 |
Case Report
Postpartum foot drop after vaginal delivery: A case of urgent spinal nerve decompression and literature review
1 Resident Physician, Department of Obstetrics and Gynecology, Loyola University Medical Center, Maywood, IL, USA
2 Medical Student, Stritch School of Medicine, Maywood, IL, USA
3 Assistant Professor, Department of Obstetrics and Gynecology, Loyola University Medical Center, Maywood, IL, USA
Address correspondence to:
Jennifer Law
1133 South Blvd, Oak Park, IL 60302,
USA
Message to Corresponding Author
Article ID: 100228Z08JL2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Law J, Zilber A, Cox-Pedota M. Postpartum foot drop after vaginal delivery: A case of urgent spinal nerve decompression and literature review. J Case Rep Images Obstet Gynecol 2026;12(1):32–37.ABSTRACT
Introduction: Postpartum neuropathies have long been recognized as potential complications of childbirth. Commonly affected nerves include femoral, sciatic, lumbosacral plexus, lateral femoral cutaneous, and peroneal nerves. Risk factors include prolonged second stage of labor, maternal short stature, fetal macrosomia, instrumental deliveries, hyperflexed positioning, and neuraxial anesthesia. Most reported cases are managed conservatively and ultimately resolve within weeks or months after delivery.
Case Report: We describe a case of new-onset foot drop following an uncomplicated spontaneous vaginal delivery. To our knowledge, very few cases of postpartum foot drop secondary to lumbar disc herniation requiring surgical decompression have been reported.
Conclusion: Although most postpartum lower extremity neuropathies resolve with time and conservative therapy, clinicians should maintain a high index of suspicion for structural causes when symptoms are severe or progressive. This case underscores the importance of prompt recognition and evaluation of new neurologic symptoms, even after apparently uncomplicated deliveries, to facilitate timely intervention and optimize recovery.
Keywords: Foot drop, Herniated disc, Obstetric palsy, Peroneal neuropathy, Postpartum, Vaginal delivery
Introduction
Postpartum neuropathies represent a rare but well-recognized complication of vaginal childbirth, with obstetric nerve palsies occurring in approximately 0.3–1.8% of deliveries [1]. The most commonly affected nerves include the lateral femoral cutaneous, femoral, obturator, sciatic, lumbosacral plexus, and common peroneal nerves. Most injuries are transient, whereas more serious long-term complications are rare. Risk factors for obstetric nerve injuries include maternal (short stature, preexisting neuropathy, diabetes), fetal (macrosomia), and intrapartum factors such as prolonged second stage, hypotension, instrumental delivery, hyperflexed maternal positioning, and neuraxial anesthesia [1].
Foot drop is a common clinical presentation of obstetric-related nerve injury, typically accompanied by sensory deficits along the anterolateral leg and dorsum of foot [1]. The mechanism of injury most frequently involves compression of the common peroneal nerve at the fibular head during leg hyperflexion (peripheral nerve compression) or from tight manual grip during the second stage of labor, either by the patient or a labor attendant. Less commonly, foot drop can arise from lumbosacral plexopathy, typically involving the L5 nerve root [2]. Proposed mechanisms for nerve injury include compression of the plexus between the bony pelvis and the fetal presenting part or during instrumental vaginal delivery [2].
Another less common mechanism for central nerve injury is compression from a spinal epidural hematoma. Although this is a rare complication of neuraxial anesthesia, prompt evaluation with spinal imaging is warranted in the setting of persistent neuropathies, acute or worsening back pain, or bladder and bowel dysfunction. Gruzman et al. suggested risk factors for spinal epidural hematoma including difficult or traumatic epidural catheter placement, coagulopathy or anticoagulation therapy, and spinal deformities or tumors [3]. Fortunately, most cases of obstetric nerve injuries resolve spontaneously with conservative management, with full recovery typically noted within 6–8 weeks [2]. Surgical intervention is exceptionally rare as obstetric nerve injuries are overwhelmingly due to peripheral compressive mechanisms rather than central level pathology.
Here we report the first documented case of postpartum foot drop after uncomplicated vaginal delivery requiring urgent surgical decompression of a herniated lumbar disc. This case highlights the importance of maintaining high clinical suspicion for atypical pathology even in the setting of a seemingly routine obstetric nerve injury. We also review the recent literature on nerve injuries presenting as foot drop following vaginal birth since 2000. For the literature review, PubMed database was searched using combinations of the terms “foot drop,” “peroneal neuropathy,” “obstetric palsy,” “obstetrics,” “postpartum,” “vaginal delivery,” and “herniated disc” and filtered for case reports between 2000 and 2026. After excluding non-obstetric cases and cesarean deliveries, 12 cases were identified. Table 1 summarizes the clinical characteristics of these published cases in addition to our patient.

