 |
Case Report
Liveborn case of limb-body wall complex with identification of the extraembryonic coelomic cavity on third trimester ultrasound
1 Department of Gynecology and Obstetrics, The Johns Hopkins Hospital, Baltimore, MD, United States
2 Department of Pathology, The Johns Hopkins Hospital, Baltimore, MD, United States
Address correspondence to:
Yanling Dong
MD, 600 N. Wolfe Street, Phipps 214, Baltimore, MD 21287,
United States
Message to Corresponding Author
Article ID: 100227Z08YD2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Dong Y, Guthrie T, Nauen D, Blakemore K. Liveborn case of limb-body wall complex with identification of the extraembryonic coelomic cavity on third trimester ultrasound. J Case Rep Images Obstet Gynecol 2026;12(1):27–31.ABSTRACT
Introduction: Limb-body wall complex (LBWC), also known as body stalk anomaly, is a rare and lethal congenital condition affecting multiple organ systems, including the abdominal and thoracic walls, limbs, craniofacial structures, and spine. It is characterized by visceral attachment to the placenta with a short or absent umbilical cord, along with spinal deformities. The exact pathogenesis of LBWC remains unknown, though several theories have been proposed, including early amnion rupture, primary ectodermal failure of the embryonic disc, and impaired embryonic blood flow. The herniation of abdominal contents into the extraembryonic coelomic cavity, the space between the chorion and the amnion, rather than the amniotic cavity, helps differentiate LBWC from complex omphalocele.
Case Report: We present the ultrasound findings of LBWC in a patient at 32 weeks and 5 days who presented with preterm contractions and suspected rupture of membranes. Despite it being unusual to observe the space between the amnion and chorion at this gestational age, prenatal ultrasound clearly revealed significant herniation of intra-abdominal organs into the extraembryonic coelomic cavity. The patient subsequently underwent a liveborn vaginal delivery the following day.
Conclusion: Recognition of herniation of abdominal contents into the extraembryonic coelomic cavity can help differentiate LBWC from other anterior abdominal wall defects, even in late gestation. Accurate diagnosis of LBWC in the third trimester can facilitate appropriate patient counseling and perinatal care planning.
Keywords: Body stalk anomaly, Extraembryonic coelomic cavity, Limb-body wall complex, Prenatal ultrasound
Introduction
Limb-body wall complex (LBWC) is a rare, severe, and typically lethal multi-organ fetal malformation characterized by major abdominal wall defects with visceral herniation, limb and spine abnormalities, and craniofacial defects [1],[2]. Prenatal diagnosis is made by ultrasonography, most often in the first or second trimester. Recognition of key findings, especially herniation of abdominal contents into the extraembryonic coelomic cavity (between the chorion and the amnion), can help differentiate LBWC from other anterior abdominal wall defects [3]. Diagnosis in the third trimester is challenging due to difficulty visualizing the extraembryonic coelomic cavity, and may complicate patient counseling given the poor prognosis. We report a case of LBWC diagnosed on third-trimester ultrasound at 32 weeks with clear visualization of visceral herniation into the extraembryonic coelomic cavity, followed by liveborn delivery.
Case Report
A 35-year-old G2P1001 woman who received care at an outside institution presented to Labor and Delivery at 32 weeks and 5 days with suspected preterm rupture of membranes and uterine contractions. She reported that her pregnancy was complicated by significant fetal anomalies but was unsure of the specific diagnosis. The patient related that pregnancy termination had been recommended earlier in gestation, though she was unable to reach a decision at that time. Per chart review, cell-free DNA screening at 14 weeks was low risk for common aneuploidies. Maternal serum alpha-fetoprotein at 18 weeks was markedly elevated at 445.4 ng/mL (8.3 multiples of the median).
Ultrasound Findings
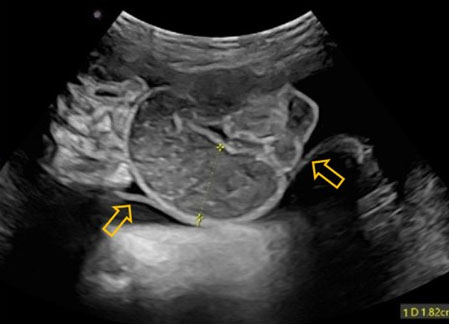
A detailed ultrasound upon the patient's arrival at our center revealed a large abdominal wall defect with evisceration of multiple intra-abdominal organs—including the liver, stomach, bowel, bladder, and a kidney—into the extraembryonic coelomic cavity (Figure 1 and Figure 2). The bowel appeared dilated and non-peristaltic (Figure 3), raising concern for volvulus or atresia. Polyhydramnios was present, with an amniotic fluid index (AFI) of 30 within the amniotic cavity. Additional findings included moderate bilateral cerebral ventriculomegaly, agenesis of the cavum septum pellucidum with disruption of the midline falx, an abnormal head shape with biparietal bulging and frontal bossing, a bifid glans penis with possible hypospadias, scoliosis, and kyphosis involving the sacral and lower lumbar spine, splaying of the sacral vertebrae consistent with spina bifida, shortened long bones, and bilateral clubfeet. The umbilical cord was short and demonstrated a single umbilical artery. The constellation of anomalies, particularly the identification of herniated intra-abdominal organs within the extraembryonic coelomic cavity, differentiated this case from a non-isolated omphalocele and established a prenatal diagnosis of limb-body wall complex.
