 |
Case Report
Twin gestation with complete molar pregnancy and coexisting normal fetus: Case report
1 Fellow in High-risk Pregnancy, Obstetrics and Gynecology, Rainbow Children’s Hospital, Bangalore, Karnataka, India
2 Head of Department, Obstetrics and Gynecology, Rainbow Children’s Hospital, Bangalore, Karnataka, India
Address correspondence to:
Hansa Bharodiya
Rainbow Children’s Hospital, Marthahalli, Bangalore 560037, Karnataka,
India
Message to Corresponding Author
Article ID: 100230Z08HB2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Bharodiya H, Shenoi P. Twin gestation with complete molar pregnancy and coexisting normal fetus: Case report. J Case Rep Images Obstet Gynecol 2026;12(1):45–48.ABSTRACT
Twin pregnancy consisting of a complete hydatidiform mole with a coexisting normal fetus is an extremely rare obstetric condition and presents significant diagnostic and management challenges. These pregnancies are associated with markedly elevated β-human chorionic gonadotropin (β-hCG) levels and increased maternal risks including hemorrhage, preeclampsia, thyrotoxicosis, and development of gestational trophoblastic neoplasia. Early identification through ultrasound and biochemical markers is essential for appropriate counselling and management. A case of complete molar pregnancy with a coexisting fetus was diagnosed at 21 weeks during a routine anomaly scan. Termination of pregnancy was considered after detailed counseling due to maternal and fetal risk. Histopathological examination confirmed the diagnosis of a complete hydatidiform mole with a separate normal placenta. This case highlights the importance of antenatal imaging, multidisciplinary counseling, and close follow-up with serial β-hCG monitoring.
Keywords: ?-hCG, Coexisting normal fetus, Complete hydatidiform mole, Gestational trophoblasticdisease, Twin pregnancy, Ultrasound
Introduction
Gestational trophoblastic disease (GTD) represents a group of disorders characterized by abnormal proliferation of trophoblastic tissue [1] . Out of these, the most common is the hydatidiform mole. A complete hydatidiform mole results from androgenetic diploidy, typically caused by fertilization of an empty ovum by one sperm or by two sperms with an empty ovum, resulting in a 46XX or 46XY karyotype entirely of paternal origin [2]. Histologically, it is characterized by diffuse villous edema, cistern formation, and marked trophoblastic hyperplasia [3].
The coexistence of a complete hydatidiform mole with a normal fetus is extremely rare, with an estimated incidence ranging between 1 in 20,000 and 1 in 100,000 pregnancies [4]. These pregnancies are associated with significant maternal complications including severe vaginal bleeding, hyperemesis, preeclampsia, hyperthyroidism, and the risk of persistent gestational trophoblastic neoplasia (GTN) [1],[5]. Fetal survival is also poor due to placental insufficiency and associated complications [6].
Advances in prenatal ultrasound and genetic testing have improved the antenatal detection of such rare conditions [7]. However, management remains controversial and requires individualized decision-making based on maternal risk and patient preference [8]. We present a case of a twin gestation consisting of a complete hydatidiform mole and a coexisting normal fetus diagnosed in the second trimester.
Case Report
A 29-year-old primigravida presented for routine antenatal care at our tertiary care center. The pregnancy was achieved through ovulation induction followed by intrauterine insemination (IUI). Her first trimester screening, including a nuchal translucency scan, was reported as normal with appropriate nasal bone visualization and no structural abnormalities.
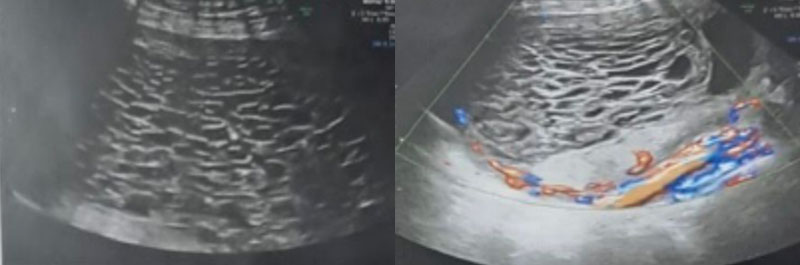
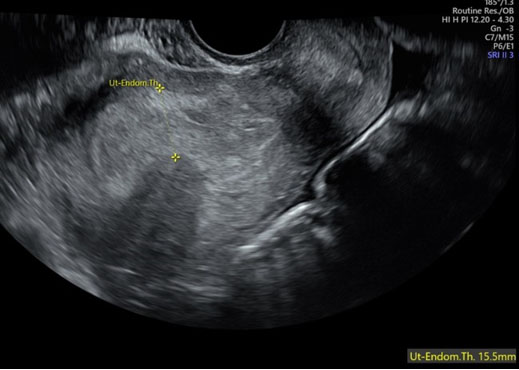
At 21 weeks’ gestation, she underwent a detailed anomaly scan. On detailed anomaly scan a single live fetus with normal biometry corresponding to gestational age and normal fetal heart activity seen. However, the placenta appeared enlarged, thickened with multiple cystic spaces (80% of placenta). A small portion of placenta appears normally posteriorly.
Color Doppler evaluation revealed increased vascularity within the abnormal placental tissue, consistent with trophoblastic proliferation. The amniotic fluid volume was within normal limits, and the umbilical cord contained three vessels.
