 |
Case Report
Ovarian torsion leading to necrosis: A case report
1 M.B.B.S., Senior House Officer, Department of Obstetrics and Gynecology, Queen Elizabeth Hospital, Bridgetown, St Michael, Barbados
Address correspondence to:
Keturah Murray
Queen Elizabeth Hospital, Martindales Road, Bridgetown, St Michael,
Barbados
Message to Corresponding Author
Article ID: 100222Z08KM2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Murray K. Ovarian torsion leading to necrosis: A case report. J Case Rep Images Obstet Gynecol 2026;12(1):5–8.ABSTRACT
The pathogenesis of ovarian torsion (OT) involves a physical twisting of the ovary on an attachment point that causes lymphatic, venous, and arterial obstruction progressing to ovarian thrombosis, edema, necrosis, and infarction. Ovarian torsion typically involves an ovary with a cyst or tumor, however, this phenomenon can occur in their absence. Ultrasound is the imaging modality of choice for the evaluation and diagnosis of ovarian torsion. Typical features include a unilateral enlarged ovary, uniform peripheral cystic structures, a coexistent mass within the affected ovary, free pelvic fluid, lack of arterial or venous flow, and a twisted vascular pedicle. Management is surgical; however, the specific approach depends on several factors, including the patient’s age, fertility desires, and the presence of underlying ovarian pathology. De-torsion and oophoropexy, rather than oophorectomy, are surgical techniques that are increasing in popularity.
Keywords: Adnexa, Necrosis, Ovary, Torsion
Introduction
Ovarian torsion is commonly seen in reproductive age females. It occurs when there is partial or complete rotation of the ovarian vascular pedicle and causes obstruction to venous outflow and arterial inflow [1],[2],[3]. Timely diagnosis and prompt intervention are critical to prevent necrosis and preserve the ovary [4]. This article discusses a patient who presented with acute pelvic pain. She was diagnosed and surgically managed for right adnexal torsion. The article discusses this case in detail, the risk factors, diagnosis, and surgical management options for adnexal torsion.