Case Report
We present the clinical course of a 32-year-old G1P0 who presented for elective induction of labor at 40 weeks and 1 day of gestation. Her initial cervical exam was 5 cm dilated with a Bishop score of 9, and labor was augmented with oxytocin. She requested epidural analgesia for labor. The pre-anesthesia checklist was completed, and no contraindications to neuraxial anesthesia were identified. Using standard aseptic technique, an 18-gauge Tuohy needle was inserted at the L4-L5 space to a depth of 8 cm, followed by placement of an epidural catheter to a skin depth of 16 cm. After dosing, she noted heaviness in both legs but maintained some voluntary movement.
Artificial rupture of membranes was subsequently performed with clear amniotic fluid. During maternal repositioning, the epidural catheter was inadvertently dislodged, and the anesthesia team was called back to replace it. A second epidural was placed at the L3-L4 space using an 18-gauge Tuohy needle advanced to 7 cm, with the catheter threaded to a skin depth of 12 cm. Immediately after the second epidural placement, the patient reported good pain relief and labor continued without further anesthetic complications.
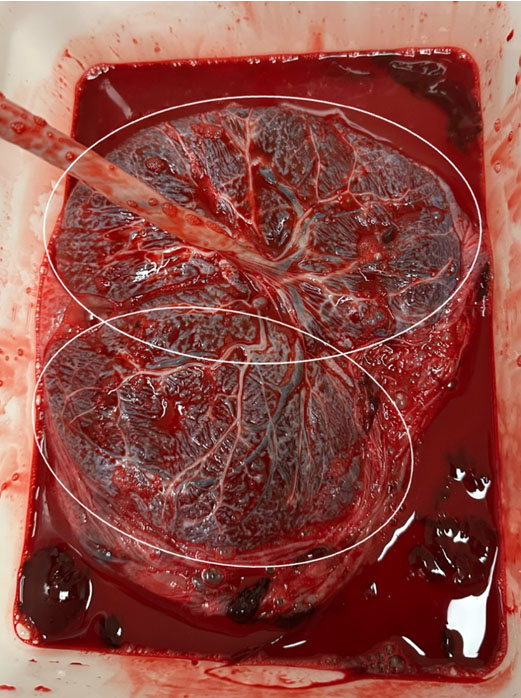
After achieving complete cervical dilation, she began pushing in the dorsal lithotomy position with stirrups. She pushed for approximately 3 hours and had a normal spontaneous vaginal delivery of a liveborn male infant weighing 3800 grams. The placenta delivered spontaneously and intact with a three-vessel cord. A second-degree perineal laceration was repaired in the usual fashion. The epidural infusion was discontinued after delivery per institutional protocol.
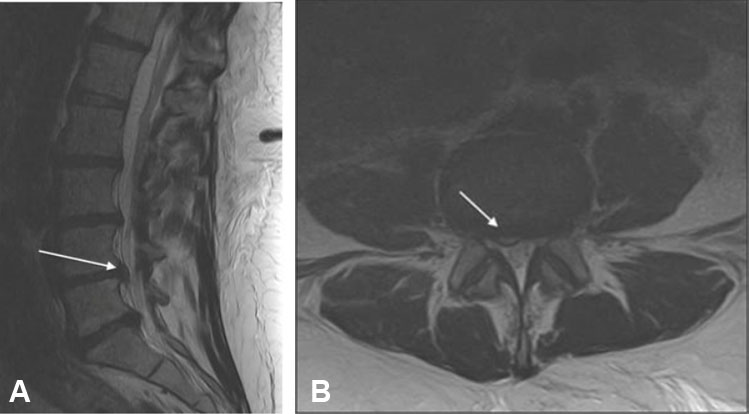
On routine postpartum exam the following morning, the patient reported new-onset right foot weakness accompanied by numbness and tingling. Neurologic examination revealed right foot drop with 0/5 strength in ankle dorsiflexion. Sensation to light touch was diminished over the right foot. Bowel and bladder function remained intact. She was evaluated by neurology and physical therapy was initiated for presumed compressive neuropathy. On postpartum day 2, symptoms persisted, and she required a walker to ambulate. Magnetic resonance imaging (MRI) of the lumbar spine demonstrated a right-sided L4-L5 disc herniation compressing the exiting L5 nerve roots (Figure 1). Neurosurgery was consulted and recommended immediate surgical decompression. The patient was transferred to a nearby tertiary center where she underwent L3-L5 laminectomy, L4-L5 right discectomy, and repair of incidental durotomy.