Laboratory investigations revealed markedly elevated serum β-hCG levels exceeding 400,255 mIU/mL. Fluorescence in situ hybridization (FISH) testing confirmed a normal fetal chromosomal pattern. Based on these findings, a diagnosis of twin gestation with a complete molar pregnancy and a coexisting normal fetus was made.
The patient was counseled extensively regarding potential maternal and fetal risks associated with continuation of the pregnancy. Maternal complications discussed included severe hemorrhage, early onset preeclampsia, hyperthyroidism, and the risk of developing persistent GTN. After multidisciplinary consultation and detailed counseling, the patient elected to terminate the pregnancy.
Medical termination was initiated using misoprostol 800 mcg administered vaginally. The patient subsequently expelled a demised fetus along with placental tissue containing numerous vesicular structures characteristic of molar pregnancy. A separate normal placenta with intact membranes and umbilical cord was also delivered.
The expelled tissues were sent for histopathological examination. Gross examination revealed multiple translucent hydropic vesicles consistent with molar degeneration. Microscopic examination demonstrated hydropic chorionic villi with central cistern formation and diffuse trophoblastic hyperplasia confirming the diagnosis of a complete hydatidiform mole. The second placental specimen showed normal villous maturation with mild inflammatory changes.
Post-evacuation monitoring with serial β-hCG measurements was planned to exclude the development of persistent gestational trophoblastic disease.



Discussion
Twin pregnancy with a complete hydatidiform mole and a coexisting fetus is a rare but clinically significant condition within the group of gestational trophoblastic disease. The pathophysiology involves the simultaneous presence of a normal fertilized ovum and a molar conception arising from an androgenetic genome. Ultrasound plays a crucial role in early identification. Typical sonographic findings include a multi-cystic placental mass with absence of fetal tissue within the molar component, alongside a separate gestational sac containing a viable fetus. Doppler imaging often demonstrates increased vascularity due to trophoblastic proliferation.
Maternal complications are common and can be severe. Elevated β-hCG levels contribute to clinical manifestations such as hyperemesis gravidarum, hyperthyroidism, and early onset preeclampsia. Hemorrhage is also a frequent complication due to abnormal placental vasculature. Additionally, patients with molar pregnancy carry a risk of developing GTN, necessitating long-term follow-up.
The prognosis for the coexisting fetus varies widely. Some reports describe successful continuation of pregnancy resulting in live birth, but overall fetal survival rates remain low. Maternal health considerations often influence decisions regarding pregnancy.
Management strategies should be individualized. Management depends on gestational age, maternal complications, fetal status, and patient preference. When pregnancy termination is chosen, careful monitoring with serial β-hCG levels is essential to detect persistent trophoblastic disease.
Our case highlights the importance of routine anomaly scanning in detecting rare placental pathologies and underscores the value of timely counseling in guiding clinical decisions.
Conclusion
Complete hydatidiform mole with a coexisting normal fetus is a rare and potentially life-threatening obstetric condition. Early recognition through ultrasound and biochemical evaluation is essential. Management requires individualized counseling with careful consideration of maternal risks and fetal prognosis. Histopathological confirmation and post-evacuation β-hCG surveillance are critical components of follow-up care.
REFERENCES
1.
Soper JT. Gestational trophoblastic disease. Obstet Gynecol 2006;108(1):176–87. [CrossRef]
[Pubmed]

2.
Berkowitz RS, Goldstein DP. Current management of gestational trophoblastic diseases. Gynecol Oncol 2009;112(3):654–62. [CrossRef]
[Pubmed]
3.
Sebire NJ, Fisher RA, Foskett M, et al. Histopathological diagnosis of hydatidiform mole. J Clin Pathol 2003;56(5):345–9.
4.
Sebire NJ, Foskett M, Fisher RA, et al. Risk of persistent trophoblastic disease and pregnancy outcome in complete hydatidiform mole with a coexisting fetus. Lancet 2002;359: 2165–6.
5.
Management of Gestational Trophoblastic Disease: Green-top Guideline No. 38 - June 2020. BJOG 2021;128(3):e1–27. [CrossRef]
[Pubmed]
6.
Braga A, Obeica B, Werner H, et al. Complete hydatidiform mole with a coexisting fetus: A systematic review. J Ultrasound 2017;20:211–8.
7.
Duggan PM, Seckl MJ, Newlands ES. Gestational trophoblastic disease: Clinical presentation and management. BJOG 2013;120:111–8.
8.
Suksai M, Suwanrath C, Kor-Anantakul O, Geater A, Hanprasertpong T, Atjimakul T, Pichatechaiyoot A. Complete hydatidiform mole with co-existing fetus: Predictors of live birth. Eur J Obstet Gynecol Reprod Biol 2017;212:1–8. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
We would like to sincerely thank Dr. Aruna for her valuable guidance and support throughout this case. We are also grateful to the patient for her cooperation and consent, which made this work possible. We extend our appreciation to the staff nurses for their dedicated care, assistance, and support during the management of this case. We acknowledge the use of ChatGPT (OpenAI, GPT-5.3) for language editing and manuscript structuring. All content was reviewed and approved by the authors.
Author ContributionsHansa Bharodiya - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Praveena Shenoi - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Hansa Bharodiya et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}