 |
Case Report
Successful penicillin desensitization in a pregnant woman with latent syphilis and penicillin allergy
1 MBBS, Senior House Officer, Department of Obstetrics and Gynecology, Queen Elizabeth Hospital, St Michael, Barbados
Address correspondence to:
Keturah Murray
Queen Elizabeth Hospital, Martindales Road, St Michael,
Barbados
Message to Corresponding Author
Article ID: 100224Z08KM2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Murray K. Successful penicillin desensitization in a pregnant woman with latent syphilis and penicillin allergy. J Case Rep Images Obstet Gynecol 2026;12(1):14–17.ABSTRACT
Syphilis during pregnancy has a high risk of congenital transmission with disastrous fetal consequences. The only proven effective therapy for gestational syphilis is benzathine penicillin, as its bioavailability ensures adequate treatment for both the mother and the fetus. Here we report a case of a 30-year-old pregnant woman, with syphilis and a penicillin allergy, who was safely and successfully desensitized using a 4-hour oral protocol in the intensive care unit and subsequently received benzathine penicillin G.
Keywords: Penicillin desensitization, Pregnancy, Syphilis
Introduction
Syphilis is a bacterial infection caused by one of the four species within the Treponema genus, which belongs to the Treponemataceae family. It can be transmitted either through sexual contact or vertically across the placenta [1]. Syphilis during pregnancy has a high risk of congenital transmission, especially during early stages of infection. Rates of 70% to 100% in untreated pregnant people with primary or secondary syphilis have been reported [2]. Consequences include abortion, premature delivery, intrauterine growth retardation, perinatal death and congenital syphilis (CS) [3]. The only proven effective therapy for gestational syphilis is benzathine penicillin. Treatment should begin immediately after a positive syphilis diagnosis in pregnant women, unless the patient has recently received appropriate treatment [4]. Due to lack of effective alternatives, treatment of penicillin allergic patients provides a unique challenge in their care.
Case Report
A 30-year-old G2P1, who presented for her antenatal booking visit at 10 weeks gestation, was found to have latent syphilis [rapid plasma reagin (RPR) positive]. Of note she had a history of untreated, late diagnosed (36 weeks gestation) latent syphilis in her last pregnancy. That pregnancy resulted in a neonate with CS, who, fortunately, did not develop any long-term complications. The patient reported an extensive allergy history to drugs including metimazole (baralgin), hyoscine butylbromide (buscopan), non-steroidal anti-inflammatory drugs and penicillin. The allergic reaction was reported to be characterized by pruritus, hives, and periorbital edema. Unfortunately, at the time of presentation confirmatory penicillin allergy testing was not available.
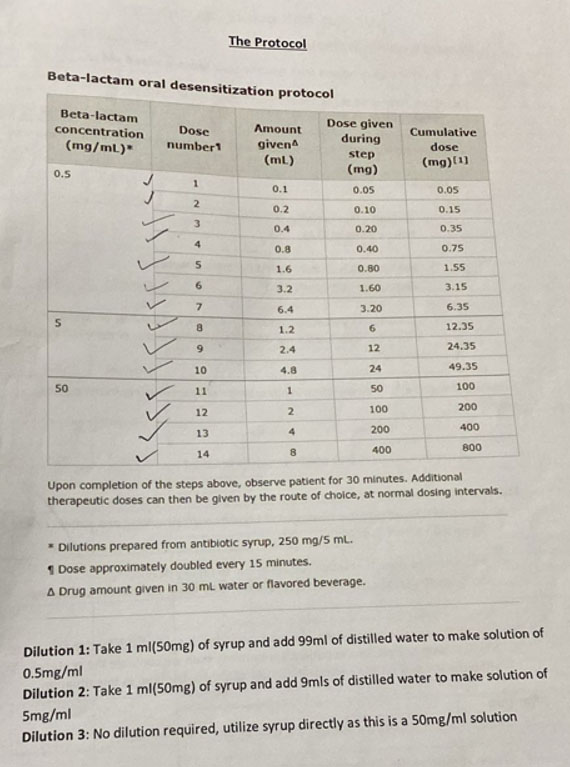
Given the outcome of the prior pregnancy and persistence of infection in this current pregnancy (RPR titer increase 8-fold between 10 and 20 weeks gestation), the decision was made to admit her to hospital for penicillin desensitization treatment. She was admitted at 25 weeks gestation and underwent the protocol (Figure 1) with no issues, she remained asymptomatic and hemodynamically stable. The protocol was finalized in 4 hours and the first dose of benzathine penicillin G was administered intramuscularly (2.4 million units). She was discharged after 48 hours monitoring on the intensive care unit. She subsequently received two further doses of benzathine penicillin G as an outpatient without complications. Monitoring of her pregnancy included serial growth scans from 28 weeks gestation. Her pregnancy was uncomplicated, and she had a spontaneous vaginal delivery of a live female neonate at 39 weeks 4 days gestation.
