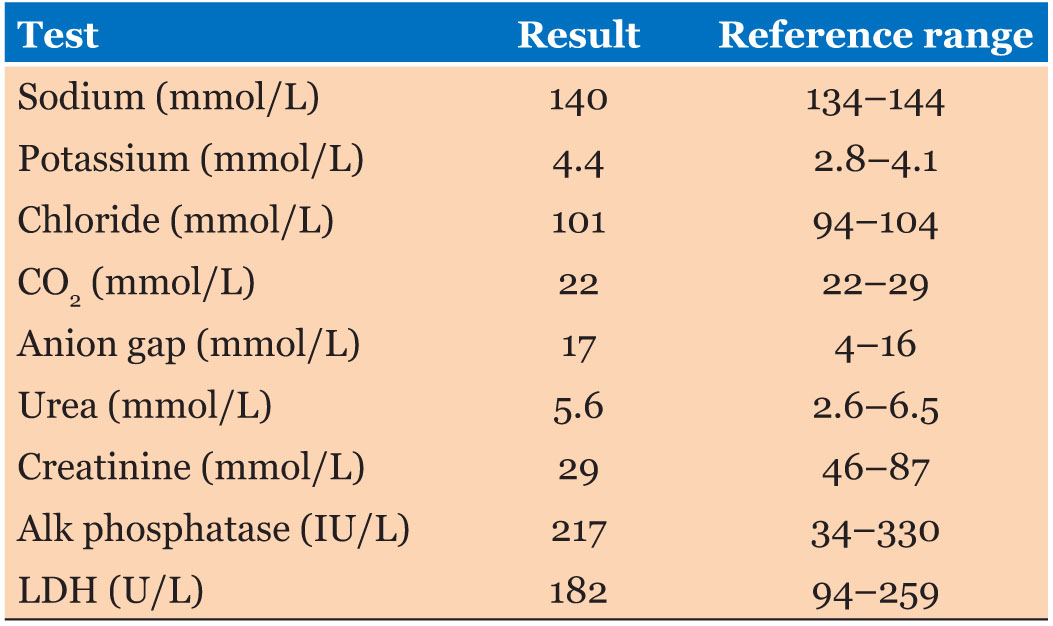
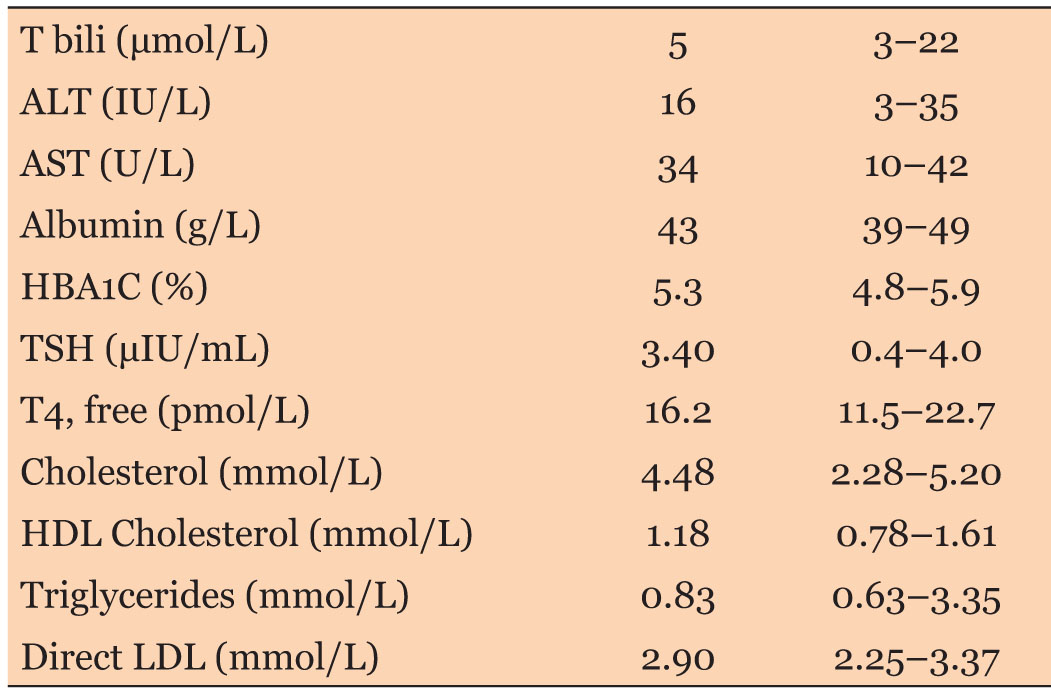
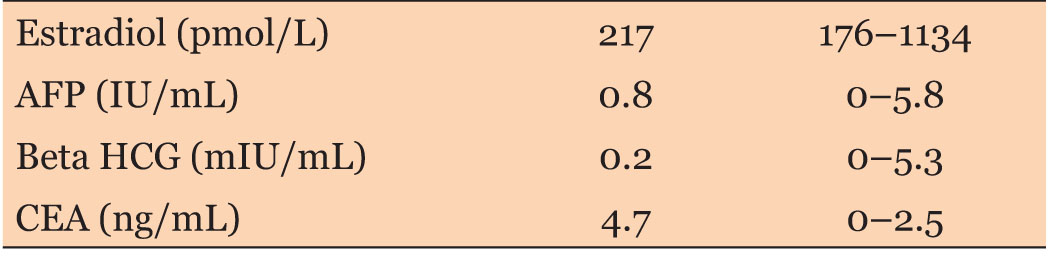
An ultrasound (US) and subsequent contrast enhanced (oral and intravenous) computed tomography (CT) scan of the abdomen and pelvis were performed. The results are as seen below (Box 1 and Box 2 and Figure 1). Her laboratory results are as seen in Table 1, Table 2, Table 3, Table 4, of note her tumor markers were normal. She was admitted to facilitate multidisciplinary review by the pediatrics, general surgery, urology, and gynecology teams and to plan for definitive surgical management.
