 |
Case Report
A tale of two laparoscopies: Diagnosing and treating a challenging case of interstitial ectopic pregnancy
1 East Sussex, Brighton South England, UK
2 District Headquarters Hospital Attock, Pakistan
3 University Hospital Sussex NHS, UK
Address correspondence to:
Aima Athar
East Sussex, Brighton, South England, BN2 5BE,
UK
Message to Corresponding Author
Article ID: 100229Z08AA2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Athar A, Khanum W, Ajala T. A tale of two laparoscopies: Diagnosing and treating a challenging case of interstitial ectopic pregnancy. J Case Rep Images Obstet Gynecol 2026;12(1):38–44.ABSTRACT
Introduction: Interstitial ectopic pregnancy (IEP) is a rather uncommon but potentially life-threatening type of ectopic implantation with a high-risk of delayed diagnosis and severe morbidity of the mother. It is usually complicated by the presence of typical clinical presentation and inconclusive early-term imaging, which makes it difficult to detect timely.
Case Report: We describe the case of a female, aged 26 years, who reported at six weeks of gestational age with intermittent abdominal pain at the lower part and increased β-hCG levels. The first transvaginal ultrasound was unable to localize the pregnancy and laparoscopy performed initially was inconclusive. The continued symptoms and the increasing level of the β-hCG stimulated additional investigation by use of the magnetic resonance imaging, MRI, which revealed a lesion typical of interstitial ectopic pregnancy. A second laparoscopy made the diagnosis and allowed surgical resection. Because of the persistent β-hCG postoperative, adjunctive methotrexate treatment was given with total resolution.
Conclusion: The case raises the issue of the complexity of diagnosis of interstitial ectopic pregnancy, especially in patients whose pelvic anatomy is altered. It highlights the value of keeping a high level of suspicion, the supplementing nature of MRI in cases where investigations within the first stage are inconclusive and the value of a combination of surgical and medical treatment in the final results.
Keywords: β-hCG, Diagnostic laparoscopy, Interstitial ectopic pregnancy, Intramural pregnancy, Methotrexate, Minimally invasive surgery
Introduction
The ectopic pregnancy poses a major maternal morbidity growth in the world with an interstitial ectopic pregnancy being one of the hardest forms to detect [1]. Interstitial ectopic pregnancy; in this case, the implantation is located in the interstitial segment of the fallopian tube through which it enters the myometrium, and then the uterine cavity. Interstitial pregnancies may be viewed as having a relatively low frequency of about 2–4% of all ectopic pregnancies, but they carry an inordinately high level of mortality, with level being due to the myometrial vascularity surrounding them and slower rupture [2].
In contrast to ampullary or ischial ectopic pregnancies, interstitial ectopic pregnancies can continue to advance to a rupture and can have a later onset and cause less specific symptoms [3]. The delay in diagnosis is frequent, especially in the case of early gestation, because imaging results can be inconspicuous or misleading. Although a Transvaginal ultrasound is the first-line imaging modality, it might not clearly outline interstitial implantation, particularly in patients who have a distorted pelvic anatomy due to prior surgical operations [4].
Interstitial ectopic pregnancy can be treated using management techniques such as surgical intervention, medical therapy using methotrexate, or both. Treatment options are based on gestational age, ectopic mass size, hemodynamic stability, reproductive desires, and regional experience. The case in point exemplifies the difficulties of the situation when the usual diagnostic pathways are ineffective and demonstrates the significance of the repeated examination, sophisticated imaging, and the staged intervention.
Case Report
A 26 years old, female patient presented herself at six weeks of gestational age with a six-day history of mild to moderate intensity lower abdominal pain. It was a spontaneous pregnancy and she was not using birth control. She did not have any related symptoms like vaginal bleeding, syncope, or hemodynamic instability. She has a surgical history of a right salpingo-oophorectomy in 2018 because of a large mucinous cystadenoma and drainage of a pilonidal abscess in 2023. She had normal colonoscopy in 2015 due to per-rectal bleeding, and history of acute psychiatric disturbance in 2023, which was managed in specialist care. She complained of regular menstrual cycles and denies any intermenstrual or postcoital bleeding.
