 |
Case Report
Delayed presentation of vaginal cuff dehiscence and evisceration of bowel after laparoscopic hysterectomy and adjuvant radiation therapy
1 Resident PGY2, HCA East Florida Division, Obstetrics and Gynecology, HCA Northwest Medical Center, Margate, Florida, United States
Address correspondence to:
Maral Darya
7253 NW 108th Way, Parkland, Florida, Zip code 33076,
United States
Message to Corresponding Author
Article ID: 100221Z08MD2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Darya M, Budhwani S, Grekos V, Ortiz-Gonzalez K. Delayed presentation of vaginal cuff dehiscence and evisceration of bowel after laparoscopic hysterectomy and adjuvant radiation therapy. J Case Rep Images Obstet Gynecol 2026;12(1):1–4.ABSTRACT
Introduction: Total hysterectomy (TH) is one of the most commonly performed gynecologic procedures, with complications including genitourinary or gastrointestinal injury, bleeding, infection, and rarely vaginal cuff dehiscence (VCD). Vaginal cuff dehiscence is an uncommon but potentially life-threatening complication, particularly associated with laparoscopic hysterectomy and may present with bowel evisceration requiring urgent intervention.
Case Report: We present the case of a woman in her 50s with a history of radical hysterectomy and adjuvant radiation for cervical cancer, who presented with acute abdominal pain and small bowel evisceration through the vagina. Emergent laparotomy was performed with small bowel resection and anastomosis, followed by transvaginal repair of the vaginal cuff.
Conclusion: This case highlights the importance of early recognition and individualized management based on patient status and intraoperative findings, with careful assessment of bowel viability prior to cuff closure. In addition to surgical outcomes, psychological consequences following such events can be significant, emphasizing the need for early counseling.
Keywords: Bowel evisceration, Emergency laparotomy, Laparoscopic surgery, Total hysterectomy, Vaginal cuff dehiscence
Introduction
Total hysterectomy (TH) is among the most frequently performed gynecologic procedures. Common complications include injuries to the genitourinary and gastrointestinal tract, bleeding, infection, and vaginal cuff dehiscence (VCD). Vaginal cuff dehiscence is an uncommon but potentially life-threatening complication following total hysterectomy [1]. It involves a partial or complete separation of the anterior and posterior vaginal cuff edges, which can result in the protrusion of intraperitoneal contents, most commonly the distal ileum [2]. The overall incidence is approximately 0.53% but the precise incidence is difficult to determine [2].
Laparoscopic hysterectomies are associated with a 3 to 13 folds increased risk of vaginal cuff dehiscence compared to open procedure [2]. This is a surgical emergency requiring immediate recognition and intervention as mortality rate increases to 5.6% due to the risk of sepsis and bowel ischemia from compromised blood flow [2].
Case Report
Female patient in her 50s, gravida 4 para 4 with history of cervical cancer status post robotic radical hysterectomy and adjuvant radiation therapy 17 years ago presented to our emergency department with acute severe abdominal pain and bowel prolapse through the introitus. This patient underwent laparoscopic repair of vesicovaginal fistula a year ago prior to presentation, a procedure that is not typically associated with subsequent vaginal cuff dehiscence. She reported pain getting progressively worse throughout that day followed by vomiting. She reported that severe abdominal pain started immediately after an episode of coughing.
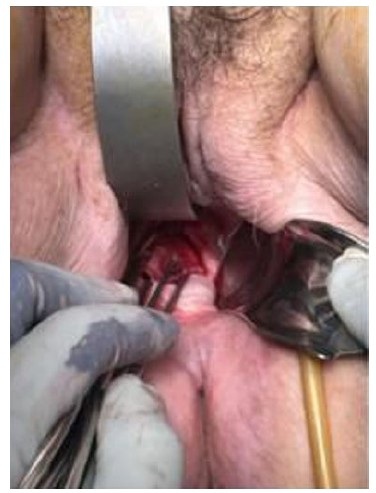
On examination, the patient appeared uncomfortable. The eviscerated bowel appeared strangulated/ischemic (Figure 1). The patient remained hemodynamically stable. Computed tomography (CT) showed evidence of pelvic floor prolapse with peritoneal fat and nondilated loops of small bowel and rectosigmoid colon extending through the vagina (Figure 2).
The patient was taken to the operating room for emergent laparotomy by the gynecology and general surgery team. The time interval from emergency room presentation to the operating room was about 2 hours. After reduction of eviscerated bowel, a midline vertical incision was made, and the entire small bowel was inspected. As already known from preoperative examination, the eviscerated bowel was noted to be strangulated, which required small bowel resection followed by anastomosis. Due to the patient’s body habitus and short vaginal canal, it was not possible to repair the defect adequately through a transabdominal approach. Attention was then directed to the vaginal cuff transvaginally and was noted to be 5 cm in length (Figure 3). Vaginal cuff was repaired with 5 interrupted sutures using absorbable suture, 1-0 polyglactin 910 (Vicryl). Peritonealization was not performed and there was no indication for drain placement. There were no intraoperative complications. The patient received postoperative antibiotics with Pipercillin and Tazobactam.
The patient recovered well and was discharged on post-operative day 7. At her 2 week postoperative appointment, examination revealed a healthy vaginal vault with no defects. We will continue to monitor the patient on an outpatient basis as part of routine follow-up.


Discussion
Vaginal cuff dehiscence is a rare complication of pelvic surgery. Since the first report in 1864, only about 100 cases have been documented in the literature [3].