Initial evaluation for ruptured membranes was positive for pooling, nitrazine, and ferning; however, subsequent exams were negative for all of these findings. A palpable amniotic sac was noted through a cervix dilated to 2 cm. It was suspected that the “sticky” fluid initially observed originated from the extraembryonic coelomic cavity. The patient was extensively counseled about the poor prognosis associated with LBWC, including the option of comfort care for the neonate postnatally. After thorough discussion, she elected to proceed with labor augmentation. She received oxytocin followed by a cervical Foley balloon, and then progressed to full dilation. She subsequently delivered a liveborn male neonate weighing 1531 g, with Apgar scores of 2 and 3 at 1 and 5 minutes, respectively. Delivery was complicated by cord avulsion and retained placenta, which required manual removal. The neonate received comfort care in accordance with the patient’s wishes and passed away at 49 minutes of life. Postnatal chromosomal microarray analysis on the neonate was normal, consistent with a male fetus.
Autopsy Findings
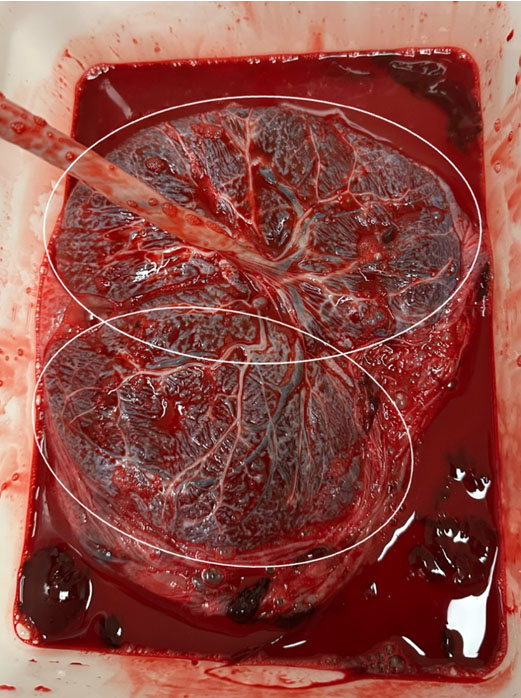
Autopsy confirmed prenatal findings, including herniation of intra-abdominal organs into the extraembryonic coelomic space (Figure 4 and Figure 5). It additionally revealed an accessory phalanx attached to the great toe, syndactyly of toes 3–6 on the right foot, abnormally edematous male external genitalia with an adjacent appendage anterior to the base of the penis, and an absent anal opening. A sacral dimple was noted without apparent evidence of an open neural tube defect.




Discussion
Limb-body wall complex is a rare, severe congenital anomaly involving multiple organ systems, traditionally characterized by the presence of at least two of the three Van Allen criteria: (1) exencephaly or encephalocele with facial clefts; (2) thoraco-and/or abdominoschisis; and (3) limb defects [1]. Limb-body wall complex affects approximately 1 in 15,000 pregnancies, with most cases resulting in intrauterine demise or elective termination. In rare cases where neonates survive delivery [4], they typically die shortly after birth, as occurred in our case.
Associations have been reported between LBWC and placental or fetal aneuploidy [5],[6], mutations in genes related to laterality and caudal development—such as HOX, bFGF, WNT1-8, and SHH [7]—and maternal cocaine use [8]. However, the majority of cases appear to be sporadic events with no identifiable genetic or teratogenic cause [9]. Overall, the recurrence risk is considered to be very low.
Several theories have been proposed for the pathogenesis of LBWC: (1) early amniotic sac rupture leading to amniotic band formation and mechanical disruption of fetal development; (2) primary defects in embryonic folding and closure during early development; and (3) vascular compromise between the fourth and sixth weeks of gestation, impairing embryogenesis [10]. The first two theories have in common the loss of the normal amniotic membrane that would usually prevent the fetus and its organs from having direct contact with the chorion and the extraembryonic coelomic cavity. By the first theory, an amnion had formed but subsequently developed a site of rupture, while by the second theory, the amnion failed to form normally in the first place. In either event, fetal parts may then become attached to the chorion and remain extruded within the extraembryonic coelomic cavity. The end result is LBWC.