Upon investigation, the patient was hemodynamically stable. Abdominal examination—slight tenderness of the lower abdomen with no guarding or rebound tenderness. Both the speculum and bimanual examination were insignificant, and there was no cervical movement tenderness or palpable adnexal masses. The preliminary lab tests revealed a steady hemoglobin level. Serial β-hCG shows that it increased more than twofold in 48 hours. Whereas transvaginal ultrasound was unable to detect an intrauterine gestational sac, a small hyperechoic mass was present near the right lateral uterine wall and this made the diagnosis of an ectopic pregnancy likely though the exact location was not clear.
Case Presentation
Patient History
The patient is a 26-year-old female without a history of pregnancy who was taken to the hospital six days ago with a history of lower abdominal mild to moderate intensity pain at approximately six weeks of pregnancy. The pregnancy has been unplanned, with the patient not using any contraceptives. None had been reported to have any vaginal bleeding, syncope, or hemodynamic instability. Her body mass index (BMI) is 33 kg/m2 with prior laparoscopic right salpingo-oophorectomy due to large ovarian cyst (33 cm mucinous cystadenoma) in 2018 and drainage of a pilonidal abscess in 2023. The results of her last colonoscopy, in 2015, were normal—done to investigate recurrent per-rectal bleeding and she had an acute change of behavior in 2023, which required treatment under psychiatric care.
Her last colonoscopy examination was carried out in 2015 was normal, and this time due to recurrent per-rectal bleeding. She experienced a case of acute psychiatric distress (suspected acute psychosis), in 2023, having a specialist psychiatric basis of treatment. Her gynecological history revealed that she had continued normal menstrual cycle with no intermenstrual, or post-coital bleeding.
Clinical Examination
It was found that the patient was hemodynamically stable. A computed tomography (CT) examination of the abdomen indicated mild lower abdominal tenderness in the absence of guarding and rebound. No distinctive cervical motion tenderness and palpable adnexal masses, bimanual and speculum, no significant findings.
Laboratory Investigations
The initial lab tests provided showed a stable hemoglobin level. The indication of a tendency to increase the levels more than twice in 48 hours by serial β-hCG put the probability of abnormal pregnancy under doubts.
Primary biochemical analysis has shown rising concentration of β-hCG (β-hCG of human chorionic gonadotropin) that doubled within 48 hours. Such pattern usually is an indication of a viable intrauterine pregnancy; however, it does not eliminate the possibility that it is an ectopic implantation, particularly interstitial pregnancies which may appear to have apparently normal β-hCG kinetics during the early development stages. Such biochemical array has helped in creating ambiguity in diagnosis at the early stages of evaluation.
Imaging/Paraclinical Findings
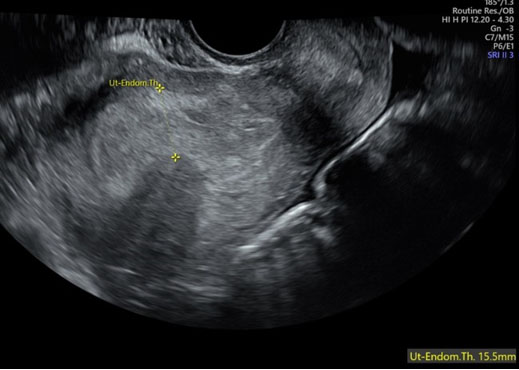
An intrauterine gestational sac could not be found in a transvaginal ultrasound (Figure 1). However, it was found that there was a small hyperechoic mass of approximately 10 × 16 × 13 mm in the vicinity of the right lateral uterine wall and this created suspicions of an ectopic pregnancy though the actual location was not clear.
The presence of an absent intrauterine gestational sac was identified in the imaging modality employed as the first-line in the suspected ectopic pregnancy transvaginal ultrasound. The absence of an intrauterine pregnancy at β-hCG levels exceeding the discriminatory zone caused one to suspect an ectopic pregnancy. There was a hyperechoic small mass located contrary to the right lateral uterine wall, but its anatomical location was unable to be well established. Prior right salpingo-oophorectomy was also a confounding factor with regard to interpretation since the remaining tubal tissue and adhesions in the aftermath may appear or conceal ectopic pathology.
An interdisciplinary assessment that included gynecological radiologists played a great role in the development of diagnosis. Magnetic resonance imaging (MRI) was chosen because of the better soft tissue contrast and the capability to define myometrial architecture. The MRI shows a focal lesion, which is in the right superior myometrium with high T2 signal intensity, which highly informs about the presence of interstitial or intramural ectopic pregnancy. Absence of fetal parts did not exclude the diagnosis since at the early stage of pregnancy the interstitial pregnancies may not give any embryonic structures.