Postoperatively, she was hospitalized for three days. Sensory symptoms improved with physical rehabilitation, but she continued to have complete paralysis of right foot motor function at discharge and was prescribed home-based physical therapy and ankle-foot orthosis (AFO). At her one-month postoperative follow-up, she continued to experience complete loss of dorsiflexion and plantarflexion and remained AFO-dependent, though she reported improvement in sensation. With ongoing home physical therapy over the subsequent months, she slowly regained strength. By the three-month follow-up appointment with neurosurgery, she reported complete restoration of right foot strength and sensation.
Discussion
Our review of the literature found that the vast majority of obstetric-related nerve injuries involve peripheral nerves and can be managed conservatively. Patients almost always experience a full or near-full return of motor and sensory function within weeks to months postpartum.
The risk of nerve injury increases in the setting of protracted labor, instrumental delivery, lithotomy positioning, stirrup use, and neuraxial anesthesia. Epidural analgesia may mask discomfort, potentially leading to prolonged positioning, rather than being a direct cause of nerve injury [1].
Table 1 summarizes the clinical characteristics of our patient plus the 12 reported cases of foot drop or lower extremity neuropathy after vaginal delivery identified in our literature review. Across these 13 cases, the mean maternal age was 28.4 years (range 23–36 years), and most patients were primiparous (69.2%, 9/13). Labor was frequently prolonged, with total labor durations up to 31 hours and length of second stage commonly exceeding 1–2 hours in those that specified pushing time. Most deliveries were spontaneous births, with only two operative vaginal deliveries identified (one vacuum, one forceps). Neuraxial analgesia was used in 84.6% of cases (11/13), highlighting its frequent association with postpartum neuropathies.
Aside from our reported case, all identified cases were treated conservatively and/or medically with 100% having complete or nearly complete recovery [3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13]. A few had residual sensory deficits, typically involving the big toe or dorsum of foot [4],[5],[6]. The mean time to full or near-full recovery was approximately three months, with reported recovery intervals ranging from 1–7 months.
Our review of the literature found that electrodiagnostic testing was frequently used to localize the affected lesion. Electromyography (EMG) and nerve conduction studies (NCS) confirmed common peroneal neuropathy or sciatic neuropathy in most cases. Spinal magnetic resonance imaging (MRI) was often normal, reinforcing the primarily peripheral nature of these injuries. Two exceptions included one patient with an epidural hematoma spanning T12-S1, causing compression at L4-L5 and L5-S1 and one case of ischiofemoral impingement in whom MRI demonstrated narrowing of the quadratus femoris space and edema of the sciatic nerve [7],[8].
The management of obstetric nerve injuries almost always includes physical therapy. In some cases, patients were also treated with gabapentin, duloxetine, and topical analgesics. Some were provided with AFO devices for gait support. The one patient who was diagnosed with an epidural hematoma was treated with intravenous steroids and had a full recovery by one month postpartum [7].
Our patient differs from these prior reports in several important ways. Rather than a peripheral mononeuropathy, she exhibited an L5 radiculopathy due to an acute L4-L5 disc herniation identified on MRI. Clinically, she presented with complete flaccid paralysis of the foot in contrast to “weakness” or partial deficits described in prior cases. Her clinical and imaging findings necessitated urgent surgical intervention with laminectomy and discectomy, whereas all previously published postpartum foot drop cases improved with conservative management alone. To our knowledge, this represents the first reported case of postpartum foot drop after vaginal delivery attributable to an acute lumbar disc herniation requiring operative decompression.
This case has important diagnostic implications. First, it highlights the significance of obtaining imaging in a timely manner, especially when symptoms are persistent or severe. In addition, complete motor paralysis should raise suspicion for potential central or root level etiology. Persistent motor paralysis beyond 24–48 hours should prompt further evaluation. A thorough neurological examination and early spinal imaging—typically MRI of the lumbar spine—are recommended to exclude structural lesions such as disc herniation or hematoma. When imaging reveals significant nerve root or cauda equina compression, prompt neurosurgical consultation and timely intervention may optimize long-term outcomes.
From a preventative standpoint, risk mitigation strategies include minimizing the duration of extreme lithotomy positioning, avoiding prolonged pressure on the fibular head and proximal tibia, and frequent repositioning during the second stage, particularly when pushing is prolonged [5],[6],[7]. Close postpartum monitoring for new neurologic symptoms is also important, especially among patients who receive neuraxial anesthesia.