In the context of her elevated BMI and associated clinical findings, the general surgery team considered the hepatic changes to be more consistent with features of metabolic syndrome rather than hepatic infarction. Laboratory investigations were initiated by the pediatrics team, along with dietitian referral and arrangements were made for outpatient participation in a pediatric exercise program. The results, as seen in Table 3, were normal.
The urology team advised that the hydroureteronephrosis was expected to resolve following cyst removal and, in the interim, recommended conservative management. Following resolution of the acute issues, she was discharged with a scheduled date to return for elective surgery.
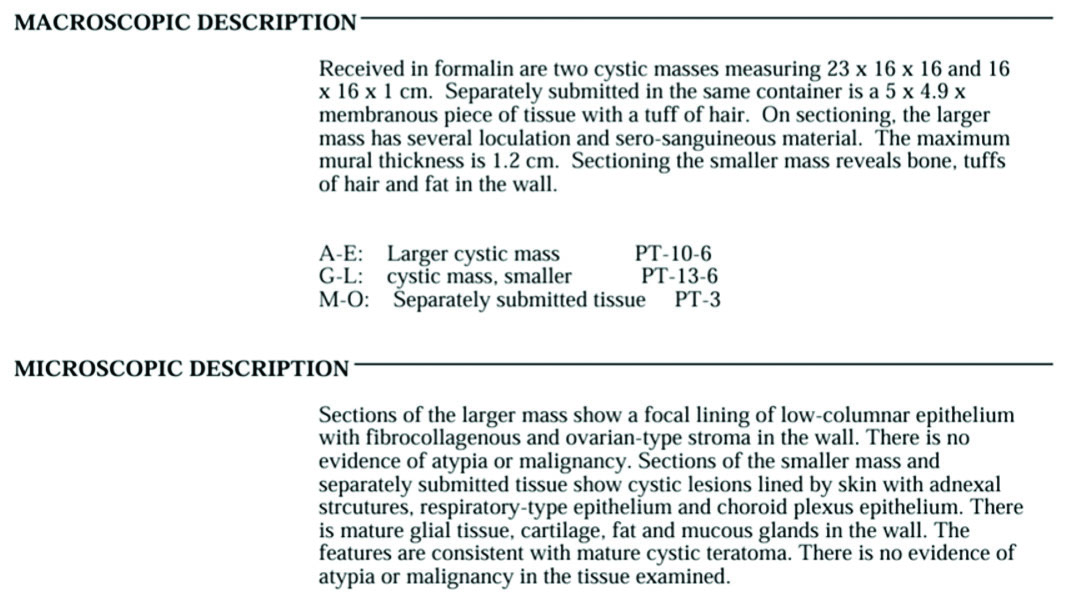
A laparotomy followed by bilateral ovarian cystectomy was performed, using a midline incision, under general anesthesia. Both ovaries were significantly enlarged (Figure 2); right ovary 23 × 16 cm and left ovary 16 × 16 cm. Each ovarian cyst capsule was incised and the cysts removed. Hemostasis was achieved and the abdominopelvic cavity was lavaged using warm saline. The estimated blood loss was 500 mL.
Her post-operative course was uneventful, and she was discharged on the third post-operative day. At her review six weeks later, in the gynecology outpatient clinic. She was well and reported no issues. Her histopathology report (Box 3) confirmed mature cystic teratomas. There was no evidence of atypia or malignancy.


Discussion
Abdominal pain is a common presenting complaint in adolescent females. A thorough history, examination, and tailored investigations are required as the differential diagnoses are numerous.