Diagnostic Assessment
The case analysis above shows that interstitial ectopic pregnancy is a complicated issue particularly in the very early pregnancy stage and in women having a deformed pelvic architecture. The patient did not experience any particular symptoms, i.e., lower abdominal pain occasional, not accompanied by vaginal bleeding, hemodynamic disorientation. This is not a rare clinical manifestation in early ectopic pregnancy and can also manifest itself in the same manner as a normal early intrauterine pregnancy or threatened miscarriage thus clinical diagnosis is not a secure system.
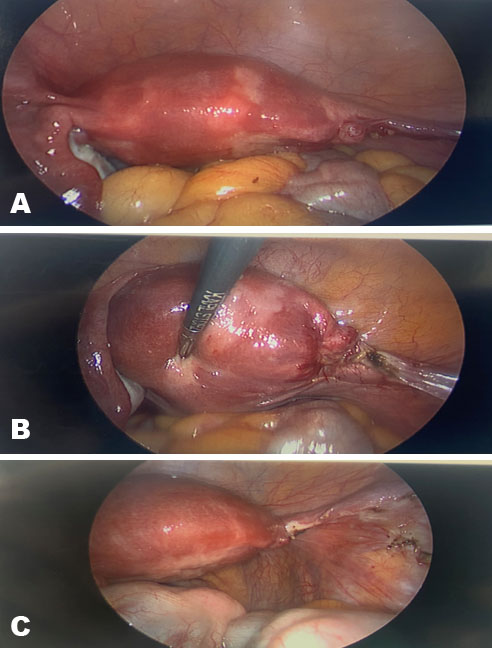
Since the pain is getting more severe in the abdomen of the patient, even though he is stable at the hemodynamic level, a diagnostic laparoscopy was adopted. Laparoscopy has been added as a bonus to the diagnostic and therapeutic treatment of the ectopic pregnancy of unclear character and has directly observed the structures of the pelvic cavity. In the present case, laparoscopy showed the remnant of the right fallopian tube without any visible ectopic pregnancy in the tubal remnant, in the uterine cornu and adnexa (Figure 2). The fact that the detection of the ectopic tissue was not possible during the operation was one of the key problems of the diagnosis and was the cause of the risk of the premature diagnosis conclusion.
Pathological studies of endometrial curettage demonstrated the presence of late secretory endometrium that contained no products of conception, all but eliminating the change of an intrauterine pregnancy, but not localizing the ectopic site. The reason why to re-assess the initial results and justify the need to administer further tests was the persistent rise of β-hCG in the postoperative period and the rise of the abdominal pains.
The line of diagnostics path above highlights the importance of high index of suspicion particularly where the course of the disease is not correlated to the biochemistry results and the initial diagnosis following the operation. It also emphasizes the role of quality imaging and multidisciplinary collaboration in the eradication of the complicated diagnostic dilemma in early pregnancy.
Management and Outcome (Therapeutic Intervention + Follow-up)
The medical treatment of the interstitial ectopic pregnancy should also be very keen of the gestational age, stability of the patient, the reproductive desires, and expertise. The chronic symptoms, rising concentrations of β-hCG and variable appearances of the diagnostic sensitivity affected the judgments of the management in this case.
Following an MRI which showed a possible existence of an interstitial ectopic pregnancy, the patient was informed concerning the available treatment provisions. Conservative medical therapy by use of systemic methotrexate was also a possibility, but due to the increasing pain that the patient was experiencing, increasing levels of β-hCG, and the uncertainty surrounding the diagnosis, surgery was considered the best intervention. The potential risk of uterine rupture and catastrophic bleeding of the interstitial pregnancies was also one of the factors that promoted the use of operative management.