Pregnancy is not considered an independent risk factor for lumbar disc herniation; however, both biomechanical and hormonal changes may predispose vulnerable discs to herniation. Whiles et al. describe such changes, including increased lumbar lordosis, higher axial load, and ligamentous laxity mediated by elevated relaxin levels, which together may increase the risk of lumbar disc extrusion in pregnancy [14] . Repeated Valsalva maneuvers and elevated intra-abdominal pressure during prolonged second stage pushing may further increase the risk of annular rupture and disc herniation. In our patient, MRI demonstrated mild to moderate stenosis at multiple lumbar levels, so it is plausible that a pre-existing but subclinical L4-L5 disc protrusion acutely herniated during labor, resulting in L5 radiculopathy and foot drop.
Conclusion
Our case and accompanying literature review highlight that although most postpartum neuropathies after vaginal delivery involve peripheral nerves and resolve without surgery, clinicians must remain vigilant for the rare but clinically significant possibility of structural etiologies resulting in compressive central or nerve root lesions. Prompt recognition of atypical features, timely imaging, and early neurosurgical involvement may optimize long-term outcomes. Increased awareness of this rare entity may facilitate earlier diagnosis and intervention, ultimately improving maternal neurologic recovery.
REFERENCES
1.
Rider Sleutel M, True B, Webb J, Valdez E, Van Thi Tran M. Integrative review of lower extremity nerve injury during vaginal birth. J Obstet Gynecol Neonatal Nurs 2020;49(6):507–24. [CrossRef]
[Pubmed]

2.
Wong CA. Nerve injuries after neuraxial anaesthesia and their medicolegal implications. Best Pract Res Clin Obstet Gynaecol 2010;24(3):367–81. [CrossRef]
[Pubmed]
3.
Gruzman I, Shelef I, Weintraub AY, Zlotnik A, Erez O. Puerperal ventral epidural hematoma after epidural labor analgesia. Int J Obstet Anesth 2017;31:100–4. [CrossRef]
[Pubmed]
4.
Boutros N, Saba D, Trikamji B. Postpartum sciatic neuropathy after uncomplicated vaginal delivery. Neurohospitalist 2023;13(4):429–33. [CrossRef]
[Pubmed]
5.
Sahai-Srivastava S, Amezcua L. Compressive neuropathies complicating normal childbirth: Case report and literature review. Birth 2007;34(2):173–5. [CrossRef]
[Pubmed]
6.
Butchart AG, Mathews M, Surendran A. Complex regional pain syndrome following protracted labour*. Anaesthesia 2012;67(11):1272–4. [CrossRef]
[Pubmed]
7.
Radawski MM, Strakowski JA, Johnson EW. Acute common peroneal neuropathy due to hand positioning in normal labor and delivery. Obstet Gynecol 2011;118(2 Pt 2):421–3. [CrossRef]
[Pubmed]
8.
Saw JL, Hale J, Madhavan A, Ringler MD, Toledano M, Naddaf E. Ischiofemoral impingement syndrome provoked by labor: An unusual case of complete sciatic mononeuropathy. Neuroradiol J 2023;36(1):116–8. [CrossRef]
[Pubmed]
9.
Dahl V. Is the epidural analgesia to blame when it comes to neurological complications following labor? [Article in Norwegian]. Tidsskr Nor Laegeforen 2001;121(13):1587–90.
[Pubmed]
10.
Qublan HS, al-Sayegh H. Intrapartum common peroneal nerve compression resulted in foot drop: A case report. J Obstet Gynaecol Res 2000;26(1):13–5. [CrossRef]
[Pubmed]
11.
Kim SH, Kim IH, Lee SY. Sciatic neuropathy after normal vaginal delivery: A case report. J Clin Neurosci 2020;72:480–82. [CrossRef]
[Pubmed]
12.
Vijayan S, Arun Babu T. A case of bilateral foot drop following uncomplicated vaginal delivery: A case report and review of literature. Amrita Journal of Medicine 2021;17(2):63–5. [CrossRef]
13.
Hakeem R, Neppe C. Intrinsic obstetric palsy: Case report and literature review. J Clin Diagn Res 2016;10(4):QD06–7. [CrossRef]
[Pubmed]
14.
Whiles E, Shafafy R, Valsamis EM, Horton C, Morassi GL, Stokes O, et al. The management of symptomatic lumbar disc herniation in pregnancy: A systematic review. Global Spine J 2020;10(7):908–18. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
Perplexity artificial intelligence (AI) tool was used to check for spelling and grammatical errors.
Author ContributionsJennifer Law - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Alexandra Zilber - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Meghan Cox-Pedota - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Jennifer Law et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}