Case Report
A 49-year-old P2+3 female presented to a general practitioner with a one-day history of severe, stabbing right lower quadrant pain. She reported similar episodes over the past year, with a severity of six out of ten, which were usually relieved with acetaminophen. On the day of presentation; however, the pain was now reported to be more intense (rated 12 out of 10 in severity), and persistent despite analgesia. She additionally reported decreased appetite and three episodes of vomiting. Her symptoms were not suggestive of infectious etiology, and were not associated with urinary complaints, vaginal discharge, or bleeding. She had a known history of vasculitis with surgical history significant for appendectomy and umbilical hernia repair. Her urinary pregnancy test was negative.
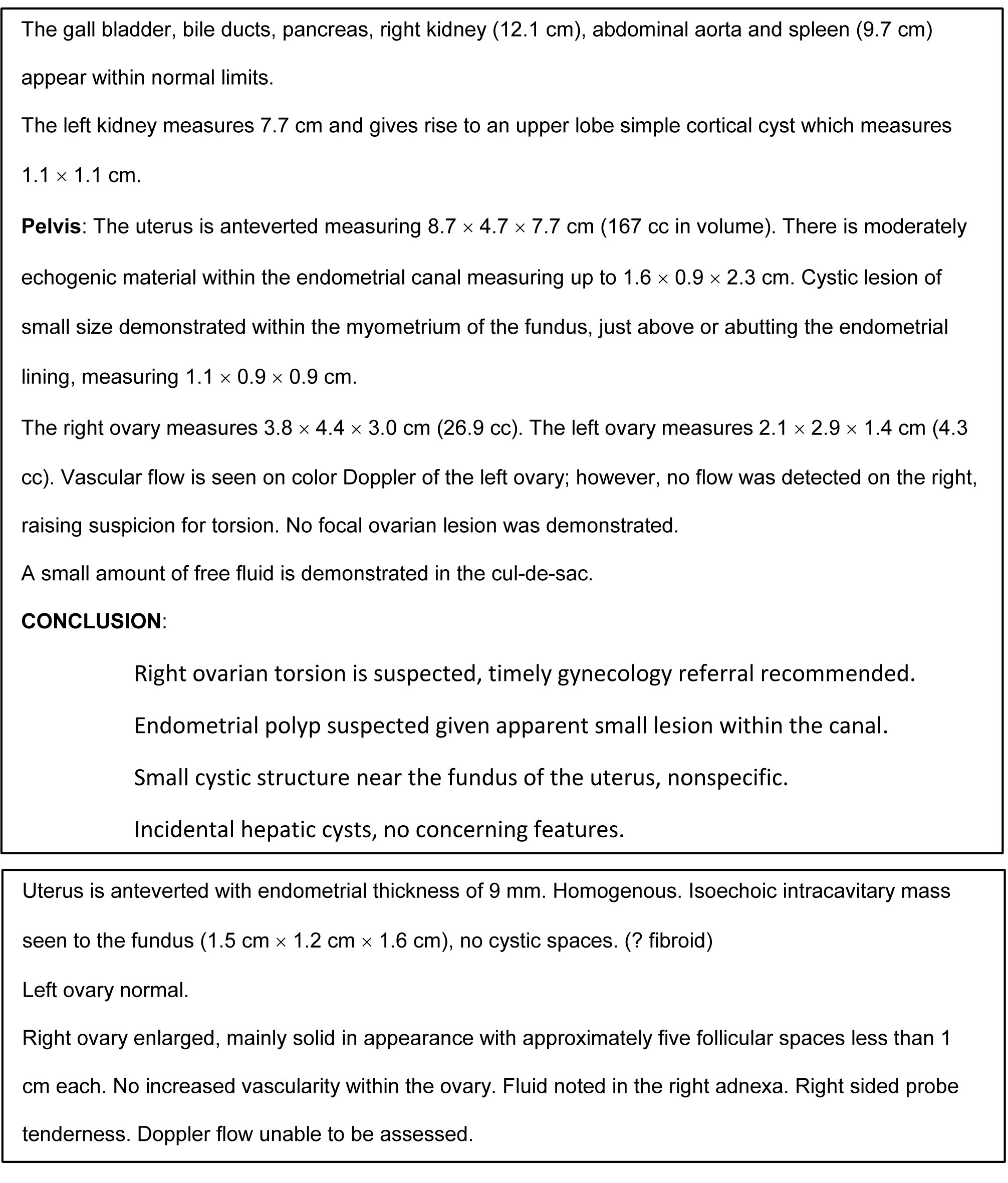
An ultrasound of the abdomen and pelvis showed features suggestive of ovarian torsion (enlarged right ovary with absence of color flow Doppler; small amount of free fluid in the cul-de-sac) (Box 1). She was subsequently referred to the Queen Elizabeth Hospital (QEH), a tertiary level center, for further management.
She appeared to be in mild painful distress. Her vitals were normal; blood pressure of 124/78 mmHg, pulse of 80 beats per minute, temperature of 36.3 °C. Inspection of the abdomen revealed surgical scars consistent with her prior operative history. On palpation, there was generalized tenderness, maximum in the right lower quadrant. There was voluntary guarding but no rebound tenderness. Her bowel sounds were present and normal. A smooth, non-tender mass was palpable in the right lower quadrant. Her cardiovascular and respiratory examinations were normal.
On genital examination, the vulva and vagina were normal, and the cervix was normal in appearance. There was no discharge or odor. Bimanual examination revealed an anteverted uterus with right adnexal tenderness, there were no adnexal masses or cervical motion tenderness.