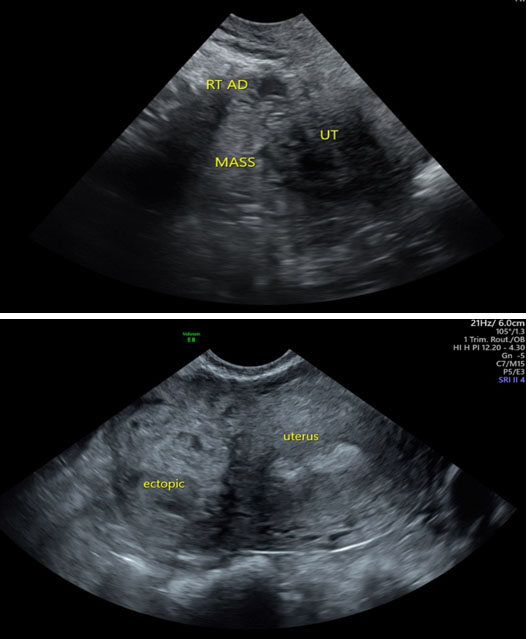
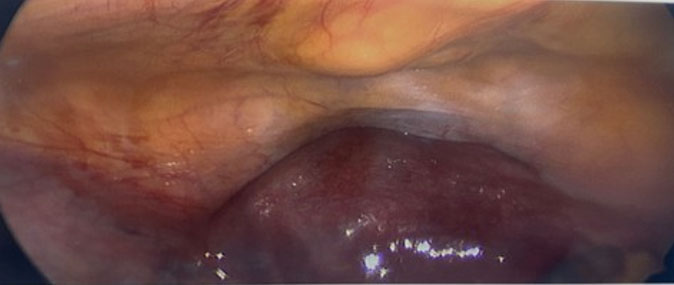
Better preoperative planning of LAP was done in repeat diagnostic laparoscopy. A consultant-led transvaginal ultrasound prior to surgery to increase localization in the operating room had proven the occurrence of an interstitial ectopic pregnancy with a circumferential hematoma (Figure 3). During laparoscopy, a mild protrusion was observed in the right posterior fundal region of the uterus and this corresponded with the observation of imaging.
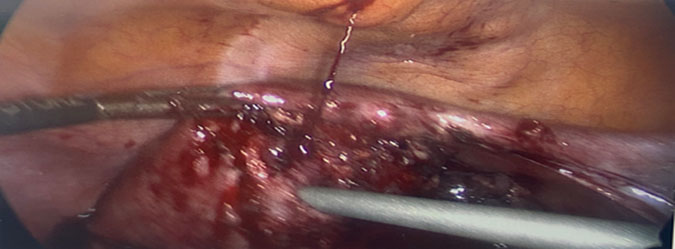
The intramyometrial carboprost (250 mcg) was done so as to assist in finding the location of the ectopic tissue more accurately and also to minimize the extent of bleeding during an operation (Figure 4). This pharmacologic treatment enhanced the intensity of contraction of the uterus and enhanced better demarcation of the ectopic mass to be removed. The patient had the interstitial pregnancy resected in harmonic shears to reduce thermal diffusion and spared the myometrial tissue surrounding. The enhanced hemostasis was achieved through the application of monopolar diathermy and topical hemostatic reagents, and figure-of-eight absorbable suture belted in the myometrium (Figure 5, Figure 6, Figure 7 ). The surgery of the two-layer myometrial defect closure was performed to assist in repairing the integrity of the uterus and the risk of uterine rupture in the future particularly in future pregnancies.
Surgical diagnosis was done using histopathological confirmation of products of conception. However, it was observed in the course of monitoring of postoperative period that the level of β-hCG suddenly increased following a reduction. This biochemical profile implied that there was chronic tissue of the trophoblast, which is a known complication post-surgery of the interstitial ectopic pregnancy by conservative surgery.
Based on these findings, adjuvant medical care of systemic methotrexate was done. This was a surgical-medical therapy, which would eliminate her residual trophoblastic activity with no extra invasive therapy. Serial levels of β-hCG recorded at intervals following administration of methotrexate indicated cumulative and gradual level-off reduction towards nearly negative levels, thus indicating that the treatment was effective.
Follow-up showed a patient who was stable and could not be clinically and the symptoms disappeared, and could not be followed by postoperative complications. A patient was also given a lot of advice about the necessity to carry out early ultrasound monitoring in further pregnancies and what it can leave to the fertility and integrity of the uterus.
The β-hCG postoperative monitoring showed a significant drop. However, there was an increment as experienced over the subsequent days, which revealed that there was presence of persistent trophoblastic tissue.
To identify a serious and consistent decline on β-hCG and the introduction of methotrexate treatment to approach negative concentrations. The patient was in her stable clinical state, and the abdominal pain was clear and no complications after surgery. The long-term follow-ups were in form of follies to monitor normalization of the levels of β-hCG; to provide advice regarding future pregnancies and early prenatal follow-ups.