Discussion
Syphilis during pregnancy remains a major public health concern and is the second leading cause of stillbirth worldwide [4]. In this pregnancy, the diagnosis of syphilis was identified in the first trimester. All women should be screened for syphilis early in pregnancy. Women at high risk for infection should be screened again at 28 weeks of gestation and at delivery [5]. The objectives of the screening program are to: reduce the risk of vertical transmission of syphilis, ensure that syphilis is identified early in pregnancy, and to facilitate appropriate and timely neonatal referral and management [6]. Intrauterine exposure to Treponema pallidum can result in severe consequences, with adverse pregnancy outcomes in more than 50% of cases, including miscarriage, stillbirth, neonatal death, and both early and late complications in live-born infants [4].
In her first pregnancy, the neonate developed CS. According to World Health Organization estimates, in 2022 there were 8 million new syphilis cases among adults and the global CS case rate was 523 per 100,000 live births [7]. The only effective treatment for gestational syphilis is administration of benzathine penicillin, which is bioavailable to the fetus and thus ensures treatment of both mother and child. Syphilis treatment must be started immediately after a positive test, regardless of the type of test or the titer detected [8]. Current guidelines recommend penicillin G benzathine, 7.2 million units total, administered in three intramuscular doses of 2.4 million units each at 1-week intervals.
This patient had an extensive allergy history. Although there is a critical need for alternatives to parenteral penicillin regimens during pregnancy, data supporting the use of alternative regimens are insufficient at this time [5]. In two separate reports, Plotzker et al. described the use of azithromycin and ceftriaxone among penicillin-allergic pregnant patients. Regarding ceftriaxone, daily injections of 250 mg for 14 days were effective in preventing CS among 11 neonates. No treatment failures were seen. Plotzker et al.’s second report described azithromycin treatment failures in 5 pregnancies. In light of concerns about efficacy and azithromycin-resistant T. pallidum, azithromycin is not recommended for treatment of syphilis in pregnancy [9].
Penicillin allergy remains the most common drug allergy reported, with a prevalence of ~8–12% [10]. Reactions can manifest as a wide range of clinical conditions, from mild rash, urticaria, or angioedema to full-blown anaphylaxis. Two methods used to investigate penicillin allergy include in vivo and in vitro testing. In vivo testing involves direct testing on the patient, such as skin prick or intradermal tests, to observe a clinical response, whereas in vitro testing uses laboratory assays on blood samples (e.g., penicillin-specific IgE) without exposing the patient to the allergen. The combination of a clinical history consistent with an immediate hypersensitivity reaction and positive in vivo or in vitro test results is diagnostic of penicillin allergy, and the patient must be referred for desensitization. If the clinical history is inconsistent with immediate hypersensitivity reaction and both in vivo and in vitro tests are negative, a drug provocation test can be carried out to confirm or rule out the diagnosis of penicillin allergy [8].