Early diagnosis of LBWC is important, as the prognosis is extremely poor and generally considered lethal as there is no curative surgical intervention [10]. High-resolution prenatal ultrasound can consistently detect LBWC as early as 11 weeks’ gestation [11]. Indeed, first trimester screening sonography, which has now become routine in many centers worldwide, should enhance the detection of LBWC. This is because careful imaging can often determine if the location of fetal abdominal contents is in the extraembryonic coelom and not intra-amniotic, as the extraembryonic coelomic cavity is still readily identifiable with separation of the amnion and chorion in the first trimester. Later in gestation, discerning this extraembryonic coelomic space becomes more difficult. Yet, the location of organs in the extraembryonic coelomic cavity is a critical differentiating feature of LBWC as opposed to a complex omphalocele. This case is unusual for demonstrating this feature sonographically at such a late gestational age, allowing timely and frank intrapartum counseling. A firm diagnosis of LBWC enables appropriate counseling to help the family process prognosis-related challenges and support decision-making, typically including the option of pregnancy termination. For a pregnancy progressing to delivery of a liveborn infant, options such as palliative care and comfort measures can be discussed prenatally for optimal parental preparedness and decision-making in the postnatal period.
Conclusion
Limb-body wall complex is a rare and typically lethal congenital anomaly that can be diagnosed prenatally by ultrasound. This case demonstrates that herniation of abdominal contents into the extraembryonic coelomic cavity may remain identifiable even in the third trimester. Recognition of this finding can aid in differentiating LBWC from other anterior abdominal wall defects and supports appropriate prenatal counseling and management.
REFERENCES
1.
Van Allen MI, Curry C, Gallagher L. Limb body wall complex: I. Pathogenesis. Am J Med Genet 1987;28(3):529–48. [CrossRef]
[Pubmed]

2.
Chikkannaiah P, Dhumale H, Kangle R, Shekar R. Limb body wall complex: A rare anomaly. J Lab Physicians 2013;5(1):65–7. [CrossRef]
[Pubmed]
3.
Zhang L, Wang R, Zhao Y, Wu J, Li H, Li M. Characteristic analysis of ultrasound diagnosis of limb body wall complex in early pregnancy. Prenat Diagn 2025;45(8):1004–12. [CrossRef]
[Pubmed]
4.
Nagase H, Ohyama M, Yamamoto M, Akamatsu C, Miyake Y, Nagashima A, et al. Prenatal ultrasonographic findings and fetal/neonatal outcomes of body stalk anomaly. Congenit Anom (Kyoto) 2021;61(4):118–26. [CrossRef]
[Pubmed]
5.
Chan Y, Silverman N, Jackson L, Wapner R, Wallerstein R. Maternal uniparental disomy of chromosome 16 and body stalk anomaly. Am J Med Genet 2000;94(4):284–6. [CrossRef]
[Pubmed]
6.
Doray B, Viville B, Touret Y, Gasser B, Samama B, Boehm N, et al. Mosaic trisomy 13 on chorionic villi in a fetus with body wall complex: Fortuitous association or pathogenic hypothesis? Prenat Diagn 2003;23(12):1021–3. [CrossRef]
[Pubmed]
7.
Gajzer DC, Hirzel AC, Saigal G, Rojas CP, Rodriguez MM. Possible genetic origin of limb-body wall complex. Fetal Pediatr Pathol 2015;34(4):257–70. [CrossRef]
[Pubmed]
8.
Viscarello RR, Ferguson DD, Nores J, Hobbins JC. Limb-body wall complex associated with cocaine abuse: Further evidence of cocaine’s teratogenicity. Obstet Gynecol 1992;80(3 Pt 2):523–6.
[Pubmed]
9.
Sahinoglu Z, Uludogan M, Arik H, Aydin A, Kucukbas M, Bilgic R, et al. Prenatal ultrasonographical features of limb body wall complex: A review of etiopathogenesis and a new classification. Fetal Pediatr Pathol 2007;26(3):135–51. [CrossRef]
[Pubmed]
10.
Farhat IB, Toumi D, Maatoug M, Gharbi N, Aribi I, Guerbej E, et al. Limb body wall complex: From diagnosis to prognosis (a case report). PAMJ Clin Med 2024;16(14).
11.
Ye CH, Li S, Ling L. Analysis of characteristic features in ultrasound diagnosis of fetal limb body wall complex during 11-13+6 weeks. World J Clin Cases 2023;11(19):4544–52. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
The authors wrote the original manuscript. ChatGPT (OpenAI, GPT-4 model) was used solely to assist with language editing and improvement of grammar and clarity in portions of the manuscript. No data, results, analyses, or scientific content were generated by artificial intelligence. The authors take full responsibility for the content of this article.
Author ContributionsYanling Dong - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Tracee Guthrie - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
David Nauen - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Karin Blakemore - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Yanling Dong et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}