Discussion
The interstitial ectopic pregnancy is still one of the most diagnostically challenging and clinically dangerous types of ectopic implantation [1]. This case demonstrates the multifactorial issues that are related to its identification and treatment, especially during early gestation and when the pelvic anatomy is altered. The late diagnosis of the patient in question highlights the shortcomings of the traditional diagnostic processes and Even though transvaginal ultrasound is the most common imaging modality used in cases of suspected ectopic pregnancy as a first-line imaging, the ultrasound has been identified to have limitations in identifying the presence of interstitial implantation [5]. The mildly hyperechoic mass near the uterine wall in this case demonstrates how early interstitial pregnancies may be wrongly classified or not come out clearly, especially in cases where pelvic surgery has been done, and the anatomy has been distorted. The patient’s history of right salpingo-oophorectomy likely contributed to diagnostic uncertainty and the initial difficulty in localizing the ectopic pregnancy during laparoscopy.
The first adverse diagnostic laparoscopy is a crucial learning aspect. Laparoscopy is still believed to be conclusive, but the interstitial ectopic pregnancy cannot be easily observed because of its internal location in the metropolis [6]. Here, no ectopic tissue was visible, and the provisional ruling out of ectopic pregnancy was done regardless of continuing symptoms and the increasing levels of β-hCG in the body. The following continuation of biochemical and clinical abnormalities was more than enough to provoke reassessment, which is why a negative laparoscopy could not be used as an argument to eliminate any further investigation in cases of high clinical suspicion.
Inclusion of magnetic resonance imaging became essential in solving the ambiguity in diagnosing. Magnetic resonance imaging (MRI) gave a better demarcation of the myometrial lesion, thus enabling proper localization of the interstitial ectopic pregnancy [7]. The case in question helps to verify the increased role of MRI as a useful supplement to ultrasound and laparoscopy in inconclusive results. Notably, the collaboration between radiologists and gynecologists was multidisciplinary and enabled the gynecologists to reinterpret the results as soon as possible, which led to subsequent management decisions [8].
Clinically, this scenario demonstrates the need to have tailored and gradual approaches to handling interstitial ectopic pregnancy. The symptoms, an increase in β-hCG levels, and a possible threat of uterine rupture led to the choice of repeat laparoscopy [9]. Intramyometrial carboprost perioperative also increased the clarity of the ectopic mass and is another example of an adjunctive pharmacologic agent that can help manage the conservative surgical outcome [10]. The meticulous removal of the interstitial pregnancy, sparing the uterine structure, can be considered a fertility-sparing technique that is suitable in a young nulliparous patient.
The ensuing secondary increase in the levels of β-hCG even after histopathological confirmation of full excision highlighted the danger of residual trophoblastic tissue after conservative surgery. The complementary use of systemic therapy in this biochemical pattern required adjuvant medical treatment using methotrexate. The effectiveness of combined medical and surgical treatment in selected cases is confirmed by the successful decrease in β-hCG after the administration of methotrexate [11].
In a more general clinical viewpoint, the case highlights why postoperative follow-up in interstitial ectopic pregnancy needs to be long-lasting. Monitoring of serial β-hCG is also critical because postoperative decreases might be inappropriate [12]. The fact that this patient did not respond immediately to the rise highlights the necessity of predetermined follow-up procedures that would help to identify the existence of a disease at an early stage to avoid complications in the late stages of the patient’s life.
Also, the case provokes significant deliberations concerning the fertility and obstetric outcomes in the future. Interstitial ectopic pregnancy management requires surgical intervention, with implications on uterine integrity, and good closure with multiple layers of myometrial closure was done in order to reduce the risk of uterine rupture in future pregnancies. In-depth counselling of patients on early pregnancy surveillance and delivery planning is thus a part of care.
The case has shown that interstitial ectopic pregnancy requires a high level of suspicion, an adaptable diagnostic approach and customized management routes. Clinical judgment, advanced imaging, repetitive surgical intervention, and adjunctive medical therapy played a critical role in ensuring a good outcome. This case provides important information about the nuances in the management of this rare but high-risk condition by illustrating the diagnostic pitfalls and therapeutic nuances observed during its management.
The importance of long-term clinical monitoring is emphasized in situations where biochemical, clinical, and radiographic data do not correlate [2].