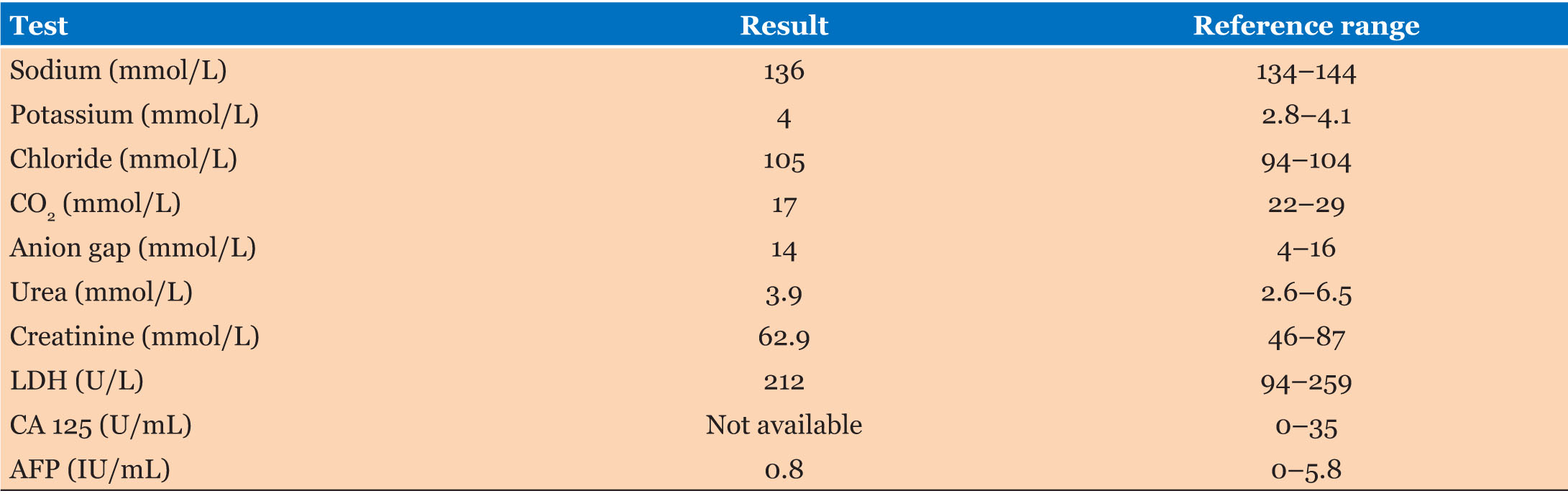
Results of her laboratory investigations (Table 1 and Table 2) were significant for a normochromic normocytic anemia. Her lactate dehydrogenase (LDH) and alpha-fetoprotein (AFP) levels were normal; however, cancer antigen 125 (CA-125) testing was not available. Given her history, examination and ultrasound findings, a diagnosis of right ovarian torsion secondary to enlarged right ovary was made. She was admitted to the gynecology ward, consent was given for surgery.
A right salpingo-oophorectomy was performed under general anesthesia. A Pfannenstiel incision was made to enter the abdomen. The uterus was enlarged to approximately 10 weeks gestation. The right ovary was twisted and hemorrhagic in appearance. It was enlarged to approximately 4 cm. The right ovary and fallopian tube were twisted one revolution (Figure 1). The left ovary and fallopian tube were normal.