A recent study of 4864 hysterectomies reported VCD rates of 0.706% for laparoscopic hysterectomy, 0.224% for robotic surgery, and 0.233% for laparotomy and notably, laparoscopic VCD often developed early with minimal external force [4].
Evidence indicates that approximately 70% of affected patients are postmenopausal women which is associated with reduced vaginal wall vascularity and atrophy [3]. Following pelvic surgery, vaginal cuff dehiscence has been reported from as early as three days postoperatively to as late as 30 years later [3]. This case is novel due to its exceptionally late presentation of VCD in a previously irradiated pelvis and history of multiple pelvic surgeries in the setting of obesity. Additionally, due to her extensive surgical history resulting in a shortened vaginal canal, it required a combined open/vaginal approach for adequate management.
Risk factors include poor surgical technique, postoperative infection, hematoma, resumption of sexual intercourse before adequate healing, advanced age, prior radiotherapy, corticosteroid therapy, trauma, history of vaginoplasty, and use of Valsalva maneuver [5]. To reduce the risk of vaginal cuff dehiscence, initiating vaginal brachytherapy no earlier than six weeks post-hysterectomy allows sufficient time for cuff healing [5]. Our patient has significant risk factors including postmenopausal state, history of robotic assisted laparoscopic hysterectomy followed by vaginal brachytherapy years ago and most recently a laparoscopic repair of vesicovaginal fistula.
Transvaginal evisceration is a rare but potentially life-threatening condition that requires urgent surgical intervention. For vaginal cuff repair, both transvaginal and transabdominal approaches can be used. However, before closing the vaginal defect, the bowel should be carefully evaluated for possible resection and anastomosis. In our case, we performed an emergency laparotomy, resected necrotic small bowel followed by anastomosis, and repaired the vaginal cough via transvaginal approach.
The management should be tailored to the patient’s status and the surgeon’s judgment. Ma et al. suggest organ repositioning without anesthesia in the emergency setting which offers several advantages: immediate relief from the protrusion, improved visualization for subsequent transvaginal repair and potential reduction in the risk of ischemia and necrosis of the eviscerated organs [1]. For medically stable patients without complications, vaginal repair is an appropriate option, offering cost-effectiveness and avoiding an additional surgical incision [1]. However, in women with very narrow vagina or significant obesity, the transvaginal approach can be challenging due to limited visualization therefore laparoscopy offers advantages [1]. When necrotic bowel resection is required or when peritonitis or intraperitoneal hematoma is suspected, an abdominal approach is warranted.
Psychological consequences following surgery can be profound, often extending beyond physical recovery. Studies have shown than patients undergoing colorectal resection demonstrate a higher incidence of anxiety, depression, and post-traumatic stress disorder compared to the general population with younger individuals and female patients particularly at risk [6]. Early recognition and timely referral for counseling and psychosocial support play a crucial role in promoting emotional recovery and improving overall quality of life.
Conclusion
Vaginal cuff dehiscence and bowel evisceration is a rare but potentially fatal complication following hysterectomy that necessitates immediate recognition and prompt surgical management. This case highlights the importance of maintaining a high index of suspicion in post-hysterectomy patients presenting with acute abdominal pain, particularly those with risk factors such as prior radiation, advanced age, and history of laparoscopic pelvic surgery. A multidisciplinary approach involving both gynecology and general surgery teams is crucial for optimal outcomes, especially when bowel ischemia or necrosis is suspected. Surgical management should be individualized based on patient factors and intraoperative findings, ensuring both adequate repair of the vaginal cuff and assessment of bowel viability. Beyond physical recovery, clinicians should also address the psychological impact through early counseling and long-term follow-up to promote holistic recovery and quality of life.
REFERENCES
1.
Ma X, Cao DY, Dai YX. Experience in the management of vaginal cuff dehiscence and evisceration: A retrospective 37-year single-center study. Front Surg 2022;9:880875. [CrossRef]
[Pubmed]

2.
Lim ET, Stylianides N, Craciunas L, Tsampras N. Vaginal vault dehiscence with small bowel evisceration, bowel necrosis, and intra-abdominal haemorrhage: A case report. J Surg Case Rep 2024;2024(4):rjae191. [CrossRef]
[Pubmed]
3.
Ali KY, Mohamud SA. Delayed presentation of vaginal cuff dehiscence and evisceration of a loop of bowel nine months after laparoscopic hysterectomy: A case report. International Journal of Surgery Case Reports 2022;95:107291. [CrossRef]
4.
Ikki A, Aoki Y, Kanno M, Tsumura S, Fusegi A, Abe A, et al. Comparison of the incidence of vaginal cuff dehiscence by hysterectomy route and type based on experienced surgeons' outcome. Int J Gynaecol Obstet 2025;170(1):222–32. [CrossRef]
[Pubmed]
5.
Cattaneo R 2nd, Bellon M, Elshaikh MA. Vaginal cuff dehiscence after vaginal cuff brachytherapy for uterine cancer. A case report. J Contemp Brachytherapy 2013;5(3):164–6. [CrossRef]
[Pubmed]
6.
Powell-Chandler A, Boyce K, James O, Scourfield L, Torkington J, Bisson J, et al. Psychological sequelae of colonic resections. Colorectal Dis 2020;22(8):945–51. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
Artificial intelligence (AI) used in the article: OpenAI’s GPT-5 was used to assist with language refinement during manuscript preparation. The tool was used to improve grammar, sentence structure, and flow in the abstract, discussion, and conclusion sections. The remaining sections were developed entirely by the authors.
Author ContributionsMaral Darya - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Simran Budhwani - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Valentina Grekos - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Karla Ortiz-Gonzalez - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Maral Darya et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}