The main peculiarity of the case was the seemingly promising initial β-hCG curve, which showed a pattern of more than doubling in 48 hours. Although this type of kinetics is generally related to viable intrauterine pregnancy, interstitial ectopic pregnancy can also display this characteristic of biochemical behavior during early development [3]. Trust in β-hCG trends can thus be deceptive and can also lead to diagnostic latitude. The discrepancy between the increasing β-hCG levels and the lack of an intrauterine gestational sac on the transvaginal ultrasound triggered further research in this patient, but failed to provide diagnostic clarity at once [4].
Conclusion
The interstitial ectopic pregnancy is a diagnostic and therapeutic dilemma, which demands a high index of suspicion, careful follow-up and multidisciplinary teamwork. The case shows that the continuing symptoms and the increase in the levels of β-hCG should be reconsidered even after negative surgical results. Developed imaging, recurrent intervention, and combined treatment approaches can result in positive outcomes with reduced maternal morbidity. The prognosis of this high-risk and rare condition, which is hard to predict, requires early identification and specific attention.
REFERENCES
1.
Atta J, Yousfani ZA, Das K, Rind G, Associate. Diagnostics and laparoscopic therapy for ectopic pregnancy [Internet]. [cited 2025 Dec 20]. [Available at: https://sjarr.com/wp-content/uploads/2021/12/1001.pdf]

2.
Stabile G, Romano F, Zinicola G, Topouzova GA, Di Lorenzo G, Mangino FP, et al. Interstitial ectopic pregnancy: The role of mifepristone in the medical treatment. Int J Environ Res Public Health 2021;18(18):9781. [CrossRef]
[Pubmed]
3.
Densley A, Shonnard M, Conklin M, Menghani V, Reddy-Moolamalla S. Angular and interstitial ectopic pregnancies: A clarification of terms and literature review. Curr Probl Diagn Radiol 2023;52(2):84–88. [CrossRef]
[Pubmed]
4.
Essebbagh Y, Errmili K, Lhaloui M, Mouimen S, Zeraidi N, Baidada A. Interstitial ectopic pregnancy: A rare challenged case report. Int J Surg Case Rep 2025;128:110938. [CrossRef]
[Pubmed]
5.
Kampioni M, Chmaj-Wierzchowska K, Wszołek K, Wilczak M. Interstitial ectopic pregnancy— Case reports and medical management. Medicina 2023;59(2):233. [CrossRef]
6.
Stabile G, Romano F, Buonomo F, Zinicola G, Ricci G. Conservative treatment of interstitial ectopic pregnancy with the combination of mifepristone and methotrexate: Our experience and review of the literature. BioMed Research International 2020;2020(1):1–7. [CrossRef]
7.
Durand YG, Capoccia-Brugger R, Vial Y, Balaya V. Diagnostic dilemma between angular and interstitial ectopic pregnancy: 3D ultrasound features. J Ultrasound 2022;25(4):989–94. [CrossRef]
[Pubmed]
8.
Slaoui A, Slaoui A, Zeraidi N, Lakhdar A, Kharbach A, Baydada A. Interstitial pregnancy is one of the most serious and uncommon ectopic pregnancies: Case report. Int J Surg Case Rep 2022;95:107195. [CrossRef]
[Pubmed]
9.
Lin TY, Chueh HY, Chang SD, Yang CY. Interstitial ectopic pregnancy: A more confident diagnosis with three-dimensional sonography. Taiwan J Obstet Gynecol 2021;60(1):173–6. [CrossRef]
[Pubmed]
10.
Bahall V, Cozier W, Latchman P, Elias SA, Sankar S. Interstitial ectopic pregnancy rupture at 17 weeks of gestation: A case report and literature review. Case Rep Womens Health 2022;36:e00464. [CrossRef]
[Pubmed]
11.
Ungureanu CO, Stanculea FC, Iordache N, Georgescu TF, Ginghina O, Mihailov R, et al. Ruptured recurrent interstitial ectopic pregnancy successfully managed by laparoscopy. Diagnostics (Basel) 2024;14(5):506. [CrossRef]
[Pubmed]
12.
Stabile G, Cracco F, Zinicola G, Carlucci S, Mangino FP, Stampalija T, et al. Subserosal pregnancy: Systematic review with proposal of new diagnostic criteria and ectopic pregnancy classification. Eur J Obstet Gynecol Reprod Biol 2024;297:254–9. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Aima Athar - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Wajiha khanum - Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Tosin Ajala - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthor declares no conflict of interest.
Copyright© 2026 Aima Athar et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}