As seen in this case, when symptomatic, ovarian masses in children commonly present with abdominal pain. This may be described as diffuse and nonspecific, additionally other pressure-related symptoms may be present [1]. Ovarian masses may also be identified incidentally when investigating adolescents for reasons such as irregular menstrual bleeding [2]. Mature cystic teratomas (MCTs) or dermoid cysts are the most common ovarian neoplastic lesions found in adolescents. These masses are a benign type of germ cell tumor that arise from totipotent cells in the ovary which develop into fully differentiated ectodermal, mesodermal, and endodermal tissue [3].
The dimensions of each cyst measured greater than 10 cm, thus meeting the criteria for definition of a giant ovarian cyst (GOC) [4]. Giant ovarian cysts are a rare occurrence, when identified, this pathology is seen more frequently in the third to sixth decade of life [4]. It was unusual therefore for this diagnosis to be made in our patient at just 14 years old. Giant ovarian cysts have the potential to cause serious complications such as torsion, suppuration, obstruction, and perforation necessitating urgent admission [5].
Cysts that reach such a giant size are almost always benign, but careful preoperative testing should be carried out due to the suspicion of malignancy [6]. Useful markers for the investigation of ovarian neoplasms in adolescents include alpha-fetoprotein (AFP), lactate dehydrogenase (LDH), beta subunit of human chorionic gonadotropin (β-hCG), cancer antigen 125 (CA-125) and inhibin. The diagnostic value of tumor markers is higher when the results are combined with clinical and radiological information [7]. The patient had an ultrasound which revealed large cysts, and a computed tomography (CT) scan was done to further evaluate these masses.
While the definitive diagnosis of an ovarian cyst requires surgical exploration and a histopathological study, the contribution of imaging to the diagnosis is crucial for determining the origin and characteristics of the cyst [8]. The main imaging modality for evaluating ovarian and adnexal masses is ultrasonography (US), which allows accurate identification in approximately 90% of cases. It has the advantage of being readily available, inexpensive, easy to perform, and has no ionizing radiation [9].
Although a pelvic US is the single most effective way of evaluating an ovarian mass, transvaginal ultrasonography (TVS) is preferable because of its increased sensitivity over transabdominal ultrasound (TAS) [10]. Leibman et al. found that when the two examinations were compared for definition of the internal architecture of a pelvic mass, the TVS showed more detail in 81% of women [11]. Our patient had a BMI of 41 kg/m2. Obesity may limit the sensitivity of TAS. In this study, more detail was seen on TVS in two-thirds of the obese patients [11]. Therefore, though TVS may have proven useful in this case, this was deferred due to the patient’s virgo intacta status.
The presence of unilocular cyst on her US was reassuring. Other benign features on imaging include smooth multilocular tumor, solid component <7 mm in diameter, the presence of acoustic shadows and no detectable doppler signal. In the absence of malignant features (irregular solid tumor, irregular multilocular mass >10 cm in diameter, ≥4 papillary structures, ascites, high doppler signal) the mass can be confidently considered benign [12]. Her clinical investigation and radiological tests excluded any signs of malignancy.
Given the size of the cysts, bilateral ovarian cystectomies were done via laparotomy. The decision to proceed with operative management of ovarian masses in children can be challenging and every attempt should be made to preserve as much normal ovarian tissue as possible [2]. Giant ovarian cysts always require resection, because of associated symptoms due to mass effect, difficulties in establishing the origin of the mass and the risk of malignancy [6]. Additionally, a true benign neoplasm of ovary (e.g., serous, mucinous, teratoma) does not resolve spontaneously [13].
Laparoscopic ovarian cystectomy can be offered for the management of presumed benign ovarian cysts. Advantages include better cosmetic results, less blood loss, less analgesic requirements, faster recovery, and shorter hospitalization time [14]. However, in the case of GOC, decompression of the mass (usually ultrasound guided) is required prior to removal [6]. On clinical examination, she had a mass that was palpable to the level of the umbilicus, however imaging revealed two cysts, one extending into the epigastric region. Mature teratomas are treated by resection alone. They are not malignant, though they may be bilateral in as many as 10% of cases [15].
There is no standard of care as to the follow-up for girls with a benign ovarian mass [2]. Given her young age at presentation, she is at an increased risk of recurrence of the MCT. In a study by Song et al., bilaterality, multilocularity, and younger age at first diagnosis were reported [16]. In the literature, it is observed that MCT recurrence rates are 3–4% [17].
Conclusion
Ovarian masses, though uncommon in childhood and adolescence, are an important differential for causes of abdominal pain in this age group. Laboratory and imaging investigations constitute a key role in the investigation of these patients. When intervention is required, conservative surgery is paramount in the development of normal puberty and in optimizing future fertility.
REFERENCES
1.
Kassidi F, Moukit M, Ait El Fadel F, El Hassani ME, Guelzim K, Babahabib A, et al. Successful management of a giant ovarian cyst: A case report. Austin Gynecol Case Rep 2017;2(1):1012.

2.
Barton SE, Kurek KC, Laufer MR. Recurrent bilateral serous cystadenomas in a premenarchal girl: A case report and literature review. J Pediatr Adolesc Gynecol 2010;23(1):e27–9. [CrossRef]
[Pubmed]
3.
Gkrozou F, Tsonis O, Vatopoulou A, Galaziou G, Paschopoulos M. Ovarian teratomas in children and adolescents: Our own experience and review of literature. Children (Basel) 2022;9(10):1571. [CrossRef]
[Pubmed]
4.
Albers CE, Ranjit E, Sapra A, Bhandari P, Wasey W. Clinician beware, giant ovarian cysts are elusive and rare. Cureus 2020;12(1):e6753. [CrossRef]
[Pubmed]
5.
Yeika EV, Efie DT, Tolefac PN, Fomengia JN. Giant ovarian cyst masquerading as a massive ascites: A case report. BMC Res Notes 2017;10(1):749. [CrossRef]
[Pubmed]
6.
Murawski M, Gołębiewski A, Sroka M, Czauderna P. Laparoscopic management of giant ovarian cysts in adolescents. Wideochir Inne Tech Maloinwazyjne 2012;7(2):111–3. [CrossRef]
[Pubmed]
7.
Birbas E, Kanavos T, Gkrozou F, Skentou C, Daniilidis A, Vatopoulou A. Ovarian masses in children and adolescents: A review of the literature with emphasis on the diagnostic approach. Children (Basel) 2023;10(7):1114. [CrossRef]
[Pubmed]
8.
Amara A, Adem A, Salhi H, El Magroud M, Zaari N, Ammor A, et al. Giant serous cystadenoma in an adolescent: A case report. SAGE Open Med Case Rep 2024;12:2050313X241296296. [CrossRef]
[Pubmed]
9.
Pramana C, Almarjan L, Mahaputera P, Wicaksono SA, Respati G, Wahyudi F, et al. A giant ovarian cystadenoma in a 20-year-old nulliparous woman: A case report. Front Surg 2022;9:895025. [CrossRef]
[Pubmed]
10.
Gwanzura C, Muyotcha AF, Magwali T, Chirenje ZM, Madziyire MG. Giant mucinous cystadenoma: A case report. J Med Case Rep 2019;13(1):181. [CrossRef]
[Pubmed]
11.
Leibman AJ, Kruse B, McSweeney MB. Transvaginal sonography: Comparison with transabdominal sonography in the diagnosis of pelvic masses. AJR Am J Roentgenol 1988;151(1):89–92. [CrossRef]
[Pubmed]
12.
Abramowicz JS, Condous G, Timmerman D. Ovarian mass-differentiating benign from malignant. Why the International Ovarian Tumour Analysis rules should be implemented in Australasia. Australas J Ultrasound Med 2018;21(3):121–4. [CrossRef]
[Pubmed]
13.
Patil TA, Limaye H, Mehta A. Case report of a huge serous ovarian cystadenoma in post hysterectomy woman. The New Indian Journal of OBGYN 2018;5(1):64–66.
14.
Ateş O, Karakaya E, Hakgüder G, Olguner M, Seçil M, Akgür FM. Laparoscopic excision of a giant ovarian cyst after ultrasound-guided drainage. J Pediatr Surg 2006;41(10):E9–11. [CrossRef]
[Pubmed]
15.
Schultz KAP, Ness KK, Nagarajan R, Steiner ME. Adnexal masses in infancy and childhood. Clin Obstet Gynecol 2006;49(3):464–79. [CrossRef]
[Pubmed]
16.
Song YN, Zhu L, Lang JH. Recurrent mature ovarian teratomas: Retrospective analysis of 20 cases. [Article in Chinese]. Zhonghua Yi Xue Za Zhi 2007;87(17):1184–6.
[Pubmed]
17.
Alanbay İ, Çoksuer H, Ercan M, Karaşahin E, Keskin U, Başer İ. Multiple recurrent mature cystic teratoma of the same ovary: A case report and literature review. Aynı overin multipl matür rekürrent kistik teratomu: Vaka sunumu ve literatürün gözden geçirilmesi. 2011. [Available at: https://acikerisim.aku.edu.tr/xmlui/handle/11630/1956?locale-attribute=en]
SUPPORTING INFORMATION
Author Contributions
Keturah Murray - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthor declares no conflict of interest.
Copyright© 2025 Keturah Murray. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}