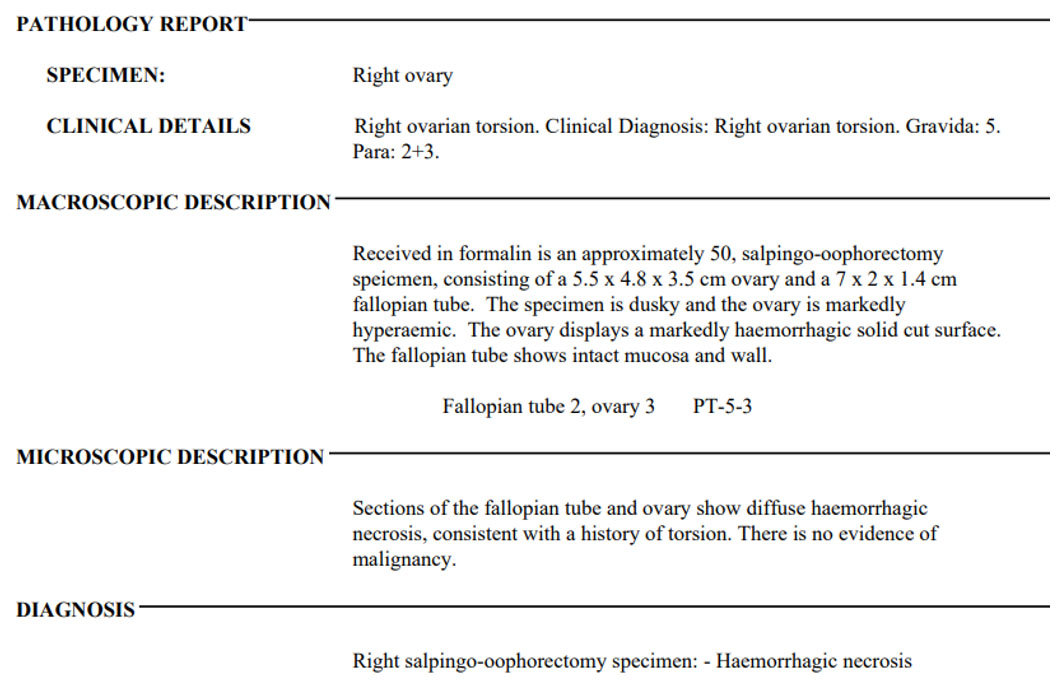
Her postoperative course was complicated by acute urinary retention on day three, which was managed with urinary catheterization. The catheter was removed following a successful trial of void prior to discharge. Her histopathology report (Box 2) showed hemorrhagic necrosis of the right ovary and fallopian tube. Follow-up was arranged with her primary care physician in her home country, as she was visiting the island at the time of admission.


Discussion
Ovarian torsion represents roughly 3% of gynecologic emergencies [1]. This phenomenon results from partial or complete rotation of the ovarian pedicle on its long axis, potentially compromising venous and lymphatic drainage [5].
Torsion occurs more commonly in young women, with the greatest incidence in the 20- to 30-year age group [5], therefore it was unusual for this diagnosis to be made in a 49-year-old female. The exact mechanism of torsion varies according to its cause. Risk factors include adnexal masses, pregnancy, ovulation induction, and previous pelvic surgery [5].
Her clinical presentation, however, was typical of that seen in ovarian torsion; acute-onset pelvic pain, often severe and unilateral, and accompanied by nausea and vomiting in up to 85% of women with ovarian torsion [4]. Her antecedent history of similar episodes over the past year was likely attributable to intermittent ovarian torsion. In scenarios where the rotation is partial or intermittent, the venous and lymphatic congestion may subside quickly, along with symptoms [5]. At presentation, patients may exhibit pyrexia and tachycardia. Abdominal examination findings may include generalized abdominal tenderness, localized guarding or rebound, while vaginal examination may reveal cervical excitation, adnexal tenderness, or an adnexal mass [3].
Her diagnosis was confirmed on ultrasound (US); there was a significant finding of an enlarged right ovary with absence of vascular flow. US imaging is a crucial diagnostic tool in suspected cases of ovarian torsion [6]. Other characteristic features include; uniform peripheral cystic structures, a coexistent mass within the affected ovary, free pelvic fluid and a twisted vascular pedicle [2]. Abnormal Doppler signals in the ovarian vessels have been identified in up to 100% of cases of adnexal torsion; however, a complete absence of perfusion may be a relatively late event, so the presence of flow within the ovary does not exclude the diagnosis of torsion [3].
Computed tomography (CT) and magnetic resonance imaging (MRI) have been shown to be useful. These modalities are expensive, however, are less readily available than ultrasound and rarely provide additional diagnostic information [3].
The surgical management of adnexal torsion is clearly determined by many factors in addition to the macroscopic appearance of the adnexa; including age, menopausal status, presence of pre-existing ovarian pathology and desire to preserve fertility [3]. Ideally, this patient would have been offered laparoscopic surgery; however, this option was not available at our institution at the time of her admission. This approach has been shown to reduce admission time, postoperative pain and long-term risk of adhesion formation [3].
Intraoperatively, involvement of both the right ovary and fallopian tube were identified therefore a right salpingo-oophorectomy was performed. Adnexal torsion is more common on the right side. This is likely due to the presence of the sigmoid colon which leaves limited space for left adnexal mobility [5]. Because of the anatomy of the broad ligament, both the ovary (or adnexal mass) and the fallopian tube are usually involved in the torsion; it is uncommon for these structures to be involved in isolation [5].
Although the traditional surgical approach has been oophorectomy or salpingo-oophorectomy, there is evidence to support conservative management with laparoscopic detorsion in most cases, with minimal short- and long-term morbidity [3]. The likelihood of preserving viable ovarian tissue is significantly decreased if the duration of torsion lasts 48 hours or longer [7]. This underscores the need for prompt intervention once the diagnosis is suspected. The patient’s age ultimately guides the definitive surgical approach; de-torsion is the treatment of choice in prepubescent girls and women of reproductive age whose families are not complete, whereas in older and postmenopausal women, oophorectomy is the treatment of choice to completely remove the risk of re-torsion [3].
Recurrent ovarian torsion is rare. It is seen more commonly in those with torsion and an adnexa without an ovarian mass, rates up to 63% [4]. In patients who undergo de-torsion, oophoropexy is a commonly used surgical technique to manage and prevent recurrent ovarian torsion however the benefits of oophoropexy to prevent further torsion versus theoretical risks lack in evidence [4].
Conclusion
Ovarian torsion is an uncommon yet serious gynecological emergency that should be considered in the differential diagnosis of any woman presenting with acute abdominal pain. A high index of suspicion is essential, as timely surgical intervention is critical to optimal management.
REFERENCES
1.
Duan Y, Hoer B, Little A. Twisting ovaries: Three cases of ovarian torsion. Cureus 2022;14(10):e30496. [CrossRef]
[Pubmed]

2.
Chang HC, Bhatt S, Dogra VS. Pearls and pitfalls in diagnosis of ovarian torsion. Radiographics 2008;28(5):1355–68. [CrossRef]
[Pubmed]
3.
Damigos E, Johns J, Ross J. An update on the diagnosis and management of ovarian torsion. The Obstetrician & Gynaecologist 2012;14(4):229–36. [CrossRef]
4.
Ellison L, Sinclair K, Sana Y. Recurrent ovarian and fallopian tube torsion: A case report. Case Rep Womens Health 2023;41:e00575. [CrossRef]
[Pubmed]
5.
Martin C, Magee K. Ovarian torsion in a 20-year-old patient. CJEM 2006;8(2):126–9. [CrossRef]
[Pubmed]
6.
Kumari A, Mishra GV, Parihar P, Dudhe SS, Bhangale PN, Agrawal R, et al. Ovarian torsion leading to necrosis: A case report of acute abdominal pain in a 25-year-old female. Cureus 2024;16(8):e67507. [CrossRef]
[Pubmed]
7.
Chen M, Chen CD, Yang YS. Torsion of the previously normal uterine adnexa. Evaluation of the correlation between the pathological changes and the clinical characteristics. Acta Obstet Gynecol Scand 2001;80(1):58–61. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Keturah Murray - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthor declares no conflict of interest.
Copyright© 2026 Keturah Murray. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}