In a study by Sullivan et al., they were able to prove oral desensitization as an effective, relatively safe approach by administering beta-lactam antibiotics to penicillin-allergic patients with life-threatening infections. Thirty consecutive patients with histories of allergic reactions to penicillin, positive immediate wheal and flare skin-test reactions to penicillin determinants, and life-threatening infections were studied. Skin-test reactions disappeared or diminished in all 23 subjects who were retested titre desensitization. Full courses of antibiotic therapy and cure of the infections were accomplished in 30 of 30 patients. No deaths, anaphylaxis, or severe acute allergic reactions occurred [11].
Serologic cure refers to a decline by a factor of 4 or more in nontreponemal titers 6 to 12 months after therapy for early syphilis and twelve to 24 months after therapy for late syphilis [5]. Therefore, these patients should be followed up and monitored after delivery.
Conclusion
Syphilis is a highly contagious sexually transmitted infection with a potential for significant detrimental impact on the fetus. Early recognition and treatment are essential for the management of this disease. A caveat in treatment is the lack of alternative appropriate antibiotic choice in penicillin allergic patients. This case highlights the option of successful penicillin desensitization and treatment for these patients.
REFERENCES
1.
Nisa AS, Bayuaji H, Winarno GNA. Too late to treat: Missed antenatal syphilis screening and a fatal neonatal outcome – A case report. Int Med Case Rep J 2025;18:1111–6. [CrossRef]
[Pubmed]

2.
Syphilis guide: Risk factors and clinical manifestations. 2021. [Available at: https://www.canada.ca/en/public-health/services/infectious-diseases/sexual-health-sexually-transmitted-infections/canadian-guidelines/syphilis/risk-factors-clinical-manifestation.html]
3.
Fica A, Muñoz D, Rojas T, Sanzana C, Muñoz C. Penicillin desensitization in allergic pregnant women with syphilis. Report of two cases. Rev Med Chil 2020;148(3):344–8. [CrossRef]
[Pubmed]
4.
Gehlen B, Feodrippe A, Garcia JFB, Aun MV, Kalil J, Giavina-Bianchi P. Effectiveness and safety of algorithm for treating pregnant women with syphilis and history of immediate allergy to penicillin. J Allergy Clin Immunol Glob 2025;4(4):100572. [CrossRef]
[Pubmed]
5.
Ghanem KG, Ram S, Rice PA. The modern epidemic of syphilis. N Engl J Med 2020;382(9):845–4. [CrossRef]
[Pubmed]
6.
Kingston M, Wilson J, Dermont S, Fifer H, Chan K, Lyall H, et al. British Association of Sexual Health and HIV (BASHH) UK guidelines for the management of syphilis in pregnancy and children 2024. Int J STD AIDS 2024;35(14):1161–73. [CrossRef]
[Pubmed]
7.
Congenital syphilis [Internet]. datadot. [cited 2025 Nov 23]. [Available at: https://data.who.int/dashboards/sti/congenital-syphilis]
8.
Gehlen B, Feodrippe A, Garcia JFB, Aun MV, Kalil J, Giavina-Bianchi P. Effectiveness and safety of algorithm for treating pregnant women with syphilis and history of immediate allergy to penicillin. J Allergy Clin Immunol Glob 2025;4(4):100572. [CrossRef]
[Pubmed]
9.
Plotzker RE, Murphy RD, Stoltey JE. Congenital syphilis prevention: Strategies, evidence, and future directions. Sex Transm Dis 2018;45(9S Suppl 1):S29–37. [CrossRef]
[Pubmed]
10.
Albin S, Agarwal S. Prevalence and characteristics of reported penicillin allergy in an urban outpatient adult population. Allergy Asthma Proc 2014;35(6):489–94. [CrossRef]
[Pubmed]
11.
Sullivan TJ, Yecies LD, Shatz GS, Parker CW, Wedner HJ. Desensitization of patients allergic to penicillin using orally administered beta-lactam antibiotics. J Allergy Clin Immunol 1982;69(3):275–82. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Keturah Murray - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Keturah